Trauma Care and Trauma Systems: Past, Present, and Future
Trauma Care and Trauma Systems: Past, Present, and Future
Donald D. Trunkey
“What experience and history teach is this – that people and governments never have learned anything from history, or acted on principles deduced from it.”
—George Wilhelm Friedrich Hegel (1832 Philosophy of History – Introduction)
THE PAST
According to Diamond (“Guns, Germs and Steel”) sometime after 13,000 BC, men began to domesticate animals and ceased to be hunter-gatherers in several parts of the northern temperate climate zones of the globe. The areas included China, India, the Middle East, the Mediterranean area, and meso-America. Accidents became common while working with domesticated animals and in building cities and settlements for people congregated together for protection and social amenities. As cultures developed and prospered, war became inevitable. This in turn led to the development of wound care. In this chapter, we will look primarily at those developments in our history, which led to present day trauma surgery. These include wound care, the concept of shock, resuscitation, analgesia/anesthesia, and antisepsis. As in medicine, the development of basic sciences in the last 500 years was also extremely important.
Trauma care antedates recorded history, and there are examples of anthropological findings showing trepanation of the skull dated to 10,000 BC. These skulls have been found in the Tigris-Euphrates Valley, along the shores of the Mediterranean, and in meso-America. It is most likely these operations were done for depressed skull fractures and possibly epidural hematomas. The surgery was most likely performed by priests or shamans within the various cultures. Some of the skulls show that the operation was done more than once; and there is ample evidence that there was success because there was healing of the man-made hole. There is also evidence that they were able to treat fractures and dislocations successfully by knitting of the bones.
The first example in recorded history of care of the wounded comes from the Sumerians, who most likely invented writing. They were overrun by the Akkadians in 2600 BC. Their language was rich in description of wounds, and they also left us with two ways to treat wounds: those that were survivable and those that were not. These were set down in the 282 Laws of King Hammurabi’s Code dating from about 1700 BC. Included in these codes are the laws concerning doctors. Interestingly, the code did not hold the physician responsible unless he used his knife. There is no mention of a “surgeon,” and medicine was dispensed by an “ashipu” or sorcerer. There was reference to an “asu” or physician. Unfortunately, the former evolved into the primary practitioner. Knowledge of anatomy and physiology was essentially nil. The concept of shock did not exist, and wounds were treated with a bandage and soothing oil. There was a rudimentary understanding of inflammation and fever.
There was a commonality in early cultures to use poultices of various plant extracts, resins, and spices. Although this was probably used on an empiric basis, it may have had a serendipitous result. In 1943, around 2,300 species of medicinal plants belonging to 166 families were studied in Oxford. Plants of 28 families were active against Staphylococcus aureus, Escherichia coli, or both. Plants undoubtedly developed these components through evolution as protection to bacteria and fungus. Resins and spices were undoubtedly used on wounds to make them less malodorous.
Almost concomitant with the development of writing in Mesopotamia was the rise of culture in the Nile valley. The three medical papyri—Kahun Papyrus, Smith Papyrus, and Ebers Papyrus—are rich sources of Egyptian medicine. In addition, archeological findings show that fractured limbs were set by means of splints and bandages. Mass graves from 2000 BC show bodies of six soldiers, which are preserved well enough to show mace wounds, gaping wounds, and arrows still imbedded in the bone. Fractures were common with 1 out of every 32 individuals from 6,000 skeletons showing callous formation. Bites were common, including those from hippopotamus, lion, and crocodile. As near as can be determined, there was no word for “surgeon.” The physician or swnw dispensed pharmaceuticals and occasionally would take to the knife.
Probably the most famous early writing is the Breasted interpretation of the Smith Papyrus. It is the most ancient medical text. One of the more interesting aspects of the Breasted rendition is that surgical cases are divided into three categories, depending on the chances of successful treatment—an ailment which I will treat, an ailment which I will contend, and an ailment not to be treated. Wounds were bandaged or held together by thorns and stitches. The use of the cautery was advocated for wounds of a vessel. Abscesses were treated by “fire-drill.” Wounds were also treated with fats and oils, and fresh meat was used as a “poultice.” Poultices were also made out of plants, including the leaves of a willow tree, which contain a small amount of salicin (aspirin). The Egyptian physician could also use the extract of the opium poppy to control pain. Green pigment was extracted from malachite and chrysocalla, which contains copper, and was used in wound dressings. Copper is a toxic bactericidal. Wounds were treated with lint, with honey and grease incorporated into the dressing. One of the interesting aspects of Egyptian “medicine” was that of embalming. It is most likely they buried the body under their all-purpose natural soda—natron. This is a mixture of sodium carbonate and bicarbonate, with a few impurities. When mixed with fats, natron acts as a mild detergent and is very effective in drying out the corpse.
The Greeks were the first to develop a trauma system. In Homer’s Iliad, there are 147 recorded wounds, with an overall mortality of 77.6%. Thirty-one soldiers sustained wounds to the head, all of which were lethal. The Greek physicians recognized the need for a system of combat care, and the wounded were given care in special barracks, klisiai, or in nearby ships. Wound care was primitive; arrowheads were removed by enlarging the wound with a knife or by pushing the arrowhead through the wound. Drugs, usually derived from plants, were applied to these wounds, which were then bound, and hemostasis was treated by an epaoide. This meant that someone sang a song or recited a charm over the wound. Fractures were splinted, and the Greeks had nine methods of reducing dislocation of the upper and lower extremities. There is also evidence that the Greeks used opium to reduce pain and possibly for anesthesia.
In the Hippocratic Collection, there are numerous surgical treatments. The Greek language ignored the word cheriorugos, which meant “physician” including the verb cheirugein, which meant “to work with the hand.” Hemorrhage was treated with a towel dipped in cold water and wrapped around the wound. After the hemorrhage was controlled, the wound was wrapped in a white bandage soaked in red wine. In addition, the juice of the fig tree was also used to stop bleeding. Another method that surely did not work was bleeding the patient. This was done usually by cutting a vein above the hemorrhage. In the Hippocratic Collection, it states, “Hemorrhage kills, but bleeding helps.” Unfortunately, bleeding became a common treatment and persisted until just before the Civil War. It is interesting that the Hippocratic Collection also documents that ligature of bleeding vessels was not yet known, and the use of a tourniquet was condemned, which was reinforced by a Roman Scribonius Largus, who showed in experiments with a skin bag that if you tied a tourniquet around it, it forced more fluid out of the skin bag. The conclusion was that this made the bleeding worse. Drainage of abscesses was common, including empyema of the chest. Lacerations were treated by closing them with stitches threaded onto a bronze needle, and after the wound was closed, it was covered with a mixture of copper oxide and honey. Wounds to the head were bandaged if they did not involve the bone. The Greeks had at least three types of bone drills (trypanon). Trephination was used for fractures of the calvarium.
The Hippocratic Collection also puts forth their understanding of physiology, which were the four humors: blood, yellow bile, phlegm, and black bile. This was to persist for the next two millennia. They also felt that in nature everything is balanced. “Too much” or “too little” causes an imbalance, which is disease. The four humors were supposed to be harmoniously mixed, and disease ensues if they are unmixed or in wrong proportions. This also explained why the Greeks would bleed a patient even when they were hemorrhaging. They also thought that pus actually prevented more dangerous complications. In order to encourage the formation of pus they would, in some instances, insert greasy wool into the wound to help it suppurate. Paradoxically, they also understood that some wounds healed best if suppuration did not occur. Therefore, they would often put in powders of lead oxide and copper oxide to prevent suppuration. They also used moist solutions that had antiseptic properties, such as white vinegar, honey, sodium carbonate, and alum.
