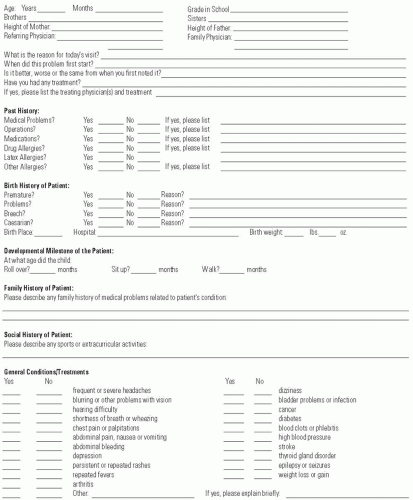
The pediatric orthopaedic examination can vary considerably depending on the age of the child, chief complaint, magnitude of the problem, and the level of concern of the patient and family. In all situations, the clinician should respect the dignity of the child, family, and other health care professionals that accompany the patient. It is important for the child to feel comfortable in the office environment, so having a bright child-friendly waiting room with toys and age-appropriate books can be very beneficial. It is helpful to have the family or caregivers fill out a patient intake form (Fig. 4-1) prior to the visit to expedite the history so the clinician can focus on engaging the child and gaining the child’s trust. In some cases, this may be the most important aspect of the pediatric orthopaedic examination, as it is almost impossible to perform an adequate examination on an uncooperative child. Currently, the paper chart is gradually being replaced by the electronic medical record (EMR). In cases where the EMR is utilized, patients and their families can fill out the patient intake form electronically at home through a security enable portal, or through special computer kiosks, set up in the waiting room. Many hospitals, including ours, are mandating that patients or families fill out a pain assessment form such as the Wong-Baker FACES pain rating scale.
Recent studies have shown that clinician-patient communication underlies successful medical care, yet medical training has paid little attention to the importance of developing communication skills. Research has shown that improved communication improves diagnostic accuracy, fosters shared decision making, and increases the likelihood that the patient will follow the treatment recommendations. In addition, patient and clinician satisfaction increases and the risks of malpractice litigation decrease. The American Academy of Orthopaedic Surgeons (AAOS) has developed the “Clinician-Patient Communication to Enhance Health Outcomes Workshop” to address communication skills.
The AAOS approach identifies the different goals of the clinician and patient and emphasizes how they can all be addressed with improved communication. While the clinician wants to solve the problem with the “find it” and “fix it” approach, the patient has already made a self-diagnosis and wants the clinician to address an agenda of concerns including the self-diagnosis. To achieve the medical goals, the clinician needs to use the “4 Es” of communication skills: engage, empathize, educate, and enlist. To “find it,” the clinician must engage and empathize with the patient and not interrupt them while they are explaining their agenda. If this person-to-person or professional-partner engagement is attained, the accuracy of the diagnosis is improved and the “fix it” is achieved by improved patient education and enlisting the patient in shared decision making in the treatment. Improved communication results in improved patient outcomes. In today’s world, parents and young people expect to be heard, and their input often helps the clinician work with them.
The clinician begins by introducing himself or herself to the patient and family. If a resident physician or medical student accompanies the clinician into the exam room, it is important to introduce them and explain that they are learning. The clinician sits down to make direct eye contact with the child and listens attentively while taking an accurate history from the patient, family, and caregivers. Although a brief history and limited physical examination may be appropriate for a 5-year-old boy with a torus fracture, a complete history and physical examination are necessary to evaluate a 2-year-old boy who is still not walking.
HISTORY
The history always should begin with the chief complaint, a sentence or short statement in the exact words of the patient. If the patient is nonverbal or not yet talking, the chief complaint can be recorded in the exact words of the family or caregivers.
The history of present illness includes the details of how and when the chief complaint started and whether the symptoms are constant or intermittent. The clinician asks how the symptoms have evolved and if there are certain circumstances that aggravate the symptoms, such as exercise, or certain circumstances that relieve the symptoms, such as rest. It is important to document if any prior treatment has been recommended or rendered.
FIGURE 4-1. Patient intake form. This form, when filled out by the patient or family, prior to the office visit can save valuable time while conducting the history and physical examination.
