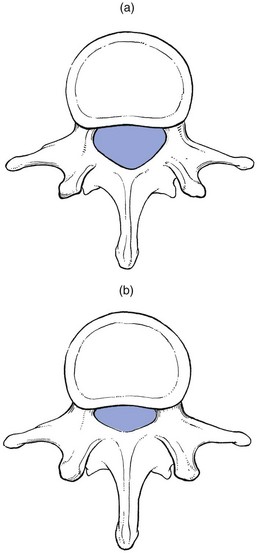
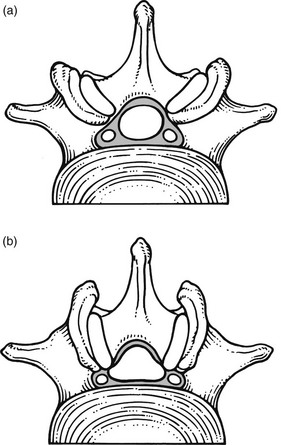
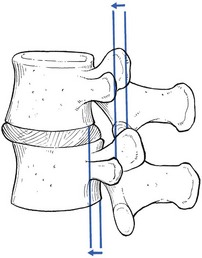
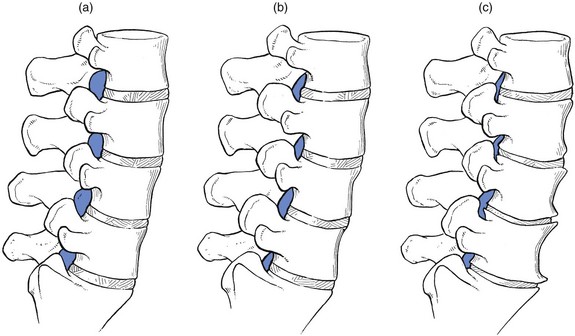
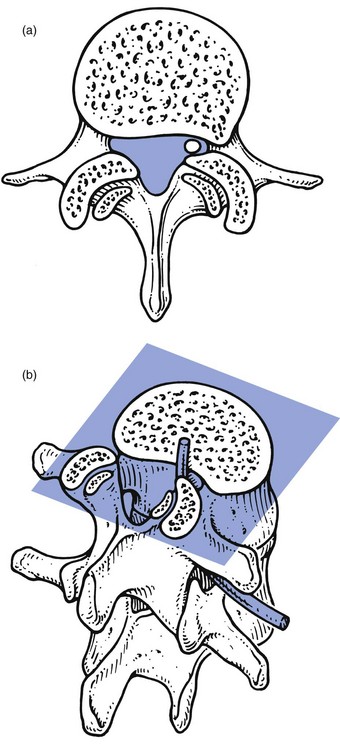
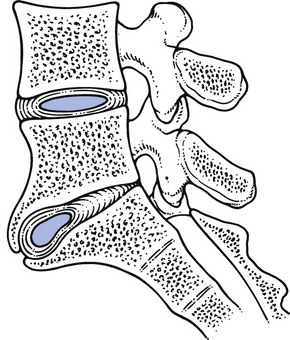
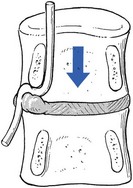
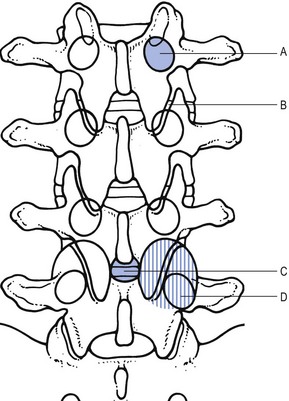
35 Compression of lumbosacral nerve roots by osteoarthritic changes in the lumbar spine has been recognized since 1900, when Sachs and Fraenkel1 published the case of a Russian tailor suffering from intermittent paresis of the legs, which improved markedly after removal of the thickened, enlarged laminae of T11 and T12. Further reports on the consequences of lumbar osteoarthrosis on the function of nerve roots followed.2,3 Patients suffering from root pain in whom the only operative finding was a marked thickening of the ligamentum flavum were also recognized,4–6 and excision of the ligaments produced considerable relief of symptoms. A hypertrophied ligamentum flavum as one possible cause for backache and sciatica was suggested both in 19377 and 1945.8 By 1945, congenital narrowing of the bony canal was recognized as responsible for pressure on the cauda equina8 and, in the same decade, for nerve entrapment at the foraminal level.9 Overhanging facets were also postulated to be a cause of nerve root irritation.10 The definitive account of developmental narrowing of the lumbar vertebral canal causing radicular symptoms was given in the 1950s.11,12 In recent decades there have been many publications on the different types of ‘spinal stenosis’, and a consensus has been reached on the classification and pathophysiology of the different types of this lesion.13–17 • Idiopathic developmental stenosis of the bony lumbar vertebral canal is a genetic disturbance that reveals its pathological effect only when growth is complete.18 The narrowing is uniform over almost the whole length of the lumbar bony canal. A mid-sagittal diameter of 10 mm or less is an absolute stenosis – the narrowing is capable of producing signs of compression of the neural content in the absence of other compressive agents. A relative stenosis has a diameter of 10–12 mm and can only lead to compression if other vertebral deformities, such as spondylitis or posterior vertebral osteophytes, compound the narrowing. • Acquired spinal stenosis is the consequence of arthrotic changes, disc herniations, postsurgical or post-traumatic lesions, or bone diseases, including tumours. • Degenerative stenosis, as its name implies, follows degenerative changes in the spine. Such narrowing is segmental and most marked between disc and posterior articular processes. Between the stenotic regions, the diameters of the vertebral canal are usually normal. • Iatrogenic stenosis is the name sometimes given to stenosis resulting from surgical procedures that have caused considerable peridural fibrosis.19 • Lateral recess stenosis indicates a narrowing of the vertebral canal in its lateral portion (the lateral recess). The condition should be differentiated from narrowing of the entire vertebral canal (lumbar stenosis) caused by either a short sagittal or transverse diameter, or by a combination of both. The two cause different clinical syndromes: lumbar stenosis is related to both legs, often involving several dermatomes; the main symptom is neurogenic intermittent claudication. Lateral recess stenosis is characterized by root pain, confined to one dermatome only. The frequency of lumbar spinal stenosis is low. A recent series of 443 lumbar spines yielded only 6 patients in 100 with relative stenosis and none with absolute stenosis.20 Lateral recess stenosis is more common. In the same series, a trefoil vertebral canal was found in 15% of the examined vertebrae and the same incidence was found in an earlier study.21 In developmental stenosis, the laminae, pedicles and posterior articular processes are increased in size (Fig. 35.1). The latter is a vertebral displacement with an intact neural arch. Although the exact mechanism is not fully understood, the combination of disc degeneration,22 general joint laxity,23 increased mechanical