Abstract
Introduction
Motor imagery can be defined as a dynamic state during which the representation of a movement is internally rehearsed in the absence of voluntary movements. There are two strategies to mentally simulate the movements, either a visual representation of the movements (visual imagery), or kinesthetic feeling of the movement (kinetic imagery). In stroke rehabilitation, studies indicate that motor imagery associated with physical therapy results in cortical reorganization and correlative functional improvements.
Aim
The aim of this study is to provide to the French-speaking community a valid and reliable version of the Movement Imagery Questionnaire – Revised Second Version (MIQ-RS).
Method
We examined the test-retest, inter-rate reliability and the internal consistency of the visual and kinesthetic items of our French version of MIQ-RS in 153 healthy subjects.
Results
Results showed the internal consistency (Cronbach α = 0.90) and test-retest reliability (intraclass correlation coefficient for visual items = 0.68 and for kinesthetic items = 0.78) of the French version of MIQ-RS were satisfactory; the two-factor structure was supported by confirmatory factor analysis.
Conclusion
The French version of MIQ-RS is a valid and reliable instrument in French-speaking population and therefore useful as a measure for motor imagery ability.
Résumé
Introduction
L’imagerie mentale consiste à imaginer mentalement l’exécution d’un mouvement sans que celui-ci soit réellement exécuté. Il existe au moins deux manières de s’imaginer un mouvement, soit en produisant une image visuelle du mouvement soit en simulant les sensations associées au mouvement. L’imagerie mentale est utilisée dans des programmes de rééducation neurologique. L’efficacité de cette rééducation semble dépendante de la façon et de la capacité du sujet à s’imaginer le mouvement. Il semble important de pouvoir tester cette capacité. La version anglophone du Movement Imagery Questionnaire – Revised Second Version (MIQ-RS) permet de tester cette capacité d’imagerie mentale.
Objectif
Traduction et validation de la version française du MIQ-RS.
Méthode
Après la traduction en français du MIQ-RS, nous validons sa cohérence interne, sa reproductibilité entre deux passations et sa validité de construit sur 153 sujets sains.
Résultats
Le coefficient α de Cronbach pour les deux échelles visuelle et kinesthésique est de 0,90, et les coefficients de corrélation intraclasse sont pour l’ensemble des items kinesthésiques à 0,78, et pour l’ensemble des items visuels à 0,68, confirmant la fiabilité du questionnaire. Les analyses factorielles confirment la structure bidimensionnelle du questionnaire.
Conclusion
La version française du MIQ-RS est disponible.
1
English version
1.1
Introduction
Motor imagery (or mental imagery) consists for a subject in imagining the performance of a simple or complex movement that is not accompanied by bodily motion; the movement is internally rehearsed, but does not take place . In the case, there exist at least two ways to imagine a movement :
- •
the subject produces a visual representation of the movement, which he can see himself performing and perceives as a spectator (external imagery); this is also known as visual motor imagery (VMI);
- •
the subject carries out a mental simulation of the movement, which is associated with kinesthetic sensations; he may then be considered as an actor or agent (internal imagery); this is also known as kinesthetic motor imagery (KMI).
The two mental or motor imaging strategies entail activation of the same cerebral regions , which include: the supplementary motor area, the upper and lower parietal lobules, the primary motor cortex, the premotor cortex, the prefrontal areas, the inferior frontal gyrus, the superior temporal gyrus, the primary and secondary sensory cortex, the insula cortex, the cerebellum and the basal ganglia. These areas correspond to the regions directly or indirectly involved in voluntary movement (motor activity). They may even constitute key targets in post-stroke rehabilitation . Gerardin et al. have shown that the simple fact of imagining a movement brings about at the cerebral level an activation of the neural networks relatively similar to actual performance of the same movement, provided that the subject is already familiar with the latter . Moreover and contrarily to VMI, KMI may in turn bring about electromyographic activity in the muscles corresponding to performance of the movement . Over recent years, these neurophysiological findings have facilitated the development of new post-stroke hemiplegia-centered rehabilitative activities including sessions in motor imagery rehabilitation . During sub-acute and chronic phases, the association of motor imagery tasks with traditional rehabilitation of the hemiplegic patient has been shown to assure greater effectiveness in terms of functional recovery than traditional rehabilitation alone .