The past medical history includes any prior major illnesses, hospitalizations, operations, and if the patient is taking any medications. The patient’s medications are reconciled and the patient’s allergies are recorded, particularly any allergies to medications.
The developmental history includes the details concerning the pregnancy, delivery, and perinatal course. Any complications associated with this pregnancy or any prior pregnancies are documented. Any problems associated with the delivery, such as an emergency cesarean section, or the newborn period, such as transfer to the Neonatal Intensive Care Unit (NICU), are noted. The clinician asks the family if anyone has raised concerns about developmental delay and records the developmental milestones, including when the child first sat, pulled to standing, cruised around furniture, walked independently, and developed handedness.
The family history focuses mainly on the immediate family including siblings, parents, grandparents, and any other close relatives. The clinician asks if any family members had a similar problem or a major illness.
The review of systems includes a general medical overview with questions about each system, such as the respiratory, cardiovascular, or genitourinary systems, to detect any other medical problems. Detecting a medical problem that may be associated with the chief complaint may lead directly to diagnose the problem (e.g., a patient with scoliosis that has a genitourinary problem).
The personal and social history reviews the living situation of the patient and may be extremely valuable in diagnosing the problem. The clinician asks about school and sports activities that interest the patient. Hobbies are important as they may reveal more about strengths, relationships, and other issues. Personal questions may be of value since smoking or secondary smoke in the home has been associated with several orthopaedic conditions such as Legg-Calvé-Perthes disease.
PHYSICAL EXAMINATION
The physical examination begins with the height and weight of the patient that is typically performed by the staff prior to placing the patient and family in the exam room. The clinician begins with a thorough examination of the skin, spine, upper and lower extremities, and a brief neurologic examination. The pediatric orthopaedic physical examination does not typically include the vital signs or a detailed examination of the head, eyes, ears, nose, throat, chest, heart, abdomen, or genitals, but any of these areas may require a detailed examination depending on the chief complaint. If there are concerns about certain aspects of the physical examination, these areas are examined in detail.
The history and physical examination varies considerably depending on the age of the patient. Infants and young children are unable to give a history, whereas an older child will often give a more accurate history than the family or caregivers. A teenage boy with a round back may have no concerns, but the family may be concerned that he will develop a severe hunchback deformity like his grandmother. Many pediatric orthopaedic conditions develop only in certain age groups, such as Legg-Calvé-Perthes disease, which typically develops in boys between 4 and 10 years of age. To highlight these important conditions that often develop only in certain age groups, this chapter is divided into three sections, according to the age of the patient. In all cases, once the history and physical examination is completed the clinician should communicate the findings with the referring primary care pediatrician or family physician.
The first section includes newborns, infants, and young children from birth to 4 years of age. These patients are usually unable to give an accurate history, so most of the history is obtained from the family or caregivers. The child may be apprehensive about going to the doctor and afraid of being examined. A toy or sticker may be helpful to divert the child’s focus away from the situation and allow the clinician to do a physical examination. The majority of the physical examination of a young child can be done in the mother’s lap. Once relaxed, the pertinent aspects of the examination can be performed on the examination table. If the infant is afraid and upset, a pause to allow bottle or breast feeding can be helpful. Once the clinician gains the respect and trust of the child and family, the physical examination can easily be performed.
The second section includes children from 4 to 10 years of age. These patients are not usually afraid and are interested in being a part of the examination. They will often correct their parents or caregivers about certain aspects of the history. They are typically calm and eager to participate and cooperate with the physical examination. In the age group, many children do not like removing their clothes or wearing a hospital gown. This situation can be avoided if the patient wears a T-shirt and a pair of shorts for the office visit. It is helpful to have extra pairs of gym shorts in the office to address this issue. Some children with special health needs are particularly resistant to anyone attempting to conduct a physical examination. In this situation, it is often helpful to tell the family exactly what you would like to accomplish. For example, the clinician can explain to the family that he or she would like to examine the child for scoliosis by having the child bend forward at the waist. The family can then place the child on a relative’s lap in the seated position while another family member bends the child forward at the waist to allow the clinician to examine the spine.
