8. The Person–Environment–Occupational Performance (PEOP) Model
Charles Christiansen, Carolyn M. Baum and Julie Bass
Overview
This chapter summarizes the history and evolution of the Person–Environment–Occupational Performance (PEOP) Model, a model for practice first conceived during the 1980s in the USA. As a guide to occupational therapy intervention, the PEOP Model can be considered a transactive systems model. The model focuses on the client and on relevant intrinsic and extrinsic influences on the performance of everyday occupations. It can be applied to individuals, groups (or organizations) and populations. The PEOP Model has characteristics that are similar to other social ecological models, in that it identifies three relevant domains of knowledge for occupational therapy practice:
• the person (intrinsic factors)
• the person’s situation or context, including the relevant physical and social environment (extrinsic factors)
• the occupations of importance to the client’s well-being (activities, tasks and roles).
It is transactive in that it views everyday occupations as being affected by, and affecting, the client and the client’s context. It is client-centred in that it values and requires the active involvement of the client in determining intervention goals. It is different from other models because it makes the intrinsic, extrinsic and occupational factors explicit and applies them at the person, organizational and population levels.
The PEOP Model:
• is client-centred
• applies to individuals, groups and populations
• is intended to be top-down, focusing first on the situations of clients
• allows the practitioner to organize current knowledge of the intrinsic and extrinsic factors in their interventions
• uses a systems perspective
• serves as a guide to creating a complete occupational profile of the client
• values collaboration with the client, with important others within the client’s social circle, and other professionals concerned about the client’s well-being
• works to achieve a match between the client’s goals and the goals of occupational therapy intervention
• believes that outcomes must be related to well-being and quality of life
• incorporates the three components of evidence-based practice: the best evidence from research, professional and clinical expertise, and the client’s unique values and circumstances.
Introduction: origins and aim of the PEOP Model
In 1985 work began in the mountains of Colorado on what was to become the PEOP Model. At the time, there was a growing awareness that it was necessary to organize the knowledge that was being used by occupational therapists in a manner that would identify, clarify and emphasize the unique contribution of occupational therapy to the health and well-being of individuals, groups and populations. We knew that occupational therapy could provide practical and relevant interventions that enabled people to preserve or improve the quality of their lives. Yet, at that time, the most influential textbooks in the field were continuing to organize their content using a biomedical approach that resembled the diagnosis and pathology-focused approach of allopathic medicine. Influenced by writers from medicine who were calling for more health-oriented approaches (e.g. Engel 1977), as well as writers from occupational therapy who openly lamented the field’s apparent divergence from ideas central to its founding (e.g. Shannon, 1977), we set about reframing the organizing structure for knowledge relevant to occupational therapy theory and practice. We intended to propose a model that would provide practitioners with an intuitive and organized way to understand the areas relevant to supporting people’s ability to perform or do the activities, tasks and roles necessary for everyday living. Through creating such a framework, we aimed to facilitate thinking in ways that would guide assessment, planning and the delivery of interventions. Our goal was to have a model that would be relevant, regardless of the settings in which occupational therapists worked, the types of client they served, or the ages, life stages or diagnoses of those clients. We also felt that creating such a model would encourage a more balanced approach to care that would encourage therapists to plan intervention with a focus on the life situations of their clients. This focus, we surmised, would require that therapists consider the person-related and environment-related resources and barriers relevant to a full understanding of how to enable their clients to perform or accomplish the particular occupations necessary to live satisfying lives.
The PEOP Model is now in its third generation (Christiansen and Baum, 1991, Christiansen and Baum, 1997 and Baum and Christiansen, 2005) and continously being updated. During the years since its inception, the knowledge generated from occupational science, neuroscience, environmental science and other biological and social sciences has enabled us to refine and extend our original ideas and to provide a more solid scientific basis for the constructs we believe are central to understanding the occupational performance of humans. Throughout this process of elaboration, we have been influenced by many emerging ideas and innovations in healthcare, disability, social policy, technology, rehabilitation and public health. Although some terminology has changed, definitions have been revised, and new concepts have been added, the basic philosophical orientation of the model and its central features have remained consistent. This, we believe, indicates that we were successful in achieving a model that was not only conceptually sound, but straightforward in its ability to organize a knowledge base of information useful for practice.
The PEOP Model values collaboration
Because occupational therapy is based on a cooperative approach toward care (Meyer 1922), the PEOP Model was designed to facilitate the development of a collaborative intervention plan with the client and with other professionals. Use of the term ‘client’ is meant to apply, whether the intervention is directly with a patient, a well community-dwelling child or adult, or a family, or done in consultation with a physician, a social worker, a student, an architect, an employee, an organization or an entire community. Each of these ‘clients’ would seek the knowledge and skills of the occupational therapist to address issues that influence occupational performance or the ability of people to participate fully in their lives. Occupational therapists provide a unique knowledge and skill set that bridges the world of the client and the world of healthcare and includes other important social services in communities. A core assumption is that people cannot truly be well if they cannot participate fully in their lives.
Occupational performance
The concept of occupational performance has become the mainstay of the development of most models of occupational therapy. Occupational performance operates as a means of connecting the individual to roles and to the sociocultural environment (Reed & Sanderson 1999, p.93). We define occupational performance as the complex interactions between the person and the environments in which they carry out activities, tasks and roles that are meaningful or required of them (Baum & Christiansen 2005).
A systems perspective
The PEOP Model is a systems model, recognizing that the interaction of the person, environment and occupational performance elements is dynamic and reciprocal, and that the client must be central to the care-planning or intervention process. Only the client (whether person, family, organization or community) is able to determine what outcomes are most important and necessary.