Some of the Greek pharmacy actually caused more harm than good. This included the side effects of poisoning with hellebore, which came from the Christmas rose. This would often raise blisters on the skin and invoke vomiting and diarrhea, and occasionally delirium, muscle cramps, and asphyxia. Purging the patient was considered necessary for them to survive.
There was undoubtedly intercourse between Greece and Egypt and exchange of medical ideas. Neither culture knew how to amputate. Wound dressings and suturing techniques were remarkably similar. Wine and honey were used in dressings. Vinegar was used as an antiseptic.
Several thousand miles to the east, in Asia, medicine was flourishing, but in quite a different way than that of Greece and Egypt. During the Chou Dynasty, which lasted from 1030 to 221 BC, several books, including the Huang Ti Nei Ching, the I Ching, were written; the latter was primarily a medical text. Surgery was discouraged, and physicians were admonished not to use medicines when “an illness occurred through no fault of your own.” It was thought that such an illness would “pass of itself.” Another medical text, Chou Li, is important because it further denigrates the status of surgery. It was thought that they were limited to a small group of “third-rate graduates.” This is in direct contrast to China’s neighbor, India, where surgery was a noble art. It is noteworthy that the practice of medicine was a tightly organized state system. Physicians were graded according to their achievement, which was followed by regular examinations. These objective techniques for measuring the ability of a candidate were devised as early as the fourth century BC and slowly diffused to the west through Baghdad and the Islamic world. The practice of examining physicians, required in Sicily under the statute of Roger II, the Norman in 1140, was in all likelihood a reflection of these Chinese standards.
Chinese medicine, like Greek medicine, had a simple explanation of disease, but there were only two factors, the yin and the yang, compared to the four humors of Greek medicine. Acupuncture was a common form of treatment. The yang i means “ulcer physician.” The primary treatments were psychology (cure the spirit), diet, drugs, acupuncture, and clinical medicine (the latter being “treat the bowels, the viscera, the blood, and the breath”). Little is mentioned about surgery of wounds. Judicial castration was common, and these eunuchs often became members of the court, since they were unable to procreate. The Chinese also used dressings that contained resins and possibly derivatives from plants because these were very common in the medical pharmacopeia. There is no mention in these historical treatises about trauma systems. Shock must have been a concept because one of their herbs, ma huang, is the same compound as ephedra (ephedrine), which was used by the Romans. This treatment of shock may well have been passed from west to east or east to west along the Silk Road.
The Hindu culture arose approximately 1500 BC when the Aryans, who came from Persia, captured the original dark-skinned inhabitants of India. They brought with them a system of medicine that was eventually called Ayurveda or science life. As noted in the preceding text, in contrast to China, India treated surgery as a noble art. The Indus valley in the west was part of the Persian Empire, whereas the valley of the Ganges in the east was subdivided into many small kingdoms. Among the kingdoms of the east, Magadha was eventually to become the most powerful. The kings were allegedly converted to Buddhism by Buddha himself, and one of these was Ashoka III of the Maurya dynasty. It was Ashoka who developed a system of trauma care for his armies. Shortly after ascending the throne, Ashoka decided to invade Kalinga on his eastern border. During his conquest, he left behind a number of rock edicts, inscriptions carved into rock. One of these refers to hospitals and another edict refers to the “provision of comforts for men and animals.” In addition to the rock edicts, there is also a book associated with Ashoka’s dynasty: The Artashastra. This book clearly shows that Ashoka’s army had an ambulance service, with well-equipped surgeons and women to prepare food and beverages, and assist in bandaging the wounded. Sushruta may have lived just before Ashoka, and he describes in detail the care of wounds. If a person was wounded by an arrow, he would not go to the internist (rogahara) nor the poison expert (vishahara), but instead would go to the shalyahara, which meant “arrow remover.” This is the first historical mention of a doctor (diadya) who specialized in surgery. They had several ways of removing arrows, including pushing them on through, removing them in a reverse manner, or tying the arrow to a bent willow and then releasing the willow branch. The wounds were often plastered with a generous scoop of honey and ghee, and bandaged with a clean piece of linen. This was essentially the same as the salve of the Smith Papyrus. The shalyahara could also probe wounds when the arrow broke off, and for injured blood vessels they used the cautery. Like other medical practices, they also had to subdue demons, and they did so by burning incense sticks and making sacrifices of food. Postoperative nutrition was provided by giving barley powder in boiled water. Their understanding of physiology was hinged on the notion that 700 vessels originating in the umbilicus carried varying proportions of blood, wind, bile, and phlegm. For snake bites, the vaidya placed a ligature above the wound. He would then consecrate the wound with a mantra and might incise the wound with a knife.
The shalyahara was also an expert in reconstructive plastic surgery. Repair of ear lobes was common because of the placement of weighted earrings. Judicial removal of the nose, unfortunately, was also common, and Sushruta had a reconstructive method using a pedicle flap brought down from the forehead. The shalyahara also treated abscesses, including empyema of the chest. Fractures were common and were splinted, and wounds were sutured with thorns and an ingenious method was followed by using the pincers of ants, who once they clamped onto the wound were beheaded.
Initially, the Romans had no physicians at all. This was not due to ignorance, and Pliny explains it as, “It was not medicine itself that the forefathers condemned, but medicine as a profession…chiefly because they refused to pay fees to profiteers in order to save their own lives.” Two hundred years before Christ, they slowly adopted Greek medicine in Pliny’s Historia Naturalis. He details a number of folk remedies, some of which are still in use today. Fern is recommended for intestinal worms, and it is somewhat effective. Rennet, either from goat, hare, or deer is also used to coagulate or bind. It is Pliny who refers to ephedra, previously mentioned, used to staunch a patient’s hemorrhage. It is noteworthy that other vasoconstrictive drugs were used for the treatment of shock until 1964.
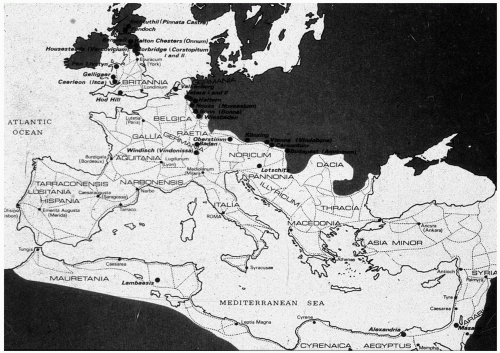
Celsus was another great Roman doctor. One of the great finds of antiquity was a copy of his De Medicina that was discovered in 1427 at the Basilica of St. Ambrose in Milan. Most of this work is based on the Hippocratic books. There are extensive sections in his book on human vivisection using criminals and gladiators. He condemned such practices. Celsus’ description of a surgeon captures the emotions of operating in an era of no anesthesia. “Now a surgeon should be youthful, or at any rate, nearer youth than age; with a strong and steady hand which never trembles, and ready to use the left hand, as well as the right; with vision sharp and clear, and spirit undaunted; filled with pity, so that he wishes to cure his patient, yet is not moved by his cries, to go too fast, or to cut less than is necessary; but he does everything just as if the cries of pain cause him no emotion.” Surgical instruments were many and specialized. Many of these have been found in the remains of Pompeii. Surgical knives, probes, and dilators, were most likely used for extracting barbed arrows. Celsus also recognized that patients who were wounded “should not die from hemorrhage or inflammation.” He treated hemorrhage by placing lint into the wound and then pressing down on the wound directly with his hand. If this did not check the hemorrhage, it was tried again, this time soaking the lint with vinegar. He also advocated ligature, and stated, “The veins that are pouring out blood are to be seized, and around the wounded spot, they are to be tied in two places.” Pompeiian forceps are remarkably similar to the bec de corbin that Ambrose Pare invented 1,500 years later. Wounds were sutured shut or closed with metal pins (fibulae). Wound plasters were also used and often contained copper acetate or lead oxide and resins. Celsus also described the signs of acute inflammation: rubor, tumor, calor, and dolor. It is most likely that this was copied from either an Egyptian medical treatise or Greek writings. Celsus also drew extensively on Indian medicine in creating his treatise on medicine. One of the more unique aspects of Roman medicine was the reintroduction of a trauma system by the Roman Army. In the first and second century AD, Roman generals provided special quarters, called valetudinaria, for the sick and wounded. At least 25 archeological remains of these valetudinaria have been found along the borders of the Roman Empire. Eleven of the trauma centers have been found in Roman Britannia, which is more than what currently exists (see Fig. 1). These hospitals for the wounded were very sophisticated. Open ventilation was stressed. Patient flow, including triage, was based on the seriousness of their wounds. Surgical instruments have been found in the remains, as well as unmistakable medicinal herbs. These include henbane (scopolamine) and dried poppies, which was undoubtedly used for pain management. The Roman army is known to have had surgeons because at least 85 army surgeons are recorded, mainly because they died and earned an epitaph. Some of their names are Greek: the majority is Latin.