The third section includes children and adolescents from 10 to 18 years of age. These patients are usually very motivated to get better and will give an accurate history. Teenagers are also concerned about removing their clothes, so it is reassuring to know that they do not need to remove their T-shirt or shorts. Having extra pairs of gym shorts in the office is again helpful if they come to the office in jeans. If conducted appropriately and in a manner that respects their privacy, teenagers will allow the clinician to perform a complete physical examination. In all age groups, it saves time and avoids repetition to begin by reviewing the patient intake form that was filled out by the family, caregivers, or the patient prior to entering the examination room (Fig. 4-1).
THE ORTHOPAEDIC EXAMINATION FROM BIRTH TO 4 YEARS OF AGE
A 1-Month-Old Girl Is Referred for Evaluation of a Hip Click. A hip click was detected by the pediatrician shortly after birth and was still present at the 2-week appointment. The pediatrician was concerned that the baby might have developmental dysplasia of the hip (DDH) and referred her for evaluation. The history reveals that this is the mother’s first child and the pregnancy was normal, but the baby was in the breech presentation and they had to do a cesarean section. The birth weight was 3500 g (7 lb 11 oz) and the baby is otherwise healthy. There is no family history of DDH or hip problems.
A hip click may be a benign click that occurs when the ligamentum teres gets trapped between the femoral head and the acetabulum, or it may indicate a subluxatable or dislocatable hip as is seen in DDH. To distinguish between these two different entities, the clinician focuses on certain aspects of the history and physical examination that are associated with DDH. The birth history may be helpful as DDH is associated with primigravida mothers, oligohydramnios, breech presentations, and congenital muscular torticollis. Of these, the breech presentation is the most important because, even if born by cesarean section, if the infant was in the frank (single) breech presentation, the frequency of DDH is 20% to 30%. The developmental history may reveal that the infant has a neuromuscular disorder, such as arthrogryposis multiplex congenita. The family history is helpful because the frequency of DDH is higher when other family members have the disorder.
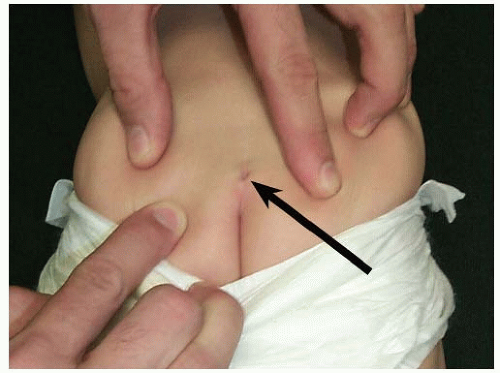
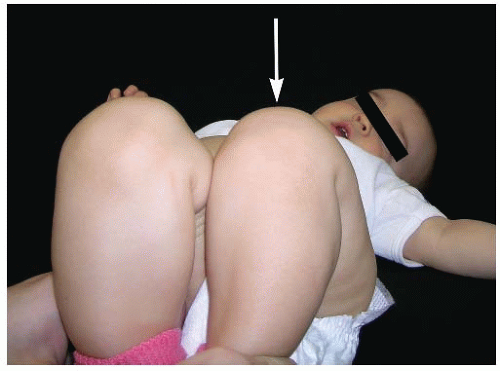
The physical examination can be started with the infant in the mother’s lap. In this position, the infant is comfortable, and the clinician can examine the range of motion of the hands, wrists, elbows, and shoulders. The neck range of motion is evaluated to rule out a contracture of the sternocleidomastoid muscle that may be secondary to a congenital muscular torticollis. The knees, ankles, and feet are examined to look for any anomalies that might be associated with DDH. The baby can then be placed prone over the mother’s shoulder, similar to the position for burping, while the clinician examines the spine. A sacral dimple or hairy patch above the natal cleft may be a sign of an underlying tethered spinal cord or lipomeningocele (Fig. 4-2). These disorders can cause partial paralysis of the lower extremities resulting in a paralytic hip dislocation. Finally, after the rest of the physical examination has been completed, the infant is placed on the examining table to examine the hips.
