Thoracic Orthopaedic Tests
Palpation
Anterior Aspect
Descriptive Anatomy
The sternum, which lies at the anterior part of the chest wall, consists of three parts: the manubrium, body, and xiphoid process. It articulates with the costal cartilages on both sides. The manubrium also articulates with the facets of the clavicle on both sides (Fig. 9-1).
Procedure
Palpate the entire length of the sternum for tenderness or abnormality (Fig. 9-2). Also palpate the costal margins and sternal clavicular articulations for tenderness, pain, and displacement (Fig. 9-3). Pain and tenderness following trauma may indicate a fractured sternum or bruised costal cartilages. Tender sternocostal or sternoclavicular articulations may indicate a sprain or subluxation of the suspect articulation.
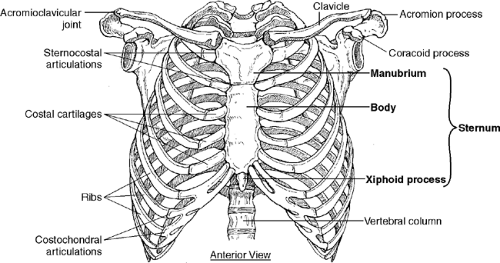 Figure 9-1 |
 Figure 9-2 |
 Figure 9-3 |
Descriptive Anatomy
The ribs at the anterior aspect of the rib cage are attached to the sternum by costal cartilages, forming the costochondral articulation. They also articulate with the sternum, forming the sternocostal articulations (Fig. 9-4).
Procedure
Palpate each costal cartilage with its associated rib from the lateral aspect of the sternum laterally to the axilla. Then palpate into each intercostal space (Fig. 9-5). Tender costal cartilages may indicate costochondritis (Tietze’s syndrome). Tender intercostal spaces may indicate an irritated intercostal nerve or a herpes zoster viral infection. Associated with this infection may be red vesicular eruptions along the course of the intercostal nerve in the intercostal space. Tenderness that follows trauma may indicate a fractured rib.
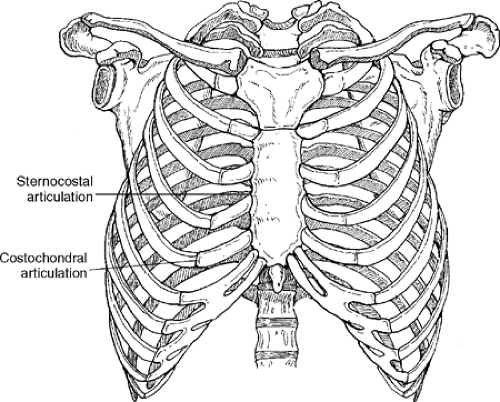 Figure 9-4 |
 Figure 9-5 |
Posterior Aspect
Descriptive Anatomy
At the posterior aspect of the thorax, the scapula articulates with the posterior aspect of the ribs. It also forms part of the glenoid fossa, which articulates with the head of the humerus. On the anterior aspect, the acromion articulates with the clavicle, forming the acromioclavicular joint. The scapula normally extends from T2 to T7. It has three borders: medial, lateral, and superior (Fig. 9-6).
Procedure
Starting with the medial border, palpate all three borders, noting any tenderness (Figs. 9-7 to 9-9). Next, palpate the spine of the scapula, noting any tenderness or abnormality (Fig. 9-10). Finally, palpate the posterior surfaces above the spine of the scapula for the supraspinatus muscle (Fig. 9-11) and below the spine for the infraspinatus muscle (Fig. 9-12). Note any tenderness, atrophy, or spasm.
