7. Applying the Canadian Model of Occupational Performance
Thelma Sumsion, Lesley Tischler-Draper and Sheila Heinicke
Overview
Client-centred practice now forms the foundation for interactions with people in many countries. Canadian occupational therapists created a model in the early 1980s to support the use of this approach and have continued to develop both the model and its application in a variety of clinical settings (see Chapter 11). Colleagues in many other countries are also developing expertise in the application of both the model and the outcome measure that arose from it. This chapter aims to ensure that students, therapists and educators understand the origins of this approach and how to apply the outcome measure. To accomplish this goal, a historical overview of the Canadian Model of Occupational Performance (CMOP) and the emergence of the Canadian Model of Occupational Performance and Engagement (CMOP-E), with a discussion of key components, has been provided. An overview of the Canadian Occupational Performance Measure (COPM) that arose from the model is also presented, together with detailed information about its application with two clients. In order to give a practical illustration of the model and outcome measure, particular reference is made to its application in a mental health setting.
This chapter examines:
• the development of the Canadian Model of Occupational Performance (CMOP)
• the emergence of the Canadian Model of Occupational Performance and Engagement (CMOP-E)
• the links between the CMOP and the Canadian Occupational Performance Measure (COPM)
and provides:
• a description of the COPM
• two case examples showing the application of the COPM.
Introduction
This chapter aims to present the story of the development of the CMOP from a historical perspective, including the many revisions that have been made to the model and its consistent components, as well as its current format. The chapter then proceeds to apply the components of the model, and the outcome measure that arose from it, to two case studies.
Model of Occupational Performance
Historical perspective
The Model of Occupational Performance forms the basis of client-centred practice in occupational therapy in Canada and increasingly in other countries. A Canadian taskforce, jointly funded by the Canadian Association of Occupational Therapists (CAOT) and the Department of National Health and Welfare, developed the original Model of Occupational Performance that was based on the work of Reed and Sanderson (Law et al 1990).
In 1983 Reed and Sanderson proposed a Human Occupation Model that contained four concentric circles. The individual was in the centre of the model and therefore, by implication, was at the centre of the intervention. The second circle contained the five performance components or skills, which are ‘areas a person develops to facilitate carrying out occupations’ (p.11). These components are
• motor — composed of the neuromuscular/skeletal system
• sensory — the primary means of gaining information from the outside world
• cognitive — attending to tasks, problem-solving and memory
• intrapersonal — coping with reality and distinguishing it from non-reality
• interpersonal — relating to others in dyads or groups (pp.13–14).
Human occupation was shown in the third circle and was broken down into:
• self-maintenance — activities done to maintain the person’s health and well-being in the environment
• productivity — activities or tasks done to enable the person to provide support to self and others
• leisure — activities or tasks done for enjoyment or renewal (p.10).
These occupations are the focus of occupational therapy. The outer circle was labelled ‘adaptation to and with the environment’ (p.6). People interact with the environment by using their occupational skills. In summary, this model outlined that the goal of occupational therapy was to promote or maintain health through performance of occupational skills throughout the lifespan, and in all stages of health and illness.
The early Canadian model (the Model of Occupational Performance) clearly replicated some aspects of Reed and Sanderson’s (1983) work but also proposed other unique elements. This original version of the Model of Occupational Performance helped to make the theory more accessible, as it provided a background for practice. This model placed the individual in the centre of many interacting spheres. The middle sphere depicted the three areas of a person’s occupational performance, which were self-care, productivity and leisure. The performance components of the individual were featured in the centre sphere. These components were spiritual, physical, sociocultural and mental. This model supported a holistic view and recognized the worth of the individual (Townsend 1993). In addition, ‘the integration and execution of occupational performance is defined and shaped by the individual’s social, physical and cultural environments’ (Townsend et al 1990, p.71) which were joined by the political, economic and legal environments in 1993 (CAOT and Health Canada 1993).
McColl and Pranger (1994) criticized this original model, saying it was developed in an unorthodox manner. They also expressed concerns that the model was limited, as it discussed occupational performance but not occupation. No empirical support was offered for the assumptions underlying the original model (McColl & Pranger 1994). In it, ‘occupational performance looked static, the environment appeared to be external and unconnected to the person, and spirituality was depicted as a performance component parallel to mental, physical and socio-cultural performance’ (CAOT 1997, p.30). The model was referred to as the Canadian Occupational Performance Model but this was not an official term. However, this issue was addressed in 1997 when the model was officially named (CAOT 1997). CAOT also recognized that there were problems with this model and these were addressed in the revised version.