That said, recruitment of the brain regions associated with motor imagery is correlated with the subject’s ability to imagine the movement and depends on the way it is imagined (VMI or KMI) . The greater a subject’s ability to mentally represent the movement, the more the brain regions involved in the motor system are activated; this fact may explain the inter-individual differences in functional recovery observed during post-stroke rehabilitation mediated by motor imagery activity. It should once again be stressed that the degree of effectiveness achieved through rehabilitation by motor imagery is contingent not only on the subject’s capacity to mentally simulate a given movement, but also on how he does it. In addition, it should be mentioned that post-stroke brain damage may diminish a subject’s ability to engage in motor imagery . Before proposing rehabilitation by means of the latter, one needs to be sure that the subject has maintained the requisite mental capability, and prior to deciding on the most suitable exercises in rehabilitation by motor imagery, it is equally necessary to be aware of the way in which a subject imagines a movement. Is he more adept in VMI or more adroit in KMI? To conclude, therapists may encounter difficulties when assessing motor imagery abilities and when evaluating a patient’s mental representation of an imagined movement.
With these issues in mind, Gregg et al. drew up the Movement Imagery Questionnaire – Revised Second Version (MIQ-RS) on the basis of the 1983 Movement Imagery Questionnaire (MIQ) by Hall and Pongrac and the 1997 Movement Imagery Questionnaire – Revised (MIQ-R) by Hall and Martin . The MIQ-R has already been translated into French and its construct validity (factorial structure and internal consistency) along with its test-retest reliability were duly validated . However, the MIQ-R includes movements such as jumping that demand a considerable degree of agility and motor control, and it is consequently not applicable to subjects presenting with motor deficit or dysfunction. For that reason, construction of a new English language version (MIQ-RS) of the MIQ-R involved subtraction of problematical items such as jumping and addition of items involving simpler gestures. Moreover, the laterality (i.e., left or right direction) of a movement is no longer indicated, and the subject is now allowed to select the limb he wishes to use, thereby enabling a hemiplegic patient to use his non-paretic limb when executing the movement to be performed. Just like the MIQ-R, the MIQ-RS comprises two scales, one of them visual and the other kinesthetic. In its original English language version, the MIQ-RS has been validated as a tool allowing for assessment of the motor imagery abilities maintained by post-stroke hemiplegia patients . The questionnaire is consequently useful with regard to motor imagery in post-stroke rehabilitation.
As of today, there exists no French language version of the MIQ-RS, and the objective of this study is to translate the MIQ-RS into French and to validate the translation in terms of its internal consistency, test-retest reliability and construct validity (factorial structure). Secondary objectives consist in determining whether or not there exist differences in motor imagery abilities, be they visual or kinesthetic, according to gender, age, practice of sport and level of studies.
1.2
Material and methods
1.2.1
Translation procedure
With the agreement of the tool’s designers, the questionnaire was initially translated from English into French by a perfectly bilingual native English speaker residing in France. The translation was then retranslated (retro-translation) from French into English by a perfectly bilingual native French speaker residing in England. The two resulting versions were subsequently compared to each other and to the French version of the MIQ-R drawn up by Lorant. In point of fact, the instruction and evaluation sections, as well as some other items in the original English version of the MIQ-RS, are identical to those of the MIQ-R. As a result, the corresponding parts of the previously validated French translation of the MIQ-R required no modification in our version of the MIQ-RS, which would consequently to some extent incorporate the existing Lorant text. Comparison of the different versions allowed us to carry out the small number of adaptations that were called for. As was suggested by Lorant himself, who differed on this point with Gregg et al. , no numbers was used in the rating scales of the instruction section and the questionnaire itself; an eventual source of bias was thereby precluded.
1.2.2
Population
By far the majority of study participants were employees at the “Les Capucins” rehabilitation center (France). We consequently expected women to be overrepresented and decided that in our sample, it would be necessary to scrupulously test an assumed absence of difference in imagery scores according to gender. Inclusion criteria were: age above 18, volunteer, consenting, with no limitation in mobility or movement disorder. We also took into account level of studies (pre-baccalaureate, baccalaureate, post-baccalaureate), sport practice frequency (lower than or equal to 2 hours, and more than 2 hours), and we divided the population into two age-based categories (under 40 years, 40 years and over). The study was approved by the local ethics committee.