The key to the early diagnosis of DDH is the physical examination. The examination should be performed on a firm surface with the infant relaxed. If the infant is crying or upset with tensing of the muscles, the DDH may not be detected. In this situation, allow the family to feed or soothe the infant and begin the examination when the infant is calm and relaxed. Barlow recommends the examination be performed in two parts (1).
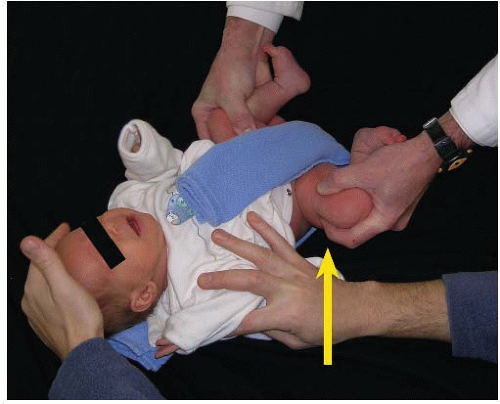
Part one is termed the “Ortolani maneuver.” To perform the Ortolani maneuver, each hip is examined individually while holding the pelvis steady with the other hand grasping the sacrum and pubic rami, or by using the other hand to hold and stabilize the opposite lower extremity and pelvis. The hips and knees are flexed to 90 degrees and the examiner places the long finger of each hand laterally, along the axis of the femur over the greater trochanter, and the thumb of each hand is placed on the inner side of the thigh opposite the lesser trochanter (Fig. 4-3). With the opposite hip and pelvis stabilized, the thigh of the hip to be examined is carried into abduction with forward pressure applied behind the greater trochanter by the long finger simultaneously. If the femoral head “clunks” forward into the acetabulum as the hip is abducted, the hip was dislocated. This maneuver, originally described by Ortolani, represents a “sign of entry” as the femoral head reduces into the acetabulum (Fig. 4-3). The Ortolani maneuver completes the first part of the Barlow test.
FIGURE 4-2. A sacral dimple (arrow) or hairy patch above the natal cleft may indicate an underlying tethered spinal cord or lipo meningocele.
FIGURE 4-3. The first part of the Barlow provocative test is the Ortolani maneuver. This test is performed by gently abducting the hip and pushing forward with the long finger over the greater trochanter (arrow). A clunk is palpated as the femoral head slides over the posterior lip into the acetabulum.
FIGURE 4-4. The second part of the Barlow provocative test involves applying pressure backward and outward with the thumb on the inner side of the thigh (arrow) while adducting the hip. If the femoral head clunks or slips out over the posterior lip of the acetabulum and back again after the pressure is released, the hip is unstable.
Part two of the Barlow test is termed the “provocative test.” To perform the Barlow provocative test, each hip is again examined individually. With the hips and knees flexed to 90 degrees, the examiner places the long finger of each hand laterally, along the axis of the femur over the greater trochanter, and the thumb of each hand is placed on the inner side of the thigh opposite the lesser trochanter. With the opposite hip and pelvis stabilized, the examiner applies pressure laterally and posteriorly with the thumb on the inner side of the thigh as the hip is adducted. The hip is unstable if the femoral head “clunks” or slides over the posterior lip of the acetabulum and relocates when the pressure is released. This maneuver represents a “sign of exit,” as the femoral head subluxates or dislocates from the acetabulum (Fig. 4-4). In a subluxating hip, the examiner may only detect a sliding sensation as the femoral head slides posteriorly in the acetabulum.
Although some investigators prefer to examine both hips simultaneously and others prefer to examine each hip separately, the most important aspect of the hip examination is to focus closely on each hip during the examination. The Barlow and Ortolani tests detect hip instability with ligamentous laxity, and although they are valuable during the neonatal period, they usually become negative by 3 months of age (2).