A special mention has to be made about Galen because his writings would influence surgery for the next 1,500 years. Galen was a prodigious writer with 22 volumes still extant. At least one third of his writings have been lost. He was born in 130 AD in Pergamon, and at age 28, became surgeon to the gladiators. For 4 years, he cared for them, and according to his own writings, none of his gladiator patients died of their wounds. This is not true, because in his commentaries, he describes wounds of the heart. He stated, “They died faster if the wound reached into the left cavity. If the wound did not poke through, they could survive for up to 24 hours, and then they died of ‘inflammation.’” He did not understand the concept of shock, nor did he really appreciate the circulation although he could view the beating human heart.
One of the things that distinguished Galen was his interest in dissection. Remarkably, he dissected apes, horses, asses, mules, cows, camels, sheep, lions, wolves, dogs, lynx, stags, bears, weasels, mice, snakes, a variety of fish and birds, and several elephants. Unfortunately, he was also guilty of vivisection, and his favorite animal was the Barbary ape. Using vivisection, he worked out the relationship of cutting the spinal cord and the type of paralysis that it produced. While he was vivisecting pigs, he worked out the two nerves that controlled squealing. He found that if he cut the two recurrent nerves in the throat, the pig could no longer squeal. He misinterpreted the course and purpose of the recurrent nerves and stated that it was tension on the nerves that caused the voice box to move and not the muscles they innervated. In treating the wounded gladiators, he was the first to describe suture of tendons and muscle.
One of the more vexing issues surrounding Galen was his way of controlling hemorrhage. He had opened live animal vessels and found that they contained blood, not air, but he still did not understand the cardiovascular system. He did control bleeding from vessels, primarily by pressure and dressings. He also knew that if a vessel was grasped with a forceps or hook, then twisted, this would often control the bleeding. He noted if the vessel was seized with a forceps, it could also be tied, and he used silk ligatures obtained from silk dresses that were in vogue in Rome. He was also familiar with styptics and their ability to control superficial hemorrhage.
Following his time with the gladiators, he moved to Rome, where he spent 24 years and rose to the position of court physician to none other than Marcus Aurelius. This association was interesting because it was Aurelius who had sent a mission of merchants to China along the Old Silk Road, and this was how Chinese silk had been obtained.
As noted in the preceding text, Galen’s theories and management of wounds persisted for the next 1,500 years. It was not until the Renaissance that the flaws in some of his anatomic dissections and management of wounds were challenged, and in some instances, ridiculed. This condemnation, in my opinion, was too harsh because it failed to recognize his genius in starting the basic science of anatomy. His failure to make salient observations on physiology, and in particular the circulation, remains a mystery, and may in fact, be due to the loss of almost one third of his writings. Nevertheless, Europe slumped into the Dark Ages and feudal times. It was an era of itinerant surgery, quackery, and charlatans who practiced surgery with little or no training. It was also the time of burning of books, including the Egyptian alchemy books in Alexandria, which were burned by Diocletian in 292 AD. There was repeated destruction of the Alexandria library in 392 AD by Theodosius I and again in 640 AD.
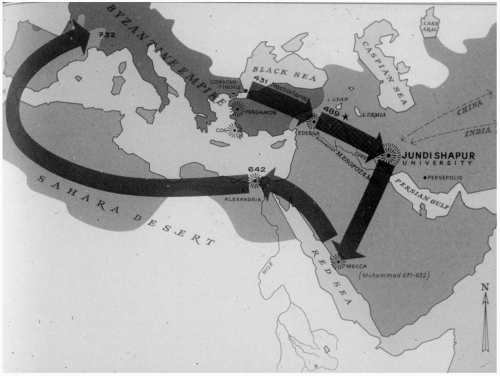
Many historians have argued that during the Dark Ages, the art and science of surgery did not advance. There are exceptions to this indictment. One of the reasons that Greek medicine survived through this dark period is in no small part due to the Nestorian epic. In 431 AD at the Council of Ephesus, Nestorius, who was the patriarch of Constantinople, was excommunicated for heresy. Nestorius disagreed with the conclusions of the Council of Nicaea, and did not accept the Holy Trinity. Nestorius was exiled and fled to Egypt, where he died probably in 451 AD (see Fig. 2). He took with him a number of books, some of which were burned by Theodosius II. His followers continued the exile to Edessa in upper Mesopotamia. From there, they found permanent asylum at Jundi Shapur University in Persia. The books carried by his followers were then translated into Arabic, and the university became a leading intellectual center, particularly in medicine. Ironically, most of the translations and scribing was done by Jewish scholars. The consequence of the Nestorian epic is that eventually these works made their way to Mecca, then back to Alexandria, and eventually across the crescent of North Africa into Spain, where the Moors reintroduced the historical record to the Byzantine empire. The second consequence was that Arab medicine reached a pinnacle during the years 700 to 900 AD, including the famous Arabic physicians Rahzes, Avicenna, and Albucasis. Unfortunately, the Arab physicians, like their Asian colleagues, looked down upon surgery as a second class of medicine. Using the books obtained from the Nestorians, they maintained Greek methodology and Galen’s surgery. This included treatment of fractures, reduction of dislocations, and use of the cautery and wound dressings which essentially remained the same. An exception was Rahzes, who practiced in the ninth century, and described the use of catgut for suturing wounds.
Another advance made before the Renaissance was the credentialing of physicians, and in particular, surgeons. Beginning in the thirteenth century, the School of Solerno, a secular university, sparked a resurgence of medical education. As noted earlier, Roger II of Italy adopted the techniques from China, which required examination and a license to practice medicine. This was soon followed by Frederick II, Emperor of the Holy Roman Empire. Surgeons were still treated as second-class citizens compared to physicians. This is beautifully documented by the Barber Surgeons in England, which eventually evolved into the Royal College of Surgeons. Across the English Channel in Paris, the same discrimination was carried out at the College of St. Côme. Paré was probably the most famous surgeon of the sixteenth century. He was not allowed to join the College of St. Cômeuntil he was 44 years of age. At that time, he was the court physician to King Henry II, but it was the friendship of Charles Etienne de la Riviere that made his membership possible. Etienne had been a dissector for the Faculté de Médicine and a Barber Surgeon. There were only two Barber Surgeons in the College of St. Cômewhen Pare was admitted. Ambrose Pare served four French kings during the time of the French-Spanish civil and religious wars. His major contributions toward treating penetrating trauma included his treatment of gunshot wounds, his use of ligature instead of cautery, and use of nutrition during the postinjury period. Paré was also much interested in prosthetic devices and designed a number of them for amputees.