1.2.3
Procedure
At first (Time 1), the questionnaire was completed by 153 healthy volunteers. In order to evaluate the reproducibility (test-retest reliability) of the questionnaire, a week later (Time 2), 113 of the 153 persons filled out exactly the same questionnaire under identical conditions. No intervention liable to modify the subjects’ motor imagery abilities was carried out during this period (situation of stability).
All of the questionnaires were completed in a calm room, with an examiner present, under standardized conditions (video: http://www.youtube.com/watch?v=oddJSEpUMrs ). On arrival, the instructions were read and the participants received an explanation on the contents of the document. The MIQ-RS is a questionnaire consisting in a total of 14 items and two scales (the VMI scale, and the KMI scale). It contains seven items pertaining to kinesthetic motor imagery and seven items pertaining to visual motor imagery. The actions to be performed, which are similar in the two scales, involve the upper limb, the lower limb, the body as a whole, and actions in daily life.
At the outset and for each item, the examiner reads to the participant a description of the movement to be carried out. After that, the participant actually performs the movement and is then asked to either visually or sensorially imagine it. In the questionnaire, the motor tasks are given in a precise order from one through 14 (seven actions, two imaging modalities). The order of the items, which is dictated to the participant, entails performance of the actions involving first visual and then kinesthetic imagery, or vice versa. Lastly, the participant is asked to estimate the ease or difficulty with which he has executed each mental task. Two scales, one of them visual and the other kinesthetic, are placed at his disposal in accordance with what he has been requested to do (VMI or KMI). Each scale comprises seven possible responses (7-point Likert scale):
- •
“very hard to see/feel”;
- •
“hard to see/feel”;
- •
“somewhat hard to see/feel”;
- •
“neutral” (not easy not hard);
- •
“Somewhat easy to see/feel”;
- •
“easy to see/feel”;
- •
“very easy to see/fell” (questionnaire in the Appendix ).
The responses to the items constituting quantitative ordinal variables were subsequently considered to be quantitative variables, as is possible when starting with seven ordinal variables . The per-item score consequently ranged from 1 (“very hard”) to 7 (“very easy”). For each scale (VMI and KMI) and for each participant, a mean score ranging from 1 to 7 was obtained, with a higher score representing better mental imagery ability with regard to the modality having been tested. It takes approximately 20 minutes to administer the test.
1.2.4
Determining the internal consistency of the MIQ-RS (French version)
The internal consistency of the questionnaire was assessed by computing the standardized Cronbach alpha coefficient. Internal consistency is generally deemed acceptable with a coefficient greater than 0.7, good at 0.8 minimum, and excellent when superior to 0.9.
1.2.5
Determining the test-retest reliability of the MIQ-RS (French version)
The repeatability (test-retest) of the scores on each of the scales (visual and kinesthetic) was assessed through comparison of the scores registered for Time 1 and Time 2, the second having occurred 1 week after the first, assuming that the participants’ clinical status had not changed. The comparison was carried out by calculating an intraclass correlation coefficient, the most appropriate tool with regard to quantitative variables according to Shrout and Fleiss (ICC type 3.1, which considers the time effect as a fixed effect) . ICC values are classified as weak (0.1–0.3), moderate (0.3–0.5) and strong (> 0.5) .
1.2.6
Construct validity of the MIQ-RS (French version)
Construct validity of the MIQ-RS questionnaire was tested by confirmatory factor analysis (CFA), which is a method for analysis of the inter-item correlation matrix aimed at confirming the dimensional structure of a questionnaire by verifying correspondence of the correlations with the expected structure.
CFA was performed by specifying the expected dimensional model for the MIQ-RS, which is to say two scales (visual and kinesthetic) composed of their seven respective items. The following parameters have been inferred by means of maximum likelihood estimation (MLE):
- •
correlations between each of the items (observed variable) and the dimension (latent variable) with which it is assumed to be associated (visual or kinesthetic imagery ability);
- •
variability percentage for each of the items as explained by the variability of the dimension with which it is assumed to be associated;
- •
adjustment indexes, which are aimed at verifying the adequacy of the data with regard to the expected model: the χ 2 /df (Q) (a value between 2 and 5 is considered acceptable ), the Root Mean Square Error of Approximation (RMSEA) (a value between 0.05 and 0.10 is recognized a good adjustment ), the Comparative Fit Index (CFI) (a value between 0.90 and 0.96 is recognized as a good adjustment ), the Root Mean square Residual (RMR) and the Standardized RMR (SRMR) (for the last two indexes, values below 0.10 are accepted as satisfactorily adequate ).