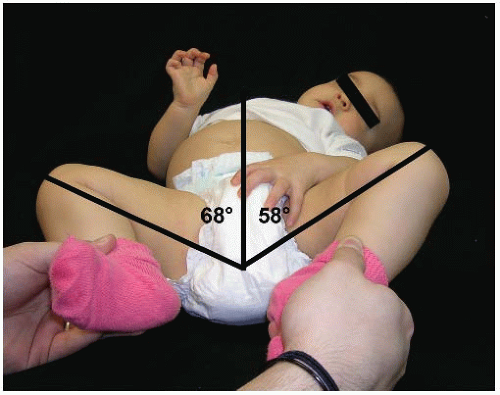
Once the infant is 3 months of age, if the femoral head is subluxated or dislocated the adductor and flexor muscles gradually develop contractures. The most common physical finding in older infants with DDH is limited abduction of the hip (Fig. 4-5). The limited abduction may be subtle, so it is important that the infant is positioned supine on a firm table. An infant with bilateral DDH may have symmetrically limited abduction that can only be detected by a careful examination. If the DDH is unilateral, the superolateral subluxation or dislocation of the femoral head causes a limb-length discrepancy that may be detected by the family or primary care physician. The subluxation or dislocation shortens the thigh causing an increased number of thigh folds (telescoping) compared with the uninvolved side. Although asymmetric thigh folds may be a normal finding, it alerts the clinician to the possibility of DDH. If the hips are flexed to 90 degrees, the subtle limblength discrepancy can be detected, as the knee on the side with DDH will be lower than the opposite side. This finding is termed a positive Galeazzi sign (Fig. 4-6). In this patient, the Ortolani maneuver is positive, so treatment with a Pavlik harness is recommended.
FIGURE 4-5. After 3 months of age, the most common physical finding in a patient with DDH is limited abduction of the hip. The asymmetry may be subtle as in this 15-month-old girl with a dislocated left hip. She has decreased abduction of the left hip (58 degrees) compared with the right (68 degrees).
A 2-Year-Old Boy Is Referred for Evaluation of Bowed Legs, Intoeing, and Tripping Over His Feet. The family first noted that his legs were bowed at 3 months of age. When he began walking at 16 months of age, the bowing was worse and his feet turned in. His feet now turn in so much that he trips over them falling frequently. The birth history reveals that he was born after a 40-week gestation via normal vaginal delivery with a birth weight of 4000 g (8 lb 13 oz). His developmental milestones reveal that he first sat at 7 months of age and began walking at 16 months of age. The family history reveals that the father wore a brace until he was 2 years old because his feet turned in.
FIGURE 4-6. The subtle femoral-length discrepancy that is seen with the hips flexed to 90 degrees is termed a positive Galeazzi sign. The Galeazzi sign is seen in DDH when the knee on the side with DDH is lower than the opposite side (arrow).
Since most 2-year-old children fall frequently, the clinician focuses on certain aspects of the history and physical examination to determine if the child has developmental delay. If so, he may have problems with coordination or retention of primitive reflexes that should have already disappeared. If the bowed legs represent physiologic bowing, one would expect the deformity to be improving by 2 years of age. If the intoeing is physiologic and represents a normal rotational variation, it will usually be symmetric and is often not noticed until the child begins walking. A unilateral problem, involving the foot, may indicate a mild clubfoot or a neurologic problem such as a tethered spinal cord. The clinician reviews the developmental history as most children will sit independently by 6 to 9 months of age, cruise (walk around furniture) by 10 to 14 months of age, and walk independently by 8 to 18 months of age (Table 4-1).
If the child has developmental delay, it is important to verify the details surrounding the birth to determine if the child was born premature, or if there were any perinatal complications. Premature infants born after 25 to 30 weeks of gestation, with a birth weight of 750 g (1 lb 10 oz) to 1500 g (3 lb 5 oz), have an increased incidence of cerebral palsy with spastic diplegia. The first sign of this disorder may occur when the family notes that their child is delayed in walking, limping, or tripping over his feet. When evaluating for developmental delay, it is valuable to ask if the infant is ambidextrous. Most children will remain ambidextrous until 18 months to 3 years of age (Table 4-1). If a child who is tripping over his left foot is also strongly right-handed, the birth history may reveal an intrauterine cerebral vascular accident causing cerebral palsy with spastic left hemiplegia.