Revised model
To address the above issues, the name of the model was changed in 1997 to the Canadian Model of Occupational Performance (CMOP). This version is shown in Figure 7.1 and presents many new concepts. ‘CMOP is a social model that places the person in a social/environmental context rather than locating the environment outside of the person’ (Sumsion 1999, p.7). Occupational performance is the result of interaction and interdependence between person, environment and occupation (Townsend 1998). The revised presentation is now an interactive model showing relationships between persons, environment and occupation (CAOT 1997).
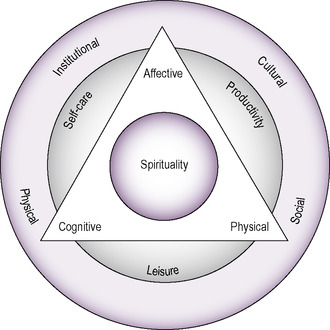 |
| Fig. 7.1 • The Canadian Model of Occupational Performance (CMOP). Reprinted from Enabling Occupation: An Occupational Perspective (1997; 2002) by the Canadian Association of Occupational Therapists, with permission of CAOT Publications ACE, Ottawa, Ontario. |
Occupation is shown as a circle overlain by a triangle representing the doing (physical), feeling (affective) and thinking (cognitive) components of the person. The points of the triangle also extend beyond the circle of occupation to interact with the environment (Townsend 1998). In reality, therapists know that the interaction between people, their roles and the environment is quite dynamic and must constantly accommodate a variety of changes. The revised model allows for change and focuses on the interaction of the elements.
Self-care, productivity and leisure remain as performance components and are now considered to be the key components of occupation. The central sphere now focuses on the person, including their spiritual, affective, cognitive and physical components. The environments included in the outer sphere are physical, institutional, cultural and social (Canadian Association of Occupational Therapists, 1997 and Sumsion, 1999).
Components of the model
Occupation
The components of occupation are self-care, productivity and leisure. CAOT defines self-care as ‘occupations for looking after the self’ (CAOT 1997, p.37). Productivity is defined as ‘occupations that make a social or economic contribution or that provide for economic sustenance’ (CAOT 1997, p.37). Leisure is defined as occupations for enjoyment (CAOT 1997, p.37), which built on the definition presented by Reed and Sanderson (1983).
Performance
The 1997 CAOT document reformulated the performance components. The original four components — mental, physical, spiritual and sociocultural — could potentially be viewed in isolation from each other, and have therefore been developed into three components — affective, physical and cognitive — which facilitate interaction. The revised performance components were defined as follows:
• affective — (feeling): the domain that comprises all social and emotional functions and includes both interpersonal and intrapersonal factors
• physical — (doing): the domain that comprises all sensory, motor and sensorimotor functions
• cognitive — (thinking): the domain that comprises all mental functions, both cognitive and intellectual, and includes, among other things, perception, concentration, memory, comprehension, judgement and reasoning (CAOT 1997, p.44).
Occupational therapists are familiar with the affective, physical and cognitive performance components. However, the spiritual component, which remains central to the model, provides additional challenges and continues to lack a consistent definition (Sumsion, 1999, Whalley Hammell, 2001 and McColl, 2003). Its position is justified, as spirituality ‘resides in persons, is shaped by the environment and gives meaning to occupation’ (CAOT 1997, p.33), and in reality is a part of all of the components of the model and is necessary to maintain life (Rebeiro, 2001a and Sumsion, 1999). However, debate about the role of the occupational therapist continues through a discussion of whether occupation, rather than spirituality, should be the therapist’s primary concern (Unruh et al 2002).
Environments
The original Model of Occupational Performance presented the cultural, physical and social environments and considered their impact on the person. The revised version of the CMOP (Fig. 7.1) has maintained the cultural, physical and social environments and has encompassed the economic, legal and political environments within the institutional environment (Sumsion 1999).
Everyone encompasses a number of different cultures, which may explain why the cultural environment fluctuates and is different for each individual (Sumsion 1997). Many issues that have an impact on a therapeutic intervention are culturally determined, including beliefs, values, customs, patterns of authority, how decisions are made and individual roles (Bonder 2001).
The physical environment can be seen as both a barrier and a support for individuals’ participation in their community. Issues such as physical accessibility and proximity to family and support services must all be considered (O’Brien et al 2002). The physical environment is the traditional domain of occupational therapists and hence is the one with which they are most familiar (Sumsion 1999).
The social environment is composed of social groups such as family, co-workers and friends and their roles, as well as occupational forms such as playing cards or jogging (Sumsion, 1997, Sumsion, 1999 and Kielhofner, 2008). This environment contains both people and social cues. The latter are implemented as we learn the rules and roles that govern behaviour (Hagedorn 2000). For those with mental illness, the social environment may limit engagement in occupation (Rebeiro 2001b).