stress24 and structural abnormalities of laminae and facet25 may precipitate forward displacement of the whole vertebra. The common denominator in the development of degenerative vertebral slippage is loss of the normal coronal orientation of the facet joints. Several studies showed a significant increase in sagittal facet joint orientation in patients with degenerative spondylolisthesis, compared with a normal population.26–28 Association with narrowing of the intervertebral joint space and development of osteoarthrosis of the facets then leads to forward vertebral subluxation.29 Later on, buckling and hypertrophy of the ligamentum flavum may supervene.30 This results in stenosis between the lamina and the posterior border of the underlying vertebra (Figs 35.2 and 35.3).31,32 The condition occurs mostly after the age of 50 years, is 4–6 times more common in women than in men, and most frequently affects the L4–L5 level.33,34 The displacement is usually moderate, less than or equal to one-third of the anteroposterior diameter of the superior border of the adjacent vertebral body.35 The displacement does not progress continuously but is arrested by further degenerative changes of the intervertebral and facet joints.36 The mechanisms that underlie the clinical symptoms in spinal stenosis are complex and poorly understood. There is pressure not only on the dural sac and nerve roots but also on the adjacent blood supply. Therefore, arterial obstruction, venous hypertension and pressure–traction on nerve roots, dura and sinuvertebral nerves are all believed to be of importance.13,37–40 In patients with degenerative spondylolisthesis, back pain is the most common complaint and is probably caused by overstretching of the facet capsules. Often the pain is episodic or chronic for many years. Patients usually report that their symptoms vary as a function of imposed posture and pain frequently worsens over the course of the day.41 The most significant symptom of lumbar stenosis is neurogenic intermittent claudication, or ‘pseudoclaudication’.42–44 As in true intermittent claudication, the pain is brought on by walking and relieved by rest. However, pseudoclaudication is believed to be secondary to mechanical compression of the spinal content, whereas intermittent claudication is the result of vascular insufficiency (Table 35.1).45 The two conditions can be distinguished by their symptoms. Table 35.1 Differences between neurogenic and vascular claudication In neurogenic claudication, leg pain is usually bilateral, poorly localized and associated with paraesthesia and numbness. Although the pain is usually provoked during walking, it does not disappear on standing still, which can even aggravate the situation.46 The pain is relieved only by adopting a stooped posture or by sitting.47,48 The main characteristic of neurogenic claudication is thus that it is generated by posture rather than by exercise. This postural mechanism explains why a patient may have the same symptoms during recumbency in the prone position and does not usually experience symptoms while riding a bike.49–51 At its most extreme, patients may report the need to sleep in the fetal position to relieve leg symptoms. With extreme stenosis, interference with bladder and bowel control can occur but, unlike the acute and often devastating bladder and bowel symptoms of cauda equina syndrome in lumbar disk herniation, spinal stenosis often has an insidious and subtle presentation.52 The patient may have difficulty in standing erect and adopts a ‘simian stance’ with flattened lumbar lordosis and hips and knees slightly flexed.53 Extension is limited and may provoke pain in the legs, especially after the extended posture is maintained for a certain length of time. There is symmetrical and painless limitation of both side flexions. As a rule, flexion does not provoke symptoms in the legs but rather relieves the leg pain.54–56 This can be explained by the fact that extension significantly decreases both mid-sagittal and subarticular sagittal diameter, whereas flexion has the opposite effect.57,58 Straight leg raising is usually normal, as are