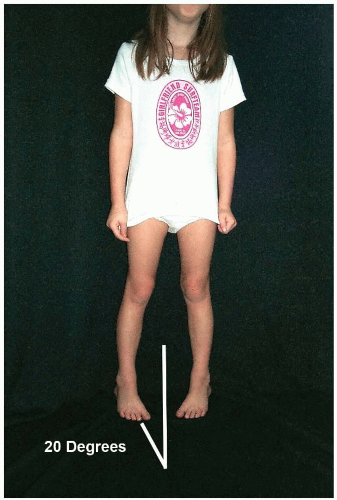
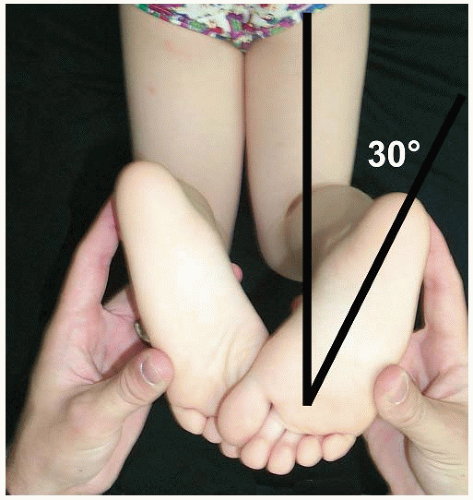
A 2-year-old boy may be apprehensive and uncomfortable in the exam room, so it may be helpful to begin the physical examination by opening the door and asking the family if they would like to take their son for a walk down the hall. Most 2-year-olds will enjoy walking away from the clinician and the exam room, but they often need to be carried back. While the family and child are walking down the hall, the clinician observes the child’s gait pattern including the foot-progression angle (3). The foot-progression angle is the angle between the axis of the foot and an imaginary straight line on the floor (Fig. 4-7). The axis of the foot is derived from a line connecting a bisector of the heel with the center of the second metatarsal head. The foot-progression angle in children 1 to 4 years of age can vary from 15 degrees of inward to 25 degrees of outward rotation. The gait pattern can also vary considerably in this age group, but usually it will be relatively symmetric, with a similar amount of time being spent in stance phase (60% of the gait cycle) and swing phase (40% of the gait cycle). Rotational values within two standard deviations of the mean are termed “rotational variations,” and values outside two standard deviations are termed “torsional deformities” (4).
TABLE 4-1 Average Developmental Achievement by Age
Age
Achievement
1 mo
Partial head control in prone position
2 mo
Good head control in prone position; partial head control in supine position
4 mo
Good head control in supine position; rolls over prone to supine
5 mo
Rolls over supine to prone
6 mo
When prone, lifts head and chest with weight on hands; sits with support
8 mo
Sits independently; reaches for toys
10 mo
Crawls; stands holding onto furniture
12 mo
Walks independently or with hand support
18 mo
Developing handedness
2 yr
Jumps; knows full name
3 yr
Goes upstairs alternating feet; stands momentarily on one foot; knows age and gender
4 yr
Hops on one foot; throws ball overhand
5 yr
Skips; dresses independently
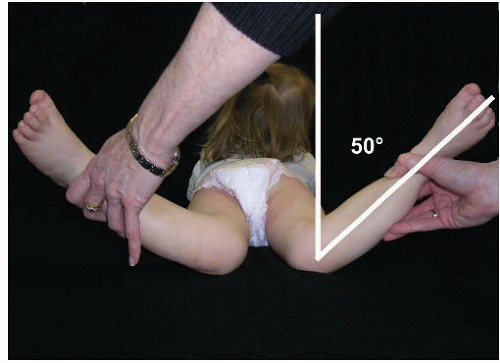
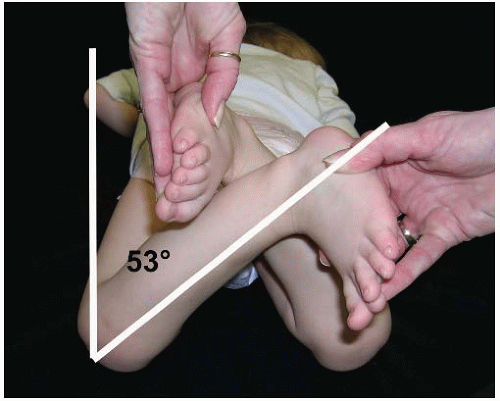
The degree and location of any rotational variations can be documented by creating a rotational profile (Table 4-2). The rotational profile includes the foot-progression angle, internal and external rotation of the hips, the thigh-foot angle, and any foot deformities. The foot-progression angle measures the degree of intoeing or outtoeing compared with an imaginary straight line on the floor (normal range 15 degrees inward to 25 degrees outward rotation) (Fig. 4-7). The internal and external rotation of the hips measures the femoral rotational variation or torsion. Measuring internal rotation of the hips in the prone position is a very important test in pediatric orthopaedics because many hip disorders can be detected by this examination including toxic synovitis, Legg-Calvé-Perthes disease, slipped capital femoral epiphysis (SCFE), and septic arthritis (Fig. 4-8). The normal range of internal rotation is 20 to 80 degrees (Fig. 4-8), and the normal range