A contemporary and acquaintance of Pare was Andreas Vesalius, who was to dramatically change surgery in the ensuing Renaissance. His dissections and interpretation corrected all of the mistakes that Galen had made. He also resurrected the treatment of empyema that had long been neglected. Pare and Vesalius attended to a very famous patient. Henri II was wounded on June 29, 1559 by a lance during a tournament. The lance struck the king above the right eye, and Pare was one of the surgeons in attendance. Vesalius was sent for from Brussels, but they were unable to ascertain the course of the splinters. The king died 11 days after the accident, and an autopsy showed a quantity of blood between the dura and the pia mater with early signs of infection.
It was in the seventeenth century that a major contribution to our understanding of the circulation was postulated by William Harvey. In 1628, Harvey published his seminal work, De Motu Cordis. Although one could surmise that the understanding of the circulation would lead to new concepts of shock, this did not occur until 290 years later. However, 28 years after Harvey’s discovery, Christopher Wren demonstrated that medicines could be administered to animals by the intravenous route. Ten years after his observation, Lower showed that homologous blood could be directly transfused between animals. Attempts to use blood transfusion in humans met with very disappointing results, complications, and death. The routine use of blood would have to wait until World War I. Between 1700 and 1900, there were major advances in the basic sciences. Morgagni was instrumental in developing the science of cellular pathology. John Hunter refined dissection and made major contributions to management of the wounds of war. Anesthesia was to be one of the major contributions to the surgical discipline. Ether was demonstrated by Crawford Long in 1842 and by William Morton in 1846 to be no “humbug.” A year after ether was introduced James Simpson demonstrated the effectiveness of chloroform, which became the primary anesthetic for the Confederates during the American Civil War. The nineteenth century was marked by the introduction of antiseptic surgery and the brilliant work of Louis Pasteur and Virchow were welcome additions to the basic sciences. Another major advance in the diagnosis of traumatic wounds was the invention of x-ray by Roentgen in 1895. Before this period, it was common to probe wounds. One reason to probe was to remove the missile if possible, the second was to determine the trajectory of the missile and predict what organs were injured. In many instances, probing caused more harm. X-rays essentially eliminated the need for probing wounds.
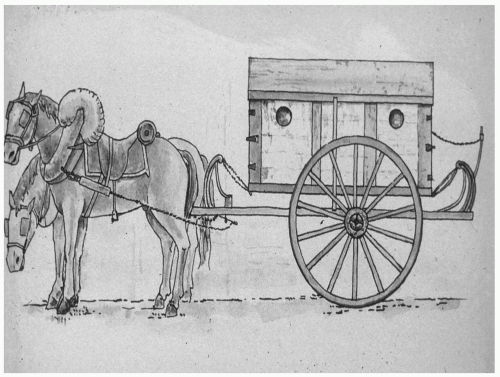
Figure 3 Larrey’s Flying Ambulance.
It was Dominique Larrey, Napoleon’s surgeon, who addressed trauma from a systematic and organizational standpoint. Larrey introduced the concept of the “flying ambulance,” the sole purpose of which was to provide rapid removal of the wounded from the battlefield. Larrey also introduced the concept of putting the hospital as close to the front lines as feasible in order to permit wound surgery as soon as possible (see Fig. 3). His primary intent was to operate during the period of “wound shock,” when there was an element of analgesia, but also to reduce infection in the postamputation period. He was a superb technical surgeon amputating the lower leg in 1.5 minutes and the upper arm in the same time.
Larrey had an understanding of problems that were unique to military surgery. Some of his contributions can best be appreciated by his efforts before Napoleon’s Russian campaign. Larrey did not know which country Napoleon was planning to attack, and there was conjecture about an invasion of England. He left Paris on February 24, 1812, and was ordered to Mentz, Germany. Shortly thereafter, he went to Magdeburg and then on to Berlin, where he began preparations for the campaign, still not knowing precisely where the French army was headed. In his own words: “Previously to my departure from this capital, I organized six divisions of flying ambulances, each one consisting of eight surgeons. The surgeons-major exercised their divisions daily, according to my instructions, in the performance of operations, and the application of bandages. The greatest degree of emulation, and the strictest discipline, were prevalent among all the surgeons.”
The nineteenth century may have been the century of enlightenment for surgical care in combat. This was partly because of better statistical reporting, but also because of major contributions of patient care, including the introduction of anesthesia. During the Crimean War (1853 to 1856), the English reported a mortality rate of 92.7% in cases of penetrating wounds of the abdomen, and the French a rate of 91.7%. During the American Civil War, there were 3,031 deaths among the 3,717 cases of abdominal penetrating wounds, a mortality of 87.2%.
The Crimean War was noteworthy in having been the conflict in which the French tested a number of local antiseptic agents. Ferrous chloride was found to be very effective against hospital-related gangrene, but the English avoided the use of antiseptics in wounds. It was also during the Crimean War that two further major contributions to combat medicine were introduced when Florence Nightingale emphasized sanitation and humane nursing care for combat casualties.
The Franco-Prussian War (1870 to 1874) was marked by terrible mortality and by the reluctance of some surgeons to use the wound antiseptics advocated by Lister. The mortality rate for thigh fractures was 65.8% in one series, and ranged from 54.2% to 91.7% in other series. Late in the conflict, surgeons finally accepted Lister’s recommendations, and the mortality fell dramatically. Antiseptic surgery remains a major contribution of the nineteenth century.
During the Boer War (1899 to 1902), the British advised celiotomy in all cases of penetrating abdominal wounds. However, early results were abysmal, and a subsequent British military order called for conservative or expectant treatment.
Although Larrey was the first surgeon to introduce systematic principles in care of injured people during war, the American effort during the Civil War on the Union and Confederate sides was remarkable. One of the most notable achievements was the publication of The Medical and Surgical History of the War of the Rebellion by the Union forces in six volumes. The only other national publications comparable with this were done by the French government in 1865 and the British government in 1854, 1855, and 1856 relating to the Crimean War (see Table 1). Although more soldiers died as a result of medical diseases than of penetrating injury, the overall death rate was staggering. The Union enlistments totaled 2,893,304 soldiers and the Confederacy enlistments were approximately between 1,277,890 and 1,406,180 soldiers. Of the 246,712 wounds resulting from weapons of war that were reported in the medical records, 245,790 were gunshot wounds and 922 were saber and bayonet wounds. The average Union mortality rate from gunshot wounds to the chest was 62% and for soldiers with abdominal wounds the mortality rate was 87%. Much of the organization for the Union effort is credited to Surgeon General William A. Hammond.
TABLE 1 CIVIL WAR DEATHS
Union
In battle
110,070
Disease
224,586
Accidents, suicides
24,872
Total
359,528
Confederacy
In battle
94,000
Disease
164,000
Total
258,000
Total Union and Confederacy
617,528
In one of the first reports of the war, Surgeon General Hammond showed that in a 4-month period (September to December 1862) soldiers with flesh wounds of the upper extremity had a very low mortality rate of 1.2% and soldiers with flesh wounds of the lower extremity had a mortality rate of 2%. In contrast, the mortality rate of soldiers with gunshot wounds of the humerus and upper arm was 30.7%; of the forearm, 21.9%; of the femur, 31.7%; and of the leg, 14.4%. These results were superior to those results reported for soldiers in the Franco-Prussian War, which was fought several years later. In addition to anesthesia, antiseptics were first used by Union medical officers predating Listerian surgery. There were at least three studies by Union surgeons during the Civil War documenting the effectiveness of antiseptics. In 1863, a study by Goldsmith showed that bromine reduced wound sepsis mortality to 2.6% in 308 patients with hospital gangrene. A comparable group of 30 patients in whom the antiseptic was not used had a 43.3% mortality rate. In 1864, Hackenberg reported to the Surgeon General that turpentine was effective in reducing hospital gangrene. In the third study by North in 1863, 60 patients with hospital gangrene had a mortality rate of 6.6%. North used “strong nitric acid.” Unfortunately, these antiseptics were not used routinely and hospital gangrene was a major cause of death.