1.2.7
Motor imagery scores–the visual and kinesthetic scales
With regard to Time 1 and Time 2, computation of mean scores (average, standard deviation [SD]) was carried out for each scale in the population taken as a whole. The resultant values may vary from 1 to 7, with a score of 7 constituting maximal motor imagery ability.
1.2.8
Statistical analyses
The analyses were carried out for the Cronbach alpha coefficient through SAS 9.2 software with the PROC CORR procedure, for the intraclass correlation coefficients with the INTERACC.SAS macro (copyright 1990 by Robert M. Hamer: http://www.psych.yorku.ca/lab/sas/intracc.htm ) and for confirmatory factor analysis by means of the PROC CALIS procedure. As for the statistical comparisons of VMI and KMI scores according to gender, age, per week sport practice frequency and level of studies, they were carried out with the non-parametric Mann-Whitney test. Comparisons of the VMI and KMI scores between the two testing sessions were carried out with the non-parametric Wilcoxon matched pairs test. P < 0.05 was considered significant. Finally, the statistical tests took place on the registered Graphpad Prism ® software, version 4.00 for Windows (GraphPad Software, San Diego, California, USA).
1.3
Results
1.3.1
Population
One hundred and fifty-three volunteers (118 women) participated in the study at Time 1, mean age 37.9 years (19 to 22 years, SD 12.9 years). One hundred and thirteen persons completed the second questionnaire (Time 2, retest situation), one week after having taken the first test.
1.3.2
Motor imagery scores: visual and kinesthetic scales according to gender, age, and level of studies
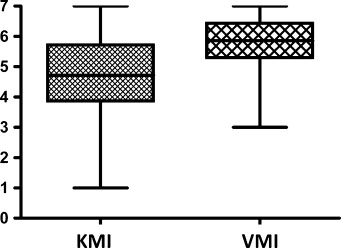
Table 1 and Fig. 1 present the mean scores and SD for VMI and KMI recorded in our population with regard to the first and second tests. The overall score ( n = 153 participants) at Time 1 was higher for visual imagery than for kinesthetic imagery (5.76 [SD: 0.83] and 4.73 [SD: 1.37], respectively), a result clearly indicating that the participants found it easier to imagine movement visually than kinesthetically. As concerns the VMI and KMI scores ( Table 1 ), there is no statistical difference between Time 1 and Time 2 ( P = 0.51 and P = 0.20, respectively) for the 113 subjects having participated in both testing sessions. And once again, the VMI scores (5.73 [SD: 0.81]) were superior to the KMI scores (4.70 [SD: 1.30]).
| Dimensions | n | Mean | Standard deviation |
|---|---|---|---|
| Time 1 (test) | |||
| VMI | 153 | 5.76 | 0.83 |
| KMI | 153 | 4.73 | 1.37 |
| VMI | 113 | 5.73 | 0.81 |
| KMI | 113 | 4.70 | 1.30 |
| Time 2 (retest) | |||
| VMI | 113 | 5.80 | 0.89 |
| KMI | 113 | 4.61 | 1.48 |
There was no statistically significant difference between the mean VMI scores of the women ( n = 118) and the men ( n = 35) participating (5.73 [SD: 0.86] and 5.91 [SD: 0.70], respectively), P = 0.37. Similarly, there was no difference between the two populations with regard to their mean KMI scores (5.15 for the women [SD: 1.20]; 4.62 for the men [SD: 1.41]; P = 0.06).
There was no statistically significant difference between the mean VMI scores of the participants aged under 40 years ( n = 81, mean score = 5.74 [SD: 0.92]) and those of the group of subjects aged 40 years or over ( n = 72, mean score = 5.79 [SD: 0.72], P = 0.76). Nor were there differences between the two sub-groups with regard to their mean KMI scores (4.61 [SD: 1.37] and 4.87 [SD: 1.37], respectively), P = 0.25.
There was no statistically significant difference between the mean VMI scores of the participants practicing less than 2 hours of sports a week ( n = 85, mean score 5.76 [SD: 0.80]), and those of the control group practicing at least 2 hours of sports a week ( n = 68, mean score 5.77 [SD: 0.86]) P = 0.84. Nor were there differences between the two populations as concerns their KMI scores (4.59 [SD: 1.40] and 4.90 [SD: 1.33]), P = 0.18.
