landmarks in injury prevention. Some of these events are accomplishments at singular points in time although many formed the basis of activities that continue today. The traffic safety movement of the 1920s and the home safety movement of the 1950s are two such examples3,4,5 (see Table 1).
TABLE 1 A SELECT CHRONOLOGY OF TWENTIETH CENTURY INJURY PREVENTION ACCOMPLISHMENTS | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
of disability and disfigurement.12,13,14,15,16,17,18 As a leading cause of death, injury is fourth behind heart disease, cancer, and stroke (see Fig. 3). As an actual cause of death injury also ranks quite high; this is especially true for certain mechanisms of injury such as motor vehicles and firearms19 (see Table 3).
 Figure 1 Twentieth century mortality reductions from injuries of all causes have been far less than those of other diseases. (Taken from Baker SP, Ginsburg MJ, O’Neill B. The injury fact book, 2nd ed. New York: Oxford Publishing; 1992.) |
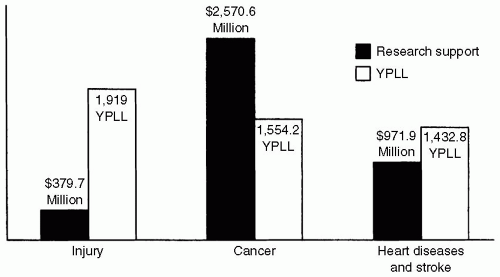 Figure 2 Years of potential life lost (YPLL) versus federal research investment. (Taken from Bonnie RJ, Fulco CE, Liverman CT, eds. Reducing the burden of injury: advancing prevention and treatment. Washington, DC: National Academy Press; 1999:19.) |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