of external rotation is 25 to 80 degrees (Fig. 4-9). The thigh-foot angle is the angle between the axis of the thigh and the axis of the foot, with the patient prone and the knee flexed 90 degrees (Fig. 4-10). The thigh-foot angle measures tibial rotational variation or torsion, and the normal ranges are 25 degrees of inward to 25 degrees of outward rotation (4). The foot examination documents any foot deformities that may be contributing to the intoeing. Once the profile is filled out, it gives an objective view of the location and magnitude of any rotational variations or torsional deformities. This 2-year-old boy has internal rotational variations of both femurs and tibias. The rotational profile can be used as a baseline while following the child to document that rotational variations are indeed changing with growth.
The rotational profile includes the foot-progression angles, internal rotation of the hips, external rotation of the hips, the thigh-foot angles, and any foot deformities. The angles should be recorded in degrees, and the foot deformities should be described. The example shows that this child has internal femoral and internal tibial variations.
a For foot-progression angle and thigh-foot angle, a positive number indicates inward rotation and a negative number indicates lateral rotation.
FIGURE 4-7. While the patient is walking, the foot-progression angle is the angle between the axis of the foot and an imaginary straight line on the floor representing the direction of movement. The axis of the foot is derived from a line connecting a bisector of the heel with the center of the second metatarsal head. This patient has a foot-progression angle of 20 degrees of internal rotation.
FIGURE 4-8. The internal rotation of the hips can be measured in the supine or prone position. Standing at the foot of the bed, with the patient prone, gravity allows the hips to fall into internal rotation. The angle between the leg and a line perpendicular to the tabletop measures the internal rotation (50 degrees in this patient).
FIGURE 4-9. Standing at the foot of the bed, with the patient prone, gravity allows the hips to fall into external rotation. The angle between the leg and a line perpendicular to the tabletop measures the external rotation (53 degrees in this patient).
FIGURE 4-10. Standing at the foot of the bed, with the patient prone, the thigh-foot angle is the angle between the axis of the thigh and the axis of the foot, with the foot held in neutral position. The axis of the foot is derived from a line connecting a bisector of the heel with the center of the second metatarsal head. The thigh-foot angle measures the amount of tibial torsion (30 degrees in this patient).
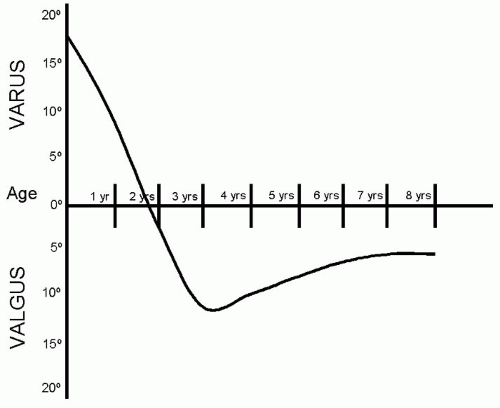
FIGURE 4-11. Graph demonstrating the development of the tibiofemoral angle. Infants have genu varum that typically corrects by 18 to 24 months of age. The lower extremities then gradually develop genu valgum, which peaks between 3 and 4 years of age. The genu valgum then decreases to reach the normal adult tibiofemoral alignment of 7 degrees of valgus by 7 to 8 years of age.