From a systems standpoint, hospitals were organized along Department of Army organization. For example, at Gettysburg almost every division had its own hospital grouped according to Army corps. These hospitals were located strategically near creeks to provide much needed water. When there were numerous regimental hospitals in one battle, they banded together to form a brigade hospital. The next level of care was the division hospital, and finally the general hospital. Many general hospitals, such as Carver, Stanton, and Campbell were located in or near Washington, DC. The south had one very large hospital, Chimborazo, located in Richmond. James B. McCaw was the medical director. The hospital had 6,000 beds and treated 76,000 patients during the war. The hospitals in Richmond included Windsor, which had 5,000 beds, and Jackson with 2,500 beds. According to the United States Sanitary Commission, Jackson Hospital was considered a model of excellent care.
There were numerous other accomplishments during the Civil War including treatment of open wounds. The Sanitary Commission of the US Army issued a directive “it is good practice to leave the wounds open to heal by granulation.” Another accomplishment was the establishment of an ambulance corps. In September 1862, the Secretary of War, Stanton, directed Surgeon General William A. Hammond to form an ambulance corps. This was done under the guidance of Jonathan Letterman, who was at that time medical director of the Army of Potomac. One of the most important innovations during the Civil War was the introduction of nursing care modeled after that established by Florence Nightingale in the Crimean War. The Sanitary Commission was founded in 1861 primarily to assist the government in the care of the troops. The commission provided temporary shelters, clean bedding, wholesome food, and much needed nursing care. A leader in this movement was Clara Barton, who later founded the National Red Cross and the School of Nursing at Bellevue Hospital. In the South, Sally Louise Tompkins maintained the Robertson Hospital in Richmond, VA and was the only woman commissioned a Captain in the Confederate States Army.
The medical problems facing the surgeons of the Confederate States Army and Navy were not unique but were compounded by the lack of supplies and in some instances by poor administration. Similar to the surgeons of the Union Army, the surgeons of the Confederate Army had little or no training or experience in military medicine or surgery. The medical department of the regular Army of the new Confederate States of America was initiated by the provisional congress at Montgomery, AL on February 26, 1861. Unfortunately, the medical officers were indifferent toward the maintenance of surgical records and nothing comparable with the documentation of the Union Army exists. However, there is well-documented data from the organization and administration of the Confederate Medical Department. For example, the original measure of the Provisional Congress provided for a medical department consisting of one surgeon general, four surgeons, and six assistant surgeons. The surgeon general would receive an annual salary of $3,000; whereas the surgeon’s pay ranged from $162 to $200 per month and that of assistant surgeons ranged from $110 to $150 for the same period. Fleet surgeons received an annual stipend of $3,500, whereas a surgeon’s remuneration for the first 5 years after the date of his commission was set at $2,200 or $2,000, depending on whether he was on sea duty. As noted in the preceding text, medical and surgical supplies were often difficult to obtain, particularly after the Union blockade was imposed on British ships bringing in such supplies. In many instances, surgical supplies were obtained when Union troops were captured.
In addition to the hospitals in Richmond, numerous principal hospitals were established in the Confederate states: these included Virginia (39 hospitals), North Carolina (21), South Carolina (12), Georgia (50), Alabama (23), Mississippi (three), Florida (four), and Tennessee (two). There were Naval hospitals in Richmond, Charleston, Wilmington, Savannah, and Mobile. The first surgeon general was David C. DeLeon. He was relieved of duty shortly after appointment and after a 2-week temporary replacement he was replaced by Samuel Preston Moore who served as surgeon general for the duration of the war. Moore had significant problems appointing and maintaining an efficient corps of medical officers. Nevertheless, the surgical results were equal to or better than those achieved in the Union army, which was far better supplied.
Hospital gangrene was as much a problem in the South as it was in the North. Wards and even entire hospitals were fumigated, but this did little to reduce the gangrene and erysipelas. Patients were given sesquichloride of iron and quinine by mouth. In some instances, wounds were treated with nitric acid, turpentine, alum, nitrate of silver, sulfate and chloride of zinc, tincture of iron, tincture of iodine, yellow wash, and Darby’s solution. There was no unified treatment of wounds and the results varied from hospital to hospital. A particular blight on the confederate medical system was Andersonville prison, where hospital gangrene was rampant. The prison was established in 1864 to relieve some of the congestion associated with the prisons around the capitol of Richmond. There were only 13 doctors to care for 26,000 prisoners. Unfortunately, as Sherman and Grant began their stranglehold of Richmond and the march through Atlanta, the transportation and supply system deteriorated, which led to deprivation of food, medical supplies, and adequate housing for the prisoners. Of the 15,987 prisoners who were treated in Andersonville, 11,086 died.
The Union recognized the shortcomings of their organization of hospitals. The regimental hospital was not adequate to care for patients who were sick and injured. Furthermore, as the regiment moved on, they could not take the patients with them and it became necessary to establish independent hospitals that could receive the sick and wounded soldiers after the troops moved. These hospitals became known as general hospitals and were permanent. Furthermore, they provided an echelon of care where patients were evacuated from hospitals near the battle line back to safer areas and to hospitals that could provide additional definitive surgery and rehabilitation.
Between the Civil War and World War I there were very few advances in the development of trauma systems. The first report of civilian surgeons treating soldiers with gunshot wounds of the abdomen appeared as early as 1889 but represented cases (five patients of whom four survived) from 1881 to 1888. Nancrede reported three patients at the American Surgical Association meeting in 1887. Two of his patients died. Subsequent studies during the Spanish American War and the Boer War showed fairly abysmal results for surgical treatment of soldiers with abdominal gunshot wounds (see Table 2).
Relatively new technologic advances were designed and applied during World War I. Blood transfusions were used relatively extensively and to good advantage. Open treatment of contaminated wounds with delayed closure was accepted at the Inter-Allied Surgical Conference in March 1917. Motorized ambulances were employed, although care was often delayed by as many as 12 to 24 hours after injury. In this preantibiotic era, patients with wound sepsis were primarily treated with topical agents such as Dakin’s solution. A commission was appointed to study shock and resuscitation and from these studies, Cannon published his classical work. As many as 8,538,315 soldiers were killed in action or died of wounds or disease. The US military force numbered 4,734,991 men. The number of American soldiers who died in battle was 53,402; this was exceeded by the number of deaths from disease, which was 63,114 (see Table 3).