reflexes. Because the lesion involves different levels and the compression of the roots is intermittent, there is often no demonstrable sensory deficit or muscle weakness. If there is some objective weakness, it is normally situated in the muscles supplied by the fifth lumbar and first sacral nerves.16 Plain radiographs are sufficient to suggest the possibility of a narrow canal. Short pedicles and narrow intervertebral foramina are clearly demonstrable on a suitable lateral projection (Fig. 35.4).59 Hypertrophy of facets, disc resorption, retrolisthesis and degenerative spondylolisthesis can also be seen easily on the same views.60,61 On the plain anteroposterior projections (Fig. 35.5), hypertrophy of the pedicles (A), hypertrophic articular processes (D), small interlaminar spaces (C) and some sagittalization of the articular facets may be seen (B).62,63 Fig 35.5 Interpretation of radiographic appearances of spinal stenosis (frontal projection): see text. However, it is as well to remember that these radiographic findings are non-specific and can also be seen in asymptomatic individuals. In patients with clinical features, there is no correlation between symptoms and signs and the severity of the radiographic appearances.64 They are helpful only in supporting the clinical diagnosis. In a symptomatic patient, the evaluation of spinal stenosis can best be made by magnetic resonance imaging (MRI), which has largely replaced computed tomography (CT) and CT-myelography.65 MRI is a non-invasive technique that can define the typical factors contributing to the symptoms of spinal stenosis: significant constriction of the cauda equina associated with a diminished cross-sectional area of the vertebral canal, apparent thickening and buckling of the ligamentum flavum, and hypertrophy of adjacent facet joints.66 The natural course of spinal stenosis can vary, but in most patients it is a relatively stable disorder, with severe disability and neurological deficits developing over time and not rapidly. A recent survey reported that, in 80% of patients treated conservatively, symptoms did not worsen over 4 years.67 For patients with moderate or severe symptoms, different conservative and surgical treatment modalities are recommended. Non-operative, conservative treatment should be used first and includes relative rest and non-steroidal anti-inflammatory drugs.68–70 Back school instruction is given in activities of daily living and pelvic tilting exercises to reduce lumbar lordosis (see p. 588).71,72 Epidural injections may be tried but reports of their efficiency are mixed.73 Some data suggest that epidural injection of corticosteroids relieves leg pain for a limited time but has no effect on functional status or the need for surgery after 1 year.74 If the patient does not respond to conservative treatment or if there is progressive deterioration, surgery is required. Decompression of the stenotic area is the usual procedure.75,76 Some advocate spinal fusion after the decompression, in order to avoid postsurgical instability.77,78 The surgical outcome is good to excellent in 45–80% of patients operated on.79–84 Patients with a preoperative duration of symptoms of less than 4 years, with no preoperative back pain and without previous back surgery tend to have a better outcome.85–88 The radicular canal is at the lateral aspect of the spinal canal. It begins at the point where the nerve root sheath emerges from the dural sac and ends at the intervertebral foramen. Its posterior border is formed by the ligamentum flavum, superior articular process and lamina. The anterior border is the posterior aspect of vertebral body and disc, both covered by the posterior longitudinal ligament. The dural sac forms the medial wall and the internal aspect of the pedicle the lateral wall.89 The radicular canal can be classified into three zones (Fig. 35.6): the entrance zone is medial and anterior to the superior articular process; the midzone is located under the pars interarticularis of the lamina and below the pedicle; the exit zone is the area surrounding the intervertebral foramen.89 Compression of the nerve root can be the result