There was no statistically significant difference between the mean VMK scores of the persons with a post-baccalaureate level of studies ( n = 101, mean score 4.87 [SD: 1.34]) and those of the group with a baccalaureate or pre-baccalaureate level of studies ( n = 521, mean score 4.42 [SD: 1.36]), P = 0.051. By contrast, there existed a statistically significant difference between the mean VMI scores of the two populations, 5.50 [SD: 0.77] and 5.90 [SD: 0.83], respectively, P = 0.001.
Table 2 presents the mean scores, the SD and the minimum and maximum levels reached by the 153 subjects, taken a whole, during Time 1.
| Items | Scale | Mean score | Standard deviation | Minimum score | Maximum score |
|---|---|---|---|---|---|
| 1 | KMI | 4.68627 | 1.86897 | 1.00000 | 7.00000 |
| 2 | VMI | 5.72549 | 1.31407 | 1.00000 | 7.00000 |
| 3 | KMI | 4.85621 | 1.57036 | 1.00000 | 7.00000 |
| 4 | VMI | 5.61438 | 1.24670 | 2.00000 | 7.00000 |
| 5 | VMI | 5.70588 | 1.12906 | 2.00000 | 7.00000 |
| 6 | KMI | 4.39869 | 1.72192 | 1.00000 | 7.00000 |
| 7 | KMI | 4.40523 | 1.59538 | 1.00000 | 7.00000 |
| 8 | VMI | 5.96078 | 1.19143 | 1.00000 | 7.00000 |
| 9 | KMI | 4.97386 | 1.58922 | 1.00000 | 7.00000 |
| 10 | VMI | 5.88889 | 1.18962 | 2.00000 | 7.00000 |
| 11 | KMI | 4.90850 | 1.63578 | 1.00000 | 7.00000 |
| 12 | KMI | 5.05882 | 1.44748 | 1.00000 | 7.00000 |
| 13 | VMI | 5.79739 | 1.13183 | 2.00000 | 7.00000 |
| 14 | VMI | 5.67320 | 1.17445 | 2.00000 | 7.00000 |
1.3.3
Determining the internal consistency of the MIQ-RS (French version)
The standardized Cronbach alpha coefficient with regard to the questionnaire taken as a whole was 0.90, which means that the internal consistency of the French version of the MIQ-RS may be considered excellent.
1.3.4
Determining the test-retest reliability of the MIQ-RS (French version)
The computed intraclass correlation coefficient (ICC type 3.1) was 0.78 for the different kinesthetic items and 0.68 for the different visual items, and these figure confirm a high degree of repeatability over time.
1.3.5
Construct validity of the MIQ-RS (French version)
The correlations between items and dimensions were strong, ranging from 0.74 to 0.85 according to the items for the kinesthetic dimension, and from 0.65 to 0.79 according to the items for the visual dimension. All of these correlations were exceedingly significant, as is illustrated in Table 3 by the t test values ranging from 8.57 to 12.88, figures corresponding to P -values ranging from 10–19 to 10–31 ( Table 3 ).
| Scale | Items | Dimension 1: kinesthetic imagery ability | Dimension 2: visual imagery ability | ||
|---|---|---|---|---|---|
| Correlation ( t ) a | R 2 b | Correlation ( t ) a | R 2 b | ||
| Kinesthetic | 1 | 0.75 (10.68) | 0.57 | ||
| 3 | 0.80 (11.64) | 0.64 | |||
| 6 | 0.81 (11.82) | 0.65 | |||
| 7 | 0.83 (12.43) | 0.70 | |||
| 9 | 0.85 (12.88) | 0.73 | |||
| 11 | 0.74 (10.42) | 0.55 | |||
| 12 | 0.80 (11.60) | 0.64 | |||
| Visual | 2 | 0.67 (8.87) | 0.44 | ||
| 4 | 0.77 (10.83) | 0.59 | |||
| 5 | 0.66 (8.88) | 0.44 | |||
| 8 | 0.79 (11.14) | 0.62 | |||
| 10 | 0.76 (10.66) | 0.58 | |||
| 13 | 0.65 (8.57) | 0.42 | |||
| 14 | 0.76 (10.66) | 0.58 | |||
a Correlation between item and dimension (degree of significance of that correlation as illustrated by t test value).
b R 2 : the item’s percentage of variability as explained by the dimension’s variability.