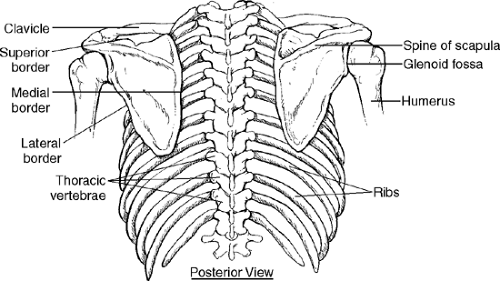 Figure 9-6 |
 Figure 9-7 |
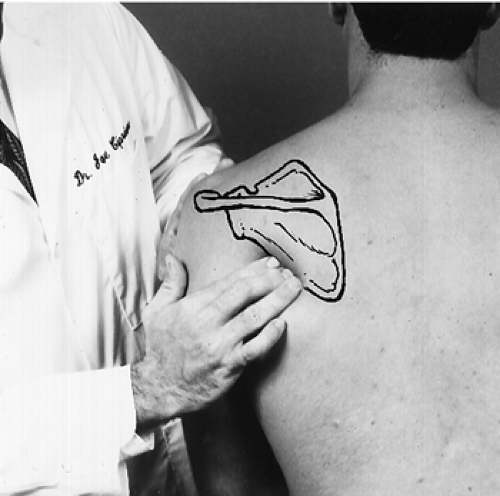 Figure 9-8 |
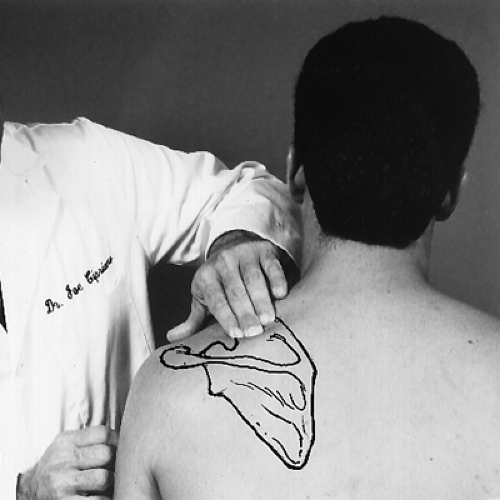 Figure 9-9 |
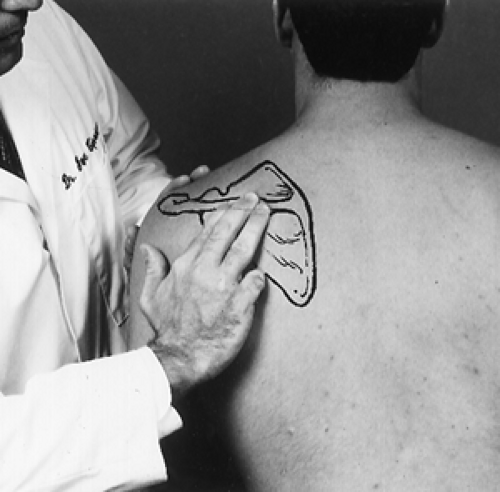 Figure 9-10 |
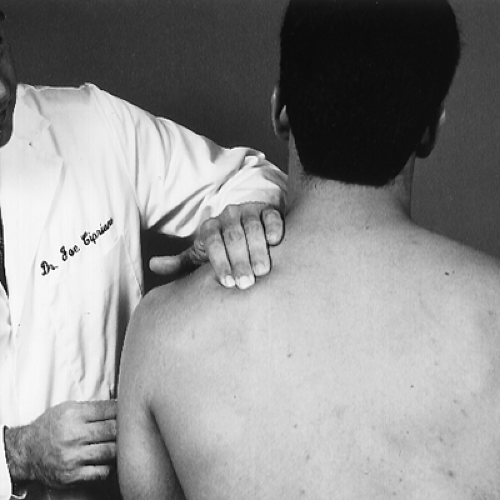 Figure 9-11 |
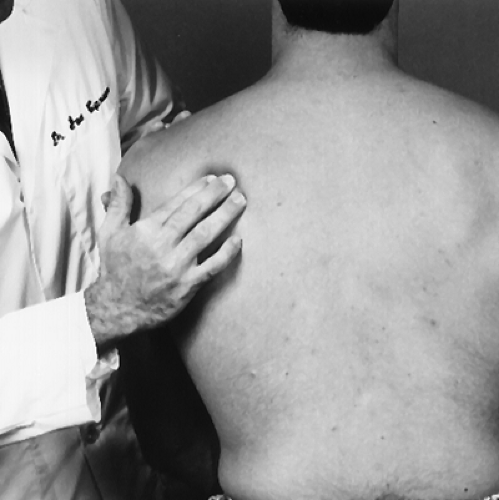 Figure 9-12 |
Descriptive Anatomy
The thoracic spinal muscles are arranged in three layers: superficial, intermediate, and deep. The superficial layers include the trapezius, latissimus dorsi, levator scapulae, and rhomboid muscles (Fig. 9-13). The intermediate layer contains the serratus posterior, serratus superior, and serratus inferior muscles (Fig. 9-14). The deep muscles of the back are ones that maintain posture and move the spinal column. These muscles, the erector spinae group, consist of the spinalis, longissimus, and iliocostalis (Fig. 9-14).