As noted previously, the concept of shock was not articulated until 290 years after Harvey described the circulation. Seventeenth and eighteenth century surgeons thought of shock in very prosaic terms. LeDran defines shock as “reflections drawn from experiences with gunshot wounds.” John Warren, another eighteenth century surgeon stated, “Shock is a momentary pause in the act of death”; and Samuel Gross thought that shock was “the manifestation of the rude unhinging of the machinery of life.” The seminal work on shock came in 1918 when Walter B. Cannon, based on a 3-month study of casualties at Clearing Station 33 during World War I, provided a definition of shock that is applicable even today. He stated, “Wound shock occurs as a consequence of physical injury. It is characterized by a low venous pressure, a low or falling arterial pressure, a rapid, thready pulse, a diminished blood volume, a normal or increased erythrocyte count and hemoglobin percentage and peripheral blood (thereby differing from simple hemorrhage), a leukocytosis, an increased blood nitrogen, a reduced blood alkali, a lowered metabolism, a subnormal temperature, a cold skin moist with sweat, a pallid or grayish or slightly cyanotic appearance, also by this, by shallow and rapid respiration, often by vomiting and restlessness, by anxiety, changing usually to mental dullness, and by lessened sensitivity.” Cannon classified shock into three groups: compensated, partially compensated, and uncompensated. Cannon recognized that all organs autoregulate in response to a shock insult, and he thought that if the blood pressure could be kept above 80 mm Hg, that was all that was necessary, and the patient could be taken to the operating room, and the hemorrhage controlled. He recognized that delay in operation increased the mortality dramatically. His description of shock is matched only by his intellectual and sound approach to resuscitation. To understand from a historical perspective, we need to return to the work started by Wren and Lower. Following this work, it was in 1831 that W. B. O’Shaughnassy treated patients who had diarrhea with fluid and electrolyte solution. This work was confirmed in 1850 by Karl Schmidt, but all these authors were essentially ignored. Between 1880 and 1882, Sidney Ringer showed that potassium was a normal constituent of physiologic fluids. Nine years later, Rudolf Matas reported success with intravenous fluid administration again for diarrhea and cholera. In 1915, three pediatricians described the chemical composition of diarrhea fluid as compared with normal stools in infants. Thirteen years later, Alexis F. Hartmann, another pediatrician in St. Louis, described the chemical changes in the body as the result of certain diseases and developed fluid therapy based on the 1915 work. He could not dissolve bicarbonate, therefore gave lactate as a replacement. He gave this to seven medical students, and they had no undesirable side effects. Six years later, it was used in children suffering from cholera and dysentery, with a remarkable reduction in mortality from 60% to 10%. The next major hurdle was to use blood. Work by Nuttal, identified the blood groups. Arthus and Pages showed that calcium was necessary for clotting, and Hustin described citrate anticoagulation. It was Robinson who used citrated blood for combat casualties in World War I. The next major advance was the work by Shires in 1964, where he showed that in severe shock there was depletion of the extracellular space above and beyond the predicted and measured loss of blood in patients. This physiologic concept had been predicted by Cannon, but Shires’ work showed conclusively with volume of distribution measurements the extent of the fluid loss.1,2 Another pivotal clinical study was done during the World War II in northern Italy in 1943. In soldiers with severe shock, blood volumes were obtained showing a straight line relationship between the loss of blood and the degree of fall in blood pressure. The pulse rate did not correlate with the fall in blood volume; however, the quality of the pulse and pulse pressure did decrease. Unfortunately, modern resuscitation uses blood components and several crystalloid solutions. Normal saline has been shown to be harmful, and recent evidence in Iraq again reestablishes the principle that whole blood and judicious use of electrolytes is the optimal choice for resuscitation.
TABLE 2 PERCENTAGE OF WOUNDED DYING OF WOUNDS (US ARMY)
War
Year
Number of Wounded
Percentage of Wounded Who Died of Wounds
Mexican War
1846-1848
3,400
15.0
American War between the States
1861-1865
318,200
14.0
Spanish-American War
1898
1,600
7.0
First World War (excluding gas)
1918
153,000
8.0 8.0
Second World War
1942-1945
599,724
4.5
Korean Conflict
1950-1953
77,788
2.5
Vietnam Conflict
1965-1972
96,811
3.6
TABLE 3 SURGICAL MORTALITY FOR HEAD, CHEST, AND ABDOMINAL WOUNDS (US ARMY)
War
Head
Thorax
Abdomen
First World War cases
189
104
1,816
Percentage of mortality
40
37
67
Second World War cases
2,051
1,364
2,315
Percentage of mortality
14
10
23
Korean Conflict cases
673
158
384
Percentage of mortality
10
8
9
Vietnam Conflict cases
1,171
1,176
1,209
Percentage of mortality
10
7
9
Between the Spanish American War and World War II surgeons in the United States began the foundations of modern trauma systems. In 1912, at a meeting of the American Surgical Association in Montreal, a committee of five was appointed to prepare a statement on the treatment of fractures. This led to a standing committee. One year later the American College of Surgeons (ACS) was founded, and in May 1922, the Board of Regents of the ACS started the first Committee on Fractures with Charles Scudder as chairman. This eventually became the Committee on Trauma. Another function begun by the College in 1918 was the Hospital Standardization Program, which evolved into the Joint Commission on Accreditation of Hospitals. One function of this Hospital Standardization Program was an embryonic start of a trauma registry with the acquisition of records of patients who were treated for fractures. In 1926, the Board of Industrial Medicine and Traumatic Surgery was formed. Therefore, it was the Hospital Standardization Program by the ACS, the Fracture Committee appointed by the ACS, the availability of patient records from the Hospital Standardization Program, and the new Board of Industrial Medicine and Traumatic Surgery that provided the seeds of a trauma system.
Between the two world wars, some significant advances were made in the development of trauma care for civilian patients. Böhler formed the first trauma care system for civilians in Austria in 1925. Although initially directed at work-related injury, it eventually expanded to include all accidents. Blood banking became routine and Fleming discovered penicillin in 1929. Unfortunately, excellent consistent trauma care remained elusive.
As with many wars, in World War II, lessons learned in previous conflicts had to be relearned. For example, it was necessary for Edward Churchill of Boston to go to the New York Times to publicize the shortage of blood before he could convince the War Department to provide blood in operating rooms (North Africa). In 1943, it was necessary for Major General Kirk to mandate that all military surgical personnel leave all amputation wounds open. Nevertheless, antibiotics made wound infections much less of a problem than in previous conflicts; finally Major General Ogilvie directed that all soldiers with colon injuries required colostomy. Transportation time for shifting the wounded soldiers from battalion aid stations to definitive care facilities was reduced to 4 to 6 hours with a subsequent reduction in mortality. Inadequately treated shock was still a problem and contributed to a high incidence of acute renal failure with attendant high mortality.
After World War II a serious attempt was made by the American Board of Surgery to form a new Board of Traumatic Surgery. This was mentioned in 1952, 2 years after the start of the Korean Conflict, and was considered at two subsequent meetings before it was abandoned.
Several advances in trauma system concepts were developed during the Korean Conflict. The introduction of air ambulances including helicopters reduced the time from injury to definitive surgical care to between 2 and 4 hours. Forward surgical hospitals (Mobile Army Surgical Hospital units) were introduced, which also reduced the time from injury to definitive surgical care. Vascular injuries were repaired, which reduced the number of amputations. Blood was used extensively, but unfortunately shock still remained a problem as did acute renal failure and the resulting high mortality.
Between the Korean Conflict and the Vietnam Conflict, many developments occurred that impacted heavily on the development of trauma care systems. The importance of ambulance services was addressed in a Scudder Oration by George Curry in 1958. Pioneer work by Moyer and Butcher, and Champion et al. led to the recognition that patients in shock lost more extravascular fluid into the intracellular space, explaining the high incidence of renal failure when not treated. This also confirmed the observations by Cannon during World War I.
The extensive use of helicopters in the Vietnam Conflict reduced the time from injury to definitive surgical care to <1 hour. By applying the resuscitation principles established by Shires, renal failure became an uncommon problem, but a new syndrome, Da Nang lung, became apparent. This reflected a misunderstanding of some of the principles espoused by Starling before World War I. Specifically, although crystalloid resuscitation was beneficial, overuse contributed to shock insult to the lung and reperfusion injury.