of different mechanisms: subarticular entrapment, pedicular kinking, or foraminal impingement due to posterior joint subluxation (MacNab90: pp. 98–104). Cyriax91 believed that the main reason for the compression lies in the fact that the posterior longitudinal ligament and the outer layers of the degenerated disc bulge in the upright position, so impinging on the nearby nerve root. Recently, stenosis as a result of surgical procedures has become more frequent. This type of stenosis is related to the entrance zone. Emerging from the dural sac, the nerve root passes between the posterior aspect of disc and vertebral body and the anteromedial aspect of the superior articular facet of the same vertebra. Hypertrophic osteoarthrosis of the facet joint, especially involving the superior articular process, may considerably diminish the distance between both borders and thus compress the nerve root,92 although there may be an additional compression by a thickened and folded posterior longitudinal ligament91,93 (this is suggested by the observation that the pain is not constant but dependent on posture94). The mechanism is as follows: increasing degeneration and anterior migration of discal tissue cause diminution of the intervertebral space and eventually lead to disc resorption and formation of gross anterior osteophytes. Consequently, the posterior longitudinal ligament, which spanned a joint 1 cm high, is now too long and will therefore bulge, especially in the standing or lordotic position.95 The thickened and buckling ligament can then exert pressure against the nerve root, especially if the recess is narrowed by the hypertrophic superior facet. Pain in the upright posture which disappears on sitting and bending is better explained in this way than by postulating a static subarticular entrapment. Cyriax called this mechanism the mushroom phenomenon, because of the characteristic radiographic appearances of a long-standing anterior shift of disc material, which results in a marked narrowing of the joint space and gross beak-like osteophytes (Fig. 35.8). This is a midzone stenosis. The mechanism is as follows: disc degeneration causes considerable narrowing of the intervertebral space and the upper vertebral body descends. The pedicle may then press on the nerve root (Fig. 35.9), especially if the narrowing is asymmetrical, and cause inflammation and oedema, which will give rise to symptoms. An alternative source of the symptoms is that the nerve root is trapped in the gutter formed by the pedicle and the posterolateral aspect of the degenerated and bulging disc. This occurs at the exit zone in the intervertebral foramen. In vitro anatomical and biomechanical studies of normal motion segments showed that the intervertebral foramen of the lumbar spine narrows significantly during extension and ipsilateral bending, and increases during flexion.96 With disc degeneration and subsequent loss of intervertebral height, the facet joints are forced into a permanent extension position: they move telescopically in relation to each other with the inferior facet moving downwards. Because of the inclination of the joints, a downward movement is accompanied by a backward one and a small retrolisthesis is produced. This further narrows the foramen, and the nerve root, which lies in close relationship to the tip of the superior articular process of the underlying vertebra, may become compressed between the tip of the subluxated (and eventually enlarged) superior facet, and the pedicle or body of the vertebra above (Fig. 35.10).
The stenotic concept

Introduction
Definitions
Incidence
Spinal stenosis
Pathological changes
Symptoms
Neurogenic
Vascular
Localization
Vague, including the back
Mostly in the calf
Paraesthesia
Present
Absent
Walking
Worse
Worse
Standing still
Worse
Better
Bending
Better
No change
Cycling
No change
Worse
Lying prone
Worse
No change
Signs
Radiography
Treatment
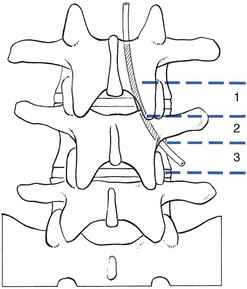
Lateral recess stenosis
Pathological changes
Subarticular entrapment (Fig. 35.7)
Pedicular kinking
Foraminal encroachment
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The stenotic concept