and Gautam M. Shetty2
(1)
Consultant Joint Replacement Surgeon Department of Orthopaedic Surgery, Breach Candy Hospital, Mumbai, Maharashtra, India
(2)
Consultant Arthritis Care and Joint Replacement Surgery, Asian Orthopedic Institute Asian Heart Institute and Research Center, Mumbai, Maharashtra, India
Abstract
A stiff knee is defined as having a range of motion of less than 50° [1]. The most common cause of stiffness in an arthritic knee is osteoarthritis and rheumatoid arthritis [2–6]. Less common causes include previous trauma, surgery, infection, ankylosing spondylitis, psoriatic arthritis and haemophilic arthropathy [2–6].
Introduction
A stiff knee is defined as having a range of motion of less than 50° [1]. The most common cause of stiffness in an arthritic knee is osteoarthritis and rheumatoid arthritis [2–6]. Less common causes include previous trauma, surgery, infection, ankylosing spondylitis, psoriatic arthritis and haemophilic arthropathy [2–6].
Approaching a stiff knee for TKA is not only difficult but is fraught with risks. This is one situation where a tibial tubercle osteotomy or a quadriceps snip may be required to achieve adequate exposure [7]. Furthermore, stiffness of soft tissues and the associated osteoporosis put these knees at high risk for inadvertent intraoperative fractures or soft-tissue avulsions [3, 4]. Apart from the difficulty in approaching the knee during TKA, stiff knees usually have significant changes in the intra- and periarticular soft tissues which make soft-tissue release and balancing more challenging. In addition to excessive fibrous tissue within the joint, important soft-tissue structures such as the quadriceps, cruciates and collateral ligaments and the joint capsule may be scarred and contracted. Hence, the integrity and competence of these important soft-tissue stabilisers of the knee is unclear and often difficult to assess.
Although technically demanding, TKA in stiff knees has been reported to significantly improve knee range of motion and function [2–4, 8–10]. However, meticulous surgical technique and aggressive postoperative rehabilitation is the key to improve overall function after TKA in stiff knees. In this chapter, the authors describe their approach to treating stiff arthritic knees with TKA.
Pathoanatomy
Stiffness in arthritic knees undergoing TKA is mainly a consequence of severe soft-tissue adhesions within and around the joint. This is more pronounced in stiffness caused due to previous trauma, surgery or infection. In cases with osteoarthritis and rheumatoid arthritis, large multiple osteophytes and adaptive bone changes may cause mechanical blocks to knee movement, further aggravating the stiffness.
Adhesions tethering the quadriceps muscle in the suprapatellar area along with severe patellofemoral arthritis (Fig. 9.1) can be a major cause of limited flexion. Contraction of the posterior capsule along with large osteophytes posteriorly can block extension (Fig. 9.1). Fibrous tissue in the lateral and medial gutters, posterior compartment and the suprapatellar pouch and around soft-tissue structures such as cruciates, collaterals, quadriceps and flexor tendons can severely restrict joint range of motion.

Fig. 9.1
Preoperative lateral knee radiograph showing severe patellofemoral arthritis which will restrict knee flexion and large posterior femoral osteophyte (arrow) which will restrict knee extension
A thorough examination of the knee under anaesthesia will give clues about the actual type of deformity in the coronal plane (varus or valgus) and the amount of medio-lateral laxity present (Fig. 9.2). It will also enable the surgeon to assess the actual knee ROM which might be severely restricted if examined without anaesthesia due to pain and reactive (muscular) spasm. A proper assessment of medio-lateral soft-tissue imbalance can only be possible once the knee has been exposed and the range of motion improves with excision of fibrous tissue, cruciates and osteophytes. The key is to proceed with caution and patience and release all the fibrous tissue and tethered soft-tissue structures and excise all the osteophytes. In most cases, this will correct the flexion and extension deformity to a large extent, and the surgeon will achieve adequate exposure of the joint to proceed with the actual TKA procedure.
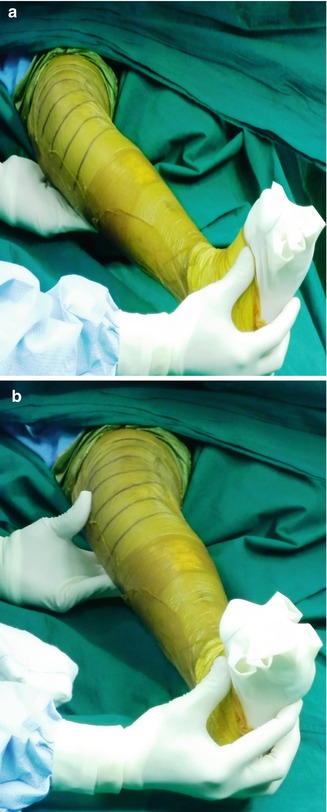

Fig. 9.2
Examination of the knee under anaesthesia to determine the type of coronal deformity and severity of knee stiffness. (a) Medial laxity with a valgus stress at the knee joint. (b) Lateral laxity with a varus stress at the knee joint. (c) Maximum knee flexion. (d) Maximum knee extension
Patients with a stiff knee need to be counselled in detail about their expectations and the likely outcome. They must be told that they may not achieve as much flexion as a person without long-standing stiffness and must not compare their progress with other patients undergoing routine TKA! Also it must be emphasised to them that they will need to undergo extensive physiotherapy to maintain and augment the range obtained at surgery.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