THE PRESENT
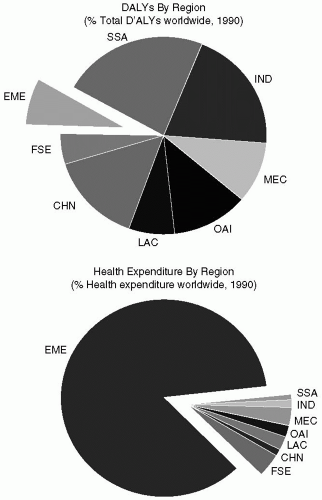
In order to set the stage for these next two sections, I would like to examine the impact of intentional and unintentional injuries on a worldwide basis. There is no better resource than the Global Burden of Disease Study by Murray and Lopez.3 In their study, they divided the world into developed and developing regions, and subcategorized the world into eight distinct economic regions (see Fig. 4). In 1990, 5 million people worldwide were estimated to have died from intentional and unintentional injuries. The risk of injury death varies strongly by region, age, and sex. If one compares mortality from violent causes, in the European market economies, injuries caused approximately 6% of all deaths in 1990, compared with 9% to 11% in other regions. It is particularly striking and problematic in sub-Saharan Africa and Latin America where 12% to 13% of deaths are related to violence. It is primarily a problem in men, where it accounts for 16% to 17% of deaths. Worldwide, road traffic accidents are the number nine cause of death. In developed regions, road traffic accidents are the number eight cause of death, and self-inflicted injuries are number nine. In developing regions of the world, road traffic accidents are number 10, and infectious diseases are number four, number six, number eight, and number nine (diarrheal diseases, tuberculosis, measles, and malaria).
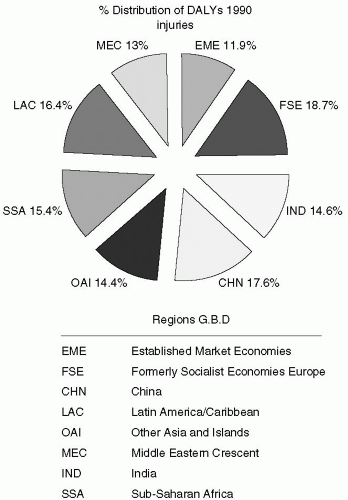
In an attempt to quantify the burden of disease and injury of various human populations, Murray and Lopez have used the concept of Disability Adjusted Life Years (DALY). A DALY is defined as the sum of life years lost due to premature mortality and years lived with disability adjusted for severity. This obviously gives us a different perspective of how injury impacts negatively on individual lives and societal costs. Worldwide in 1990, road traffic accidents were number nine as a cause of DALYs. In developed regions, the traffic accidents were the number four cause of DALYs, and self-inflicted injuries was number nine. In developing regions, road traffic accidents was number 11, war was number 16, violence was number 18, and self-inflicted injuries was number 19. Murray and Lopez conclude that injuries play a surprisingly large role in the burden of disease. Overall, it accounts for 14.5% of the burden in developed regions and 15.2% in developing regions. It is noteworthy that there is variability across the eight economic regions in the world (see Fig. 5).
Figure 4 Results from the Global Burden of Disease Study. Courtesy of World Health Organization (Murray CJL, Lopez AD. The global burden of disease. Harvard University Press for the World Health Organization; 1996).
The lessons learned in military conflicts of the twentieth century have been applied to trauma care of civilians. However, the evolution of trauma care systems for civilians was accelerated in 1966, with the establishment of two trauma centers in the United States.4 One of these trauma centers was started at San Francisco General Hospital under the leadership of William Blaisdell and the other was started at Cook County Hospital in Chicago under the leadership of Robert Freeark. The rationale for these two trauma centers was multiple. Titles 18 and 19 (Medicare and Medicaid) had just been introduced, and the old city and county hospitals were essentially without patients. At the same time, urban violence was on the rise, primarily as a consequence of the increase in urban ghettos and drug-related violence. The leaders of these two trauma centers recognized the need for a systematic approach to trauma care and the concept of a trauma center was pivotal to this overall need.
Figure 5 Distribution of DALYs 1990 within the eight economic regions of the Global Burden of Disease (Murray CJL, Lopez AD. The global burden of disease. Harvard University Press for the World Health Organization; 1996).
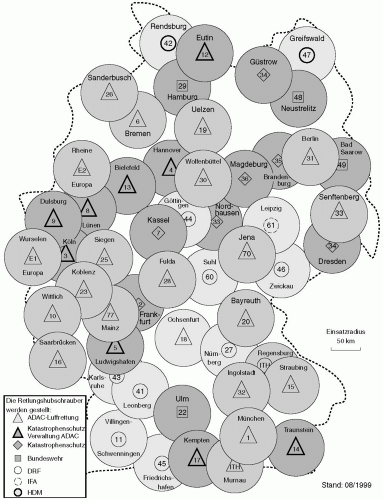
Shortly after these two centers were started, the political and administrative genius of R. Adams Cowley were combined when he established the Maryland system of trauma care, which eventually became a state-wide system. The most remarkable development of a state-wide trauma system occurred early in the 1970s in Germany.5 At that time, road traffic accidents accounted for 18,000 deaths annually. Since 1975, this has been reduced to approximately 7,000 (see Fig. 6).
One year later in 1976, the ACS Committee on Trauma developed a formal outline of injury care called Optimal Criteria for Care of the Injured Patient. Subsequently, task forces of the ACS Committee on Trauma met approximately every 4 years and updated their optimal criteria, which are now used extensively in establishing regional and state trauma systems. More recently, the ACS Committee on Trauma, working with the American College of Emergency Physicians, has developed some new guidelines for trauma care systems. Under the new model, the system of trauma care is inclusive rather than exclusive. In the old system, only patients who were injured severely were treated at a trauma center. Under the new system, all patients, including those with moderate and minor injuries, are part of the model trauma care plan. The model trauma care system cares for patients whether they are in an urban or a rural setting and the providers have been expanded to include teams and system management and prehospital care, trauma care facilities, and rehabilitation services. The components of this system include leadership; system development; legislation; finance; public information, education, and prevention; human resources; prehospital care with the subcomponents of communication; medical direction; triage and transport; definitive care, including the subcomponents of trauma facilities, interfacility transfer, and rehabilitation; and finally a quality improvement program that evaluates all of these components. Other contributions by the ACS Committee on Trauma include introduction of the advanced trauma life support (ATLS) courses, establishment of a national trauma registry (National Trauma Data Bank), and a national verification program. The latter is analogous to the old Hospital Standardization Program and verifies whether a hospital’s trauma center meets the guidelines of the ACS.
Since 1984, more than 20 articles have been published showing that trauma systems benefit society by increasing the chances of survival when patients are treated in specialized centers.6 In addition, two studies have shown that trauma systems also reduce trauma morbidity.7,8 In 1988, a report card was issued on the current status and future challenges of trauma systems.9 At that time an inventory was taken of all directors of state emergency medical services (EMSs) or directors of health departments who had responsibility over emergency and trauma planning. They were contacted by telephone in February 1987 and were asked eight specific questions on their state trauma system. Of the eight criteria, only two states, Maryland and Virginia, had all eight essential components of a regional trauma system. Nineteen states and Washington, DC, either had incomplete state-wide coverage or lacked essential components. Not limiting the number of trauma centers in a region was the most common deficient criterion.
Figure 6 Road traffic accidents in Germany [need more legend].
In 1995, another report card was issued in the Journal of the American Medical Association.10 This report card was an update on the progress and development of trauma systems since the 1988 report. It was a more sophisticated approach; it expanded the eight original trauma criteria and was more comprehensive. According to the 1995 report, five states (Florida, Maryland, Nevada, New York, and Oregon) had all the components necessary for a state-wide system. Virginia no longer limited the number of designated trauma centers. An additional 15 states and Washington, DC had most of the components of a trauma system.