The institutional environment includes legal elements that often overlap with the economic one as control of funds and who makes financial decisions often become legal matters (Sumsion 1997). The political and economic environments are also often connected and have the potential to expand well beyond the boundaries of this discussion. In reality, the economic environment overlaps with all other environments, including the political one, where issues such as accessible transport and buildings are of particular concern to occupational therapists (Sumsion 1997). The institutional environment has been shown to shape occupational performance, which reinforces its importance to occupational therapists (Dyck & Jongbloed 2000).
The environment is an underused resource and therefore it is important that all environments are evaluated and altered so people can function to the best of their abilities (Dressler & MacRae 1998). Throughout the lifespan, clients will change their self-perception according to the meaning they give to both occupation and the surrounding environments (CAOT 1997). Therefore it is important for occupational therapists to remember that occupational performance is where the unique being, the environment and occupation overlap and that all environments are of equal importance in therapeutic considerations (Law et al 1996).
Current model
In 2007 the CAOT released Enabling II as a companion document to Enabling Occupation (CAOT 1997). This publication contained a revised version of the CMOP known as the Canadian Model of Occupational Performance and Engagement (CMOP-E). This version of the model has added increased emphasis to the concept of engagement signified by the ‘E’. This is accomplished through the addition of a transverse section (Fig. 7.2) that presents occupation as ‘our core domain of interest’ (Townsend and Polatajko 2007, p.24). The authors further state that ‘we are only concerned with what is related to human occupation and its connection with the occupational person and the occupational influences of the environment’ (Townsend and Polatajko 2007, p.24).
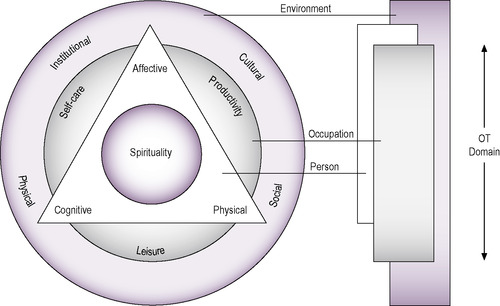 |
| Fig. 7.2 • The Canadian Model of Occupational Performance and Engagement (CMOP-E). Reprinted from Townsend, E., Polatajko, H., 2007. Enabling Occupation II: Advancing an Occupational Therapy Vision for Health, Well-being and Justice Through Occupation, p.23, with permission from CAOT Publications ACE, Ottawa, Ontario. |
Application of the model
The CMOP and recently presented CMOP-E now truly form the basis of occupational therapy practice in Canada. Both the components and the model as a whole are the focus of research and local and national conference presentations.
At one end of the lifespan the model has been used as a framework to clarify a range of facts involved in feeding infants with congenital heart disease (Imms 2001). At the other it has been applied to work with community-dwelling older adults (Griffith et al 2007), where the application of components of the model enabled therapists to understand the person’s occupational limitations and how these affected occupational performance.
Godfrey (2000) saw a clear link between the quality of a person’s life and how they interact with the environment. In this discussion, the CMOP was used to illustrate how changes in one aspect of the system, such as the person or their occupation, affect all other aspects. However, concern was expressed that the model was not accompanied by a clear framework to guide practice. The need for more literature related to the application of the model in settings outside of Canada was also stressed (Clarke 2003). The CMOP-E attempts to address some of these concerns but there is still more work to be done.
Applying the model in a clinical setting
The CMOP, with a person at its centre, conveys occupational therapy’s client-centred perspective (CAOT 1997). All therapists in Britain, as well as in Canada, are expected to provide services that are client-centred, as stated in the Code of Ethics and Professional Conduct (College of Occupational Therapists 2005). Therefore, any therapist committed to a client-centred approach would do well to explore this model. There are other models and associated assessments that are also client-centred (see Chapters 6 and 10); however, the appeal of the Canadian model lies in its simplicity and comprehensiveness. The Canadian model provides therapists with a simple, clear, conceptual framework for thinking about the person, with the person, throughout the occupational therapy process. Central to this model is the concept of occupational performance, which is an occupational therapist’s principal domain of concern and expertise (Law et al 2005).
The link between the CMOP-E and the Canadian Occupational Performance Measure
Both the CMOP and CMOP-E are client-centred models for use in occupational therapy intervention with people with all types of health impairment across the lifespan. They look at each individual person’s cognitive, affective and physical abilities within the context of the person’s environment. A person’s individual and unique spiritual nature is embedded within all aspects of the model.
Related posts:
 Occupational science
An introduction to the psychodynamic frame of reference
An introduction to conceptual models of practice and frames of reference
The Person–Environment–Occupational Performance (PEOP) Model
The cognitive behavioural frame of reference
The biomechanical frame of reference in occupational therapy
Occupational science
An introduction to the psychodynamic frame of reference
An introduction to conceptual models of practice and frames of reference
The Person–Environment–Occupational Performance (PEOP) Model
The cognitive behavioural frame of reference
The biomechanical frame of reference in occupational therapy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