The variability percentages for the items as explained by the variability of the corresponding dimension ranged from 55 to 73% according to the items with regard to the kinesthetic dimension, and from 42 to 62% according to the items with regard to the visual dimension ( Table 3 ).
Finally, the values of the adjustment indexes were Q (χ 2 /df, 169.44/76) = 2.23; RMSEA = 0.09; CFI = 0.93; RMR = 0.06; SMR = 0.06, results meeting the adequacy criteria described in the Methods section of this paper.
Taken as a whole, these results confirm the expected two-dimensional structure of the MIQ-RS questionnaire (French version).
1.4
Discussion
This study effectively validates the metrological qualities of our French translation of the MIQ-RS, which can henceforth be proposed to a French-speaking public. Indeed, the reliability of this version, which was assessed in terms of internal consistency and repeatability, has been deemed excellent. The questionnaire’s Cronbach alpha coefficient was equal to 0.9 , and the ICC values were greater than 0.5 for each of the two scales . The two-dimensional (visual and kinesthetic) structure of the MIQ-RS was unambiguously confirmed by CFA. Moreover, there was no “learning effect” altering the results of the second series of test sessions, which took place one week after the first; the mean scores at Time 1 and at Time 2 were so similar as to underscore the satisfactory reproducibility of the questionnaire over a specified length of time.
As for the overrepresentation of women in our population, which was largely due to our means of recruitment (over half the participants were employees in our rehabilitation center), it did not constitute a meaningful bias in the validation methodology applied to the French version of the MIQ-RS. It has already been demonstrated that there does not exist a significant difference between men and women as regards motor imagery ability , and this finding was corroborated in our sample. It would nonetheless appear that women’s KMI abilities tend to be greater than men’s; unfortunately, the overrepresentation of women in our study does not allow us to offer further interpretation of this tendency, which would require targeted analysis in a dedicated study.
Nor does there exist a difference in visual or kinesthetic imagery ability according to a participant’s degree of sports practice. In this respect, however, it is interesting to note that Lorant has shown that regular sports practice and experience in practicing seem to constitute elements favoring enhanced kinesthetic imagery ability, whereas in our work, no connection was found between the respective levels of sports practice and mental or motor imagery. That said, our sample was not built in such a way as to provide an answer directly addressing the question of a possible association between the two. In our study, the boundary line of two weekly hours of sports practice was established arbitrarily, and it would be worthwhile, in the future, to get to know the effect of the number of hours of regular sports practice on a subject’s motor imagery capabilities; it would be similarly interesting to get to know the effect on these capacities of the type of discipline favored by the subject (martial arts, motor sports, team sports…).
The movement imagery questionnaire is consequently a tool assessing visual and kinesthetic imagery ability. Having been validated, this French language version of the MIQ-RS may potentially be used in the field of neurological rehabilitation in patients presenting with motor disorders such as post-stroke hemiplegia so as to determine their motor imagery ability. Indeed, the subtraction of some items, such as jumping, and the addition of other items (a simple action, such as grasping and/or gripping) should enable the MIQ-RS to be employed by patients with reduced motor skills. And since the questionnaire contains no indication of the side of the body to be used when carrying out an action to be imagined, it could be particularly helpful in hemiplegic subjects, who might be called upon to perform a task such as “take a glass” with the non-deficitary upper limb, as is the case in the study by Butler et al. validating the MIQ-RS in stroke populations . Given these results, which were achieved in an English-speaking environment , our French language validation in a population devoid of motor difficulties supports the hypothesis that the tool is applicable in French-speaking populations with motor deficiency or dysfunction. Complementary studies with French-speaking aphasic patients would be particularly relevant.