Bazzoli upgraded her 1995 report card at the Salishan Conference in 1998.11,12 There are now 35 states that are actively engaged in meeting trauma system criteria. Many of these states have implemented their systems through Federal support of the Trauma Care Systems Planning and Development Act (Public Law 101-590). Although there has been constant growth and development of statewide trauma systems, there are still underserved areas in the United States, particularly in the rural areas. This is unfortunate because one study has shown conclusively that a state-wide trauma center makes a major difference in trauma outcome in rural areas once a trauma system has been established. Finally in 2006, a more definitive study evaluating the efficacy of trauma center care on mortality showed that the mortality from trauma was 7.6% in designated trauma centers compared to 9.5% in hospitals that were not designated.13 One year after discharge, the significance continued with a mortality of 10.4% versus 13.8%. This slight increase in the 1-year mortality most likely represents deaths in the elderly and late deaths from traumatic brain injury. Another study published in 2006 from Florida showed that in counties with a trauma center, the mean fatality rate was 50% less than in counties without a trauma center.14 It can be seen from this data that the effectiveness of a trauma center is irrefutable as shown by these two recent studies and the data from Germany.
The centerpiece for the Canadian trauma system is represented by the 17 medical schools in the various provinces. Designation of trauma centers is up to the province, and in several instances, there is more than one trauma center per major metropolitan area. Like the United States, Canada has some very rural areas, particularly the plains of the provinces of Central Canada and the Rocky Mountain West. Prehospital care in these regions can be prolonged despite common 911 number and prehospital aircraft rescue systems.
There have been some studies from the Montreal McGill University regarding prehospital care, not only in Montreal but also extending from Quebec into Ontario provinces.15,16 It was these studies that refuted the concept of trying to stabilize the patient at the scene and showed that physicians were not as effective as paramedics. At present, there is no country-wide designation and verification process. ATLS is taught to almost all eligible physicians, and critical care is provided both by surgeons and physicians.
A study from Mexico shows that 9 6% of seriously injured patients are transported to hospital by ambulance17. Fifty percent of the prehospital personnel are volunteers with little or no training; the remaining half has basic emergency medical technician training. In a 1999 study, it was shown that in some trauma centers in large cities that focused on care of the injured,18 interestingly, only a few of the general surgeon attendings had taken ATLS courses, and essentially none of the residents had had ATLS training. In this particular article, it was pointed out that the primary problem in having functional and designated trauma centers was the lack of funding and resource commitments. More recently, a study has been done comparing trauma care delivery in three areas within Mexico.19 They used as their guidelines the World Health Organization (WHO)’s Guidelines for Essential Trauma Care.3,4 The authors then did a study and evaluated these three areas by a “pre-review questionnaire” and a site-visit process. In total, five clinics, four small hospitals, and seven large hospitals were surveyed. The large hospitals averaged 1,000 to 9,000 trauma admissions annually. Using the WHO criteria, they showed that in the small hospitals, resources were extremely limited. They lacked pulse oximetry as an example. Large hospitals were fairly well supplied for acute resuscitation. However, most did report problems occasionally with blood supply. Using this study, which also looked at manpower, it was the intent of the investigators to show that the WHO criteria are reasonable, and using them would allow various Mexican states to improve trauma care. The WHO criteria will be discussed in more detail later in this section; nevertheless, some of the shortcomings are that the WHO lists specialists and tertiary care facilities in developing countries as “desirable” rather than as “essential”. This might include image intensification and angiography. It is noteworthy that they found that quality improvement is mandated by the Secretariat of Health for the larger hospitals. The quality of these programs was not studied in detail in this particular paper and does represent a departure from the verification visits conducted by the ACS. The most positive thing about this study is that it shows that Mexico is addressing trauma as a serious public health problem, and physicians are addressing this from a systems standpoint, including human resources and equipment resources.
Costa Rica is a progressive country from the standpoint of health care.22 In 1942, the Caja Costarricense de Seguro Social (CCSS) was passed into law. This is essentially a social health care system that covers 87.6% of the population and consists of 23 hospitals with 5,861 beds. Trauma is the fourth leading cause of death in Costa Rica, with both general surgeons and orthopaedic surgeons managing trauma patients. Because it is a social system, trauma care would be provided in one of the larger hospitals, but there are problems in the rural areas, prehospital care, and getting patients to these centers in a timely manner. Furthermore, there are only 154 general surgeons and 85 orthopaedic surgeons in the country. In the 2002 paper, it was admitted that the issue of surgical complications is difficult to analyze because statistics about this problem are underreported. A review of the literature does not catalog the number of surgeons who have taken ATLS training and critical care is somewhat fragmented among medical, anesthesia, and surgical specialties.
South America represents a very heterogeneous mix of trauma system and trauma care. One of the most violent areas in South America is Columbia. Trauma centers are present in Bogata, Medellín, Cali, and Cartagena. Violence is a particular problem secondary to drug trafficking, and the FARC (Revolutionary Armed Forces of Columbia) terrorize the eastern part of Columbia and contribute to the violence in the cities. Because of the differences in altitude and terrain it is extremely difficult to provide ambulance services to some of the more rural and remote parts of Columbia. Even within major cities, there is inconsistent ambulance service. At present, there is no state-wide trauma system.
In a recent study from Brazil, emergency care was assessed for victims of trauma.23 This was a comparative study between two different periods before and after the introduction of modifications in prehospital care. The emergency unit of the University of Saõ Paulo is a hospital committed to trauma care. In addition to changing the prehospital system, they have also introduced ATLS. Despite these measures, the anticipated improvement in outcomes did not match that of the Major Trauma Outcome Study in North America. Nevertheless, it does show that with improvements in education and prehospital health care delivery, outcomes can be improved. Brazil is another country that has violence within the cities and a very large land mass with remote rural areas. There is no country-wide trauma system, and I believe it is fair to say that the universities within the major cities provide the bulk of trauma care. The same is true in Chili, where the economy has improved immensely within the last 30 years. Excellent trauma care is provided in the larger cities, particularly Santiago, but again, because of the geography with mountainous areas and a very long coastline, prehospital care is problematic.
In contrast to North America, the initial trauma care, resuscitation, and critical care in South America is not necessarily provided by general surgeons. Trauma surgeons are not recognized as a separate specialty except in Venezuela. Critical care is more often provided by adult intensivists trained in internal medicine. Many of the Latin American countries have also adopted ATLS and this is particularly true in Argentina. They have also introduced Prehospital Trauma Life Support.
Most of the countries in Latin America have embryonic or developing trauma systems, but the great majority of care is provided by university hospitals. In many instances, this is dependent on local leadership. In addition, the relatively recent organization, Pan American Trauma Society has fostered exchange of information and education between North America and South America.
The countries making up Europe also represent a potpourri of trauma care and trauma systems. Böhler formed the first civilian trauma system in Austria in 1925. The Birmingham Accident Hospital was founded in 1941. It continued to provide regional trauma care until recently. A study done by the Royal College of Surgeons in England showed that preventable death rate approached 33% of the 514 patients with major trauma admitted to hospital accident and emergency departments.24 As a consequence, an experimental trauma center was started in Northwest Midland region.25 The effectiveness of this regional trauma system, in essence, failed. Multiple critiques were offered in the British Medical Journal on the reasons for this failure, including data analysis.26,27,28,29 It was also pointed out in letters to the editor in British Medical Journal that in Glasgow, where 16% of all major trauma is penetrating injuries, the results approach those obtained in the United States. Similar results have been presented from Edinburgh.30 More recently, trauma centers have been started in the London area, but there is no state trauma system in Great Britain.
One of the better trauma systems in Europe is the one that is found in Germany.31,32,33 This system was established in 1975 and was based on the system that had been developed in Austria. This particular system has all four major components of acute care, including prehospital care, resuscitation units, critical care units, and rehabilitation units. The results are remarkable. The mortality has decreased by more than 50% since the establishment of this state-wide trauma system. Incorporation of East Germany into the German Republic has also shown an interesting comparison. The same decrease in mortality is now evident in the East German counties, despite an increase in the number of people injured because of increased use of automobiles. The German system also has a patient registry, and the patients are followed up from the time of injury until resolution of their care through rehabilitation.
Only gold members can continue reading. Log In or Register to continue