The Uncemented Socket
James A. Keeney
John C. Clohisy
BACKGROUND
Cementless fixation has become the primary method of acetabular component reconstruction in North America as several reports have suggested unacceptably high failure rates of cemented acetabular fixation (1,2,3). Contemporary acetabular implant designs incorporating surfaces favorable to biologic fixation have demonstrated excellent implant survivorship, provided that adequate initial implant stability has been obtained with interference fit or with the addition of supplemental screws or spikes (4,5,6,7,8,9,10,11). While fixation failures of contemporary cementless acetabular components have been infrequently reported, conventional ultrahigh molecular weight polyethylene (UHMWPE) wear rates have been the predominant source of failure among cementless component designs implanted during the 20th century (3,11,12,13,14,15). The introduction of highly cross-linked polyethylene into contemporary cementless acetabular components has demonstrated limited wear, even among highly active individuals, and leads to cautious optimism that this combination will result in longer acetabular component survivorship (16).
INDICATIONS
Cementless fixation can be utilized for all primary and revision total hip arthroplasty procedures. Diagnoses commonly addressed with primary cementless implants include the following:
Osteoarthritis secondary to acetabular dysplasia or femoroacetabular impingement
Protrusio acetabuli
Osteonecrosis
Inflammatory arthritis
Femoral neck fracture
PREOPERATIVE PREPARATION—GENERAL CONSIDERATIONS
Attentive preoperative planning is an essential component of successful acetabular reconstruction, regardless of the fixation method utilized. The desired depth of acetabular reaming relative to the medial wall should be determined for implant fit and superolateral coverage. The placement and sizing of acetabular components may vary for hips depending on the primary diagnosis. The presence of osteophytes in the floor of the acetabulum may result in a lateralized hip center among patients with osteoarthritis and may require medialization beyond the floor of the cotyloid fossa (Fig. 13-1). Lateralization of the hip center may also occur with hip dysplasia, and the amount of medialization will vary depending on the thickness of the pelvis and the amount of preparation necessary to obtain adequate lateral implant coverage and stability (Fig. 13-2). In some cases of severe acetabular protrusio, it may be necessary to lateralize the hip center into a more normalized position (Fig. 13-3).
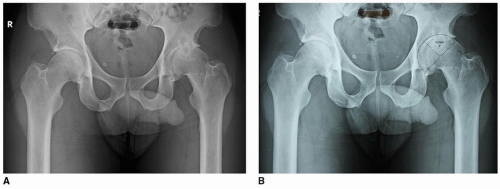 FIGURE 13-1 A: Hip osteoarthritis with lateralized hip center. B: Templated. |
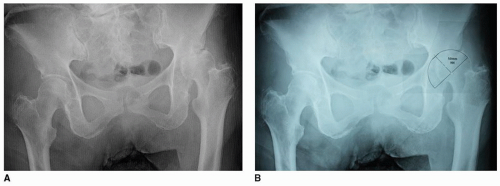 FIGURE 13-2 A: Hip dysplasia with lateralized hip center. B: Templated. |
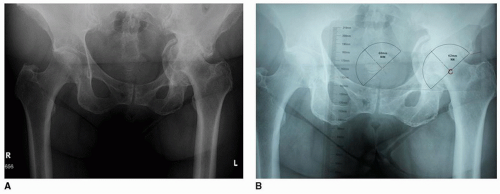 FIGURE 13-3 A: Acetabular protrusio. B: Templated. |
Medialization of the acetabular component is important to reduce biomechanical forces on the hip and to provide adequate contact between the implant and the acetabular bone for successful osseointegration. Traditional techniques used in cemented total hip arthroplasty have advocated for acetabular component placement within 1 to 2 mm of the medial acetabular wall (17). In cases where the acetabulum has been medialized substantially relative to patient’s native hip center, this may result in a decrease in tension of the gluteus medius and minimus muscles and potentially contribute to prosthetic joint instability. Femoral offset or length may need to be increased in order to optimize hip stability in these cases. Charnley’s surgical approach, utilizing a trochanteric osteotomy, facilitated advancement of the trochanter in order to improve soft tissue tension with the reconstruction. However, concerns of trochanteric nonunion have limited the use of this exposure in contemporary arthroplasty. Acceptance of a slightly more lateral acetabular component position relative to the medial wall may be preferred for cases where medialization will substantially reduce femoral offset. It may also be an acceptable consideration for younger THA patients in whom the preservation of medial and posterior bone will facilitate safe removal of well-fixed components if indicated in the future (e.g., malposition, instability, infection).
Knowledge of acetabular implant design is also important. Enlargement of the peripheral rim of the acetabular component may vary with implant manufacturer and component design. Selection of the appropriate final reamer should allow for a 1- to 2-mm press fit of the acetabular component against the prepared acetabular bone according to implant design specifications. With some of the newer porous metals, line-to-line reaming has been advocated. Surface characteristics and implant stiffness will dictate the reaming technique.
TECHNIQUE
Surgical Exposure
Several anatomical approaches to the hip are available and may be selected based on patient preferences and surgeon experience. Details of the surgical approaches have been described in Chapters 1, 2, and 3
 The Direct Lateral Approach for Total Hip Arthroplasty
The Direct Lateral Approach for Total Hip Arthroplasty
 Arthroscopy for Structural Hip Problems
Arthroscopy for Structural Hip Problems
 Double-Tapered Primary Stems
Double-Tapered Primary Stems
 Uncemented Acetabular Revision with Metal Augments or Cup-Cage Combinations
Uncemented Acetabular Revision with Metal Augments or Cup-Cage Combinations
 Tapered Fluted Titanium Stems in Revision Total Hip Arthroplasty
Tapered Fluted Titanium Stems in Revision Total Hip Arthroplasty
 Techniques to Manage Infection around Total Hip Arthroplasty and Antibiotic-Loaded Spacers for Infection
Techniques to Manage Infection around Total Hip Arthroplasty and Antibiotic-Loaded Spacers for Infection




Related posts:
The Direct Lateral Approach for Total Hip Arthroplasty
Arthroscopy for Structural Hip Problems
Double-Tapered Primary Stems
Uncemented Acetabular Revision with Metal Augments or Cup-Cage Combinations
Tapered Fluted Titanium Stems in Revision Total Hip Arthroplasty
Techniques to Manage Infection around Total Hip Arthroplasty and Antibiotic-Loaded Spacers for Infection
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