In addition to the metrological aspects of our work, it is apparent that the tested participants registered higher VMI than KMI scores, thereby confirming that it is more difficult for untrained subjects to perform KMI as opposed to VMI tasks. In their validation study of the original English language MIQ-RS, Gregg et al. demonstrated that with regard to their population, VMI is easier to achieve than KMI, and this fact should no doubt be taken into account when drawing up a rehabilitative motor imagery task. Indeed, it appears easier to propose motor imagery exercises calling upon visual as opposed to kinesthetic imagery. From a neuro-functional standpoint, however, as demonstrated by Solodkin et al. , even though VMI and VKI present a common pattern of cerebral activation, especially at the level of the supplementary motor area, they also differ from each other. While VMI more strongly activates the occipital areas, KMI more strongly activates the primary motor and sensory areas. While KMI appears to preferentially call upon sensory-motor feedback (internal imagery), VMI appears to preferentially call upon a visuo-motor pattern or connection (external imagery). Moreover, only KMI appears to bring about electromyographic activation at the level of the muscles solicited by the movement imagined . It would consequently seem well-advised to propose a form of motor imagery rehabilitation involving exercises in VMI as well as KMI, and to make sure that they take into full account the motor imagery performances tested by the MIQ-RS. It should also be pointed out that the absence of differences between men and women with regard to motor imagery ability should render it feasible to envision that rehabilitative motor imagery tasks be the same, regardless of gender. As for the absence of association in our study results and in those of Butler et al. between age and mental imagery ability, it may also be feasible to envision mental imagery testing in adult subjects, regardless of age. Complementary findings on subjects over 75 years of age, who were not represented in our sample, would likewise be helpful.
If the questionnaire presents undeniable interest with regard to the elaboration of rehabilitation programs employing motor imagery, one reason is that it may help to highlight the motor imagery capacities proper to each patient. For example, a patient presenting strong ability in VMI and weak ability in KMI may be given exercises favoring VMI and simpler movements in KMI. That said, there does not exist a threshold value for VMI and KMI allowing one to say that a subject’s motor imagery ability is weak or strong. On an overall basis, the values pertaining to the 14 items of the MIQ-RS approximate 5 (as in the MIQ-RS concept design study ), with possible scores ranging from 1 to 7. It may be surmised that for a given participant, a VMI or KMI score lower than the values ranging from 4 to 5 shows low imagery ability, while a higher score would translate high imagery ability. If the results are homogeneous with regard to the different items, it may be supposed that the degree of difficulty of the latter is correspondingly similar. In our work, we also noted that a subject’s level of studies appears to have some incidence on his or her motor imagery ability; to our knowledge, this point was not taken up in the preliminary studies, and it would seem important to understand by dint of which factor level of studies may alter motor imagery ability. Is it simply a matter of competence in comprehending the questionnaire, or is it associated with an experience of memorization and internalization of movements that would be more substantial in post-baccalaureate subjects? Targeted studies will surely help to elucidate connections between motor imagery ability and level of cognition.
Lastly, motor imagery may be employed as part of a cognitive strategy likely to improve motor skill acquisition and enhance athletes’ motor performances . To date, it has not been demonstrated that the most competent subjects in terms of motor imagery are likewise the most competent subjects in terms of actual motor tasks.
The French version of the MIQ-RS places at the disposal of French-speaking researchers a tool facilitating study of mental or motor imagery ability in a large-scale population. VMI and KMI tests may be taken in 20 to 30 minutes, and this should allow a large use of the scale.
1.5
Conclusion
This study places the validated French version of the MIQ-RS at the disposal of French-speaking rehabilitation therapists; more broadly speaking, this tool assessing subjects’ motor imagery ability is addressed to the scientific community. It may be consulted in the Appendix of this paper.
Disclosure of interest
The authors declare that they have no conflicts of interest concerning this article.
Acknowledgements
The authors wish to thank M. Gregg, A.J. Butler and C. Hall for having allowed us to translate and validate their tool (MIQ-RS). We also wish to thank M. Fisbach and M. Koffi for the translation and the retro-translation, respectively. Finally, we wish to thank all of the participants.
Related posts:
 Speaking French: Will it be a shared opportunity for scientific communication in PMR?
Traumatic brain injury rehabilitation, the programs applied in French UEROS units, and the specificity of the Limoges experience
Goal Attainment Scaling in rehabilitation: A literature-based update
Non-surgical management of posterior positional plagiocephaly: Orthotics versus repositioning
The effects of respiratory muscle training on improvement of the internal and external thoraco-pulmonary respiratory mechanism in COPD patients
Neuromuscular diseases
Speaking French: Will it be a shared opportunity for scientific communication in PMR?
Traumatic brain injury rehabilitation, the programs applied in French UEROS units, and the specificity of the Limoges experience
Goal Attainment Scaling in rehabilitation: A literature-based update
Non-surgical management of posterior positional plagiocephaly: Orthotics versus repositioning
The effects of respiratory muscle training on improvement of the internal and external thoraco-pulmonary respiratory mechanism in COPD patients
Neuromuscular diseases
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