Procedure
Palpate the superficial layer by moving your fingers in a transverse fashion over the belly of the muscle, noting any abnormal tone or tenderness (Fig. 9-15). Palpate the deep layer with the fingertips directly adjacent to the spinous processes (Fig. 9-16), noting any abnormal tone or tenderness. Any abnormal tone or tenderness may indicate an inflammatory process in the muscle, such as muscle strain, myofascitis, or fibromyalgia.
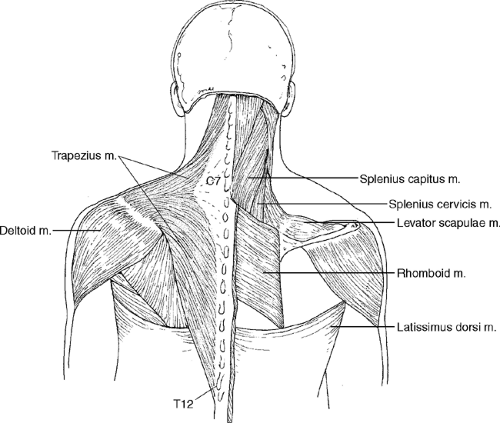 Figure 9-13 |
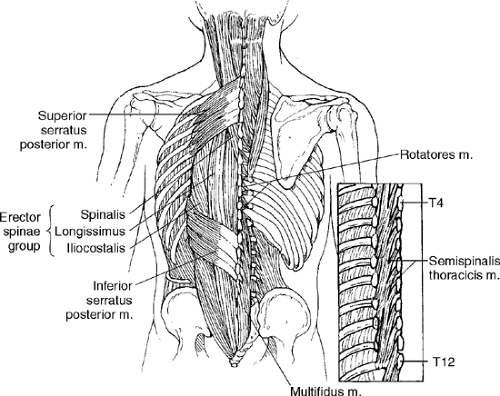 Figure 9-14 |
 Figure 9-15 |
 Figure 9-16 |
Descriptive Anatomy
The T1 to T12 vertebrae have relatively prominent spinous processes that are easily palpable (Fig. 9-17). The tip of each spinous process is below the transverse process of the same vertebra.
Procedure
With the patient seated and thorax slightly flexed, palpate each spinous process with your index and or middle finger, noting any pain, tenderness, and abnormal alignment. Each process should be palpated individually (Fig. 9-18). Next, push each spinous process laterally, noting any rotational mobility (Fig. 9-19). Tenderness upon static spinous palpation may indicate subluxation of a thoracic vertebra. Tenderness secondary to flexion or extension injury may indicate supraspinous ligament sprain, especially in the upper thoracic vertebra. Abnormal gross alignment may indicate scoliosis.