Client-centred
In the traditional medical model it is the practitioner who determines the approach to care. The PEOP Model provides a bridge from the biomedical model to a sociocultural model and provides students and clinicians with a tool to organize evidence for use in practice. That is, it recognizes impairments when they limit performance participation but also views the client in context, including a consideration of the abilities and strengths that a client can use to enable performance, as well the environmental characteristics that provide support, whether those include places, people, policies or technologies. Ultimately, the comprehensive assessment of a client, what that client needs and wants to do, and the environment clients will inhabit collectively determine the interventions aimed at enabling the client to perform valued roles, activities and tasks that are central to living, whether these pertain to management of self and others, work or community engagement. A central theme of the PEOP Model is that, ultimately, the client determines the performance goals toward which therapy is targeted.
The PEOP Model is used as a guide to creating a complete occupational profile of the client, which includes information about the client’s perception of the current situation, and includes consideration of the client’s roles, interests, responsibilities and/or mission and values. The assessment and planning phase of care is grounded in evidence. We believe that clients should enter into the intervention phase with a clear understanding of the outcome that should ultimately result. Intervention must be a collaborative endeavour, with effort and commitment contributed through the partnership of the practitioner and the client.
Description of the model
Figure 8.1 provides a graphic representation of the model. This representation is intended to convey that occupational performance is determined not only by the nature of the activity, task or role to be performed, but also by the characteristics of the person or client (depicted as intrinsic factors) and the environment (depicted as extrinsic factors). Performance and participation always occur in context, and ultimately determine well-being and quality of life. It should be noted that, for a given situation or context, the applicability or importance of given intrinsic and extrinsic factors will vary. The model presupposes that a complete assessment to plan intervention will include a consideration of each of the factors.
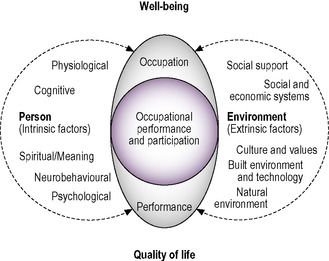 |
| Fig. 8.1 • The Person–Environment–Occupational Performance Model. Reprinted with permission from SLACK Incorporated. Christiansen, C.H., Baum, C.M., Bass, J., 2005. Occupational Therapy: Performance, Participation and Well-being, third ed. Slack Inc. Thorofare, NJ. |
Using the PEOP Model to plan care
The PEOP Model visually represents the constructs that must come together to support both the practitioner and the client in developing a realistic and sequenced plan of care. Success in this process depends on the practitioner’s skills in forming a relationship with the client, asking the right questions, and being able to access the knowledge necessary to understanding the issues and options presented by the client’s occupational performance issues and goals. Using the PEOP Model involves a ‘top-down approach’, in that it first considers the individual in context, identifying the client’s roles, occupations and goals. The model requires the occupational therapist to use this context to address the personal performance capabilities/constraints and the environmental performance enablers/barriers that are central to the occupational performance of the individual.
Intrinsic factors
Intrinsic factors in the PEOP Model that are central to occupational performance are:
• physiological, including strength, endurance, flexibility, inactivity, stress, sleep, nutrition and health
• cognitive, including organization, reasoning, attention, awareness, executive function and memory, all necessary for task performance
• neurobehavioural, including somatosensory, olfactory, gustatory, visual, auditory, proprioceptive and tactile, as well as motor control, motor planning (praxis) and postural control
• psychological and emotional, including emotional state (affect), self-concept, self-esteem and sense of identity, self-efficacy and theory of mind (social awareness)
• spiritual: that which brings meaning.
Extrinsic factors
Extrinsic factors in the PEOP Model that are central to occupational performance are:
• social support, practical or instrumental support and informational support
• societal, including interpersonal relationships (groups), social and economic systems and their receptivity (policies and practices) to supporting participation, laws
• cultural, including values, beliefs, customs, use of time
• the built environment, including physical properties, tools, assistive technology, design and the natural environment, covering geography, terrain, climate and air quality.
Situational analysis
In order to incorporate key elements of planning, the occupational therapist completes a situational analysis. This analysis seeks information from the client by interview and by employing assessments that give the practitioner a clear understanding of constraints and/or barriers that may limit the person’s activity and participation. As well, the practitioner will gain insight into barriers and environmental enablers that will limit or support the individual in doing the things he or she wants and needs to do.
There are a number of key elements of a plan of care in the PEOP Model. These client-centred elements change, depending on whether the client is a person, an organization, or the community, as reflected in a population approach. Each will be discussed.
The following situational analyses were designed to help the practitioner organize information to address the issues of individuals, of organizations and of communities. In each situational analysis, evidence underpins the practitioner’s decisions as to what measures to include and which interventions to employ. All professionals are held to a standard — the expectation of competent practice using methods that have been objectively shown to be effective. Evidence thus becomes the filter through which clinical decisions about the type of evaluation or assessment and the interventions that will support the client in achieving their goals will be made.
Related posts:
 Occupational science
An introduction to the psychodynamic frame of reference
An introduction to conceptual models of practice and frames of reference
Applying the Canadian Model of Occupational Performance
The cognitive behavioural frame of reference
The biomechanical frame of reference in occupational therapy
Occupational science
An introduction to the psychodynamic frame of reference
An introduction to conceptual models of practice and frames of reference
Applying the Canadian Model of Occupational Performance
The cognitive behavioural frame of reference
The biomechanical frame of reference in occupational therapy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