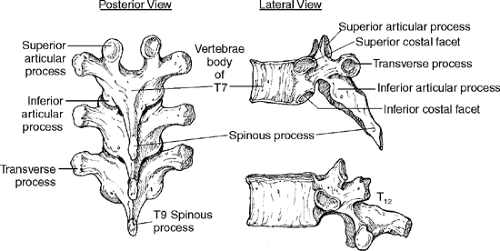 Figure 9-17 |
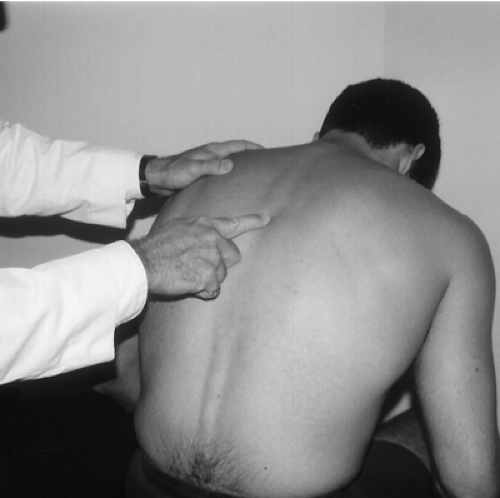 Figure 9-18 |
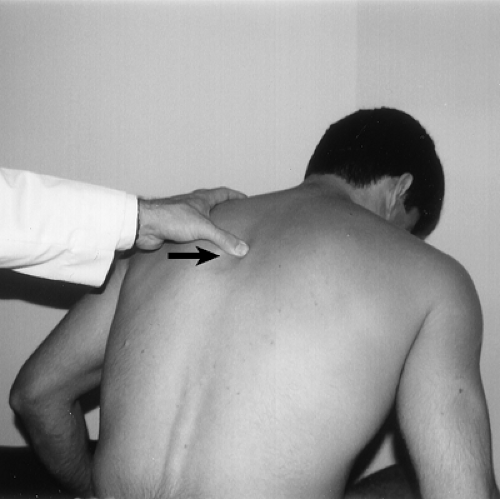 Figure 9-19 |
Descriptive Anatomy
The ribs at the posterior aspect of the rib cage are attached to the vertebral body and transverse process by a capsule and a series of ligaments and muscles (Fig. 9-20). The ribs can bend slightly under stress without breaking. Between the ribs in the intercostal spaces are three layers of intercostal muscles and an intercostal nerve. This nerve can become infected with the herpes zoster virus, which invades the spinal ganglia and produces sharp burning pain in the area supplied by the affected intercostal nerve.
Procedure
Palpate each individual rib from the lateral aspect of the spinal column laterally to the axilla. Then palpate each intercostal space (Fig. 9-21). Tenderness or pain following trauma may indicate a fractured rib. Tender intercostal spaces may indicate an irritated intercostal nerve or a herpes zoster viral infection. Associated with this infection may be red vesicular eruptions along the course of the intercostal nerve in the intercostal space.
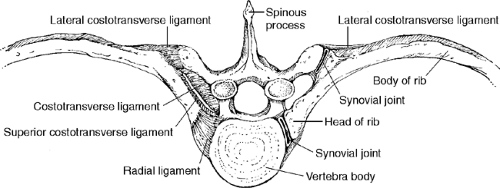 Figure 9-20 |
 Figure 9-21 |
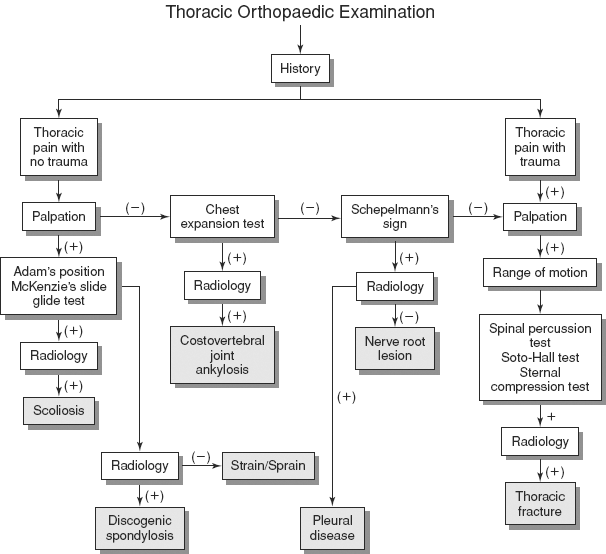
Thoracic Range of Motion
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