In describing bowlegs and knock knees, the terms “varus” and “valgus” refer to the orientation of the distal fragment (leg) compared with the midline or proximal fragment (thigh). In a child with bowlegs, the distal fragment (tibia) is angulated toward the midline compared with the proximal fragment (femur) and is termed “genu varum.” In a child with knock knees, the tibia is angulated away from the midline compared with the femur and is termed “genu valgum.” In a child with bowlegs, when the ankles are touching, there is a gap between the knees, whereas in a child with knock knees, when the knees are touching there is a gap between the ankles. Most infants are born with bowlegs that spontaneously correct between 12 and 24 months of age. If the bowlegs correct by 2 years of age, it is termed physiologic bowing. The lower extremities then gradually develop genu valgum, which peaks between 3 and 4 years of age, then decreases to reach the normal adult tibiofemoral alignment of 7 degrees of genu valgum by 7 to 8 years of age (Fig. 4-11) (5).
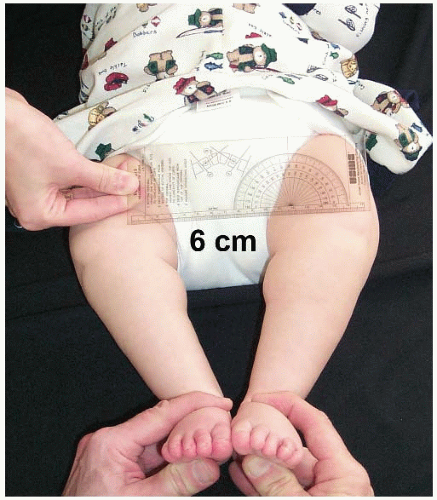
On physical examination, the lower extremities are closely inspected to determine exactly where the deformity is located. If the deformity is mainly located in the proximal tibia, it may indicate tibia vara or Blount disease. If the deformity is symmetric, involving both the distal femur and proximal tibia, it may indicate physiologic bowing (6). The genu varum deformity is documented by measuring the “intercondylar distance.” The intercondylar distance is measured in the supine position with the hips and knee in extension. The feet are brought together until the medial malleoli are just touching, and the intercondylar distance is the distance between the femoral condyles (Fig. 4-12).
FIGURE 4-12. To measure the intercondylar distance, the child is supine with the lower extremities in extension. The feet are brought together until the medial malleoli just touch; the intercondylar distance is the distance between the femoral condyles (6 cm in this patient).
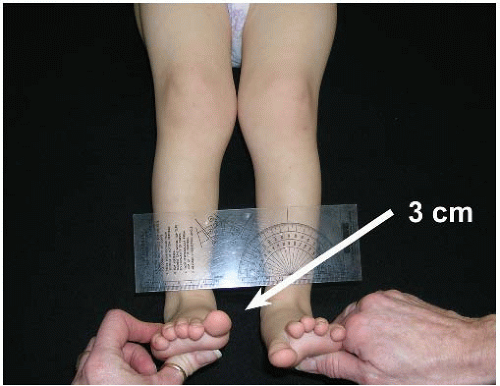
A genu valgum deformity is documented in a similar fashion by measuring the “intermalleolar distance.” With the child in the same position, the feet are brought together until the femoral condyles are just touching, and the intermalleolar distance is the distance between the medial malleoli (Fig. 4-13). This 2-year-old boy likely has physiologic bowing with internal tibial torsion, so the clinician anticipates that the intercondylar distance and thigh-foot angles will decrease over the next 6 months.
A Newborn Boy Is Referred for Evaluation of a Right Foot Deformity. A newborn boy was noted in the neonatal nursery to have a right foot deformity. The birth history reveals that he was the mother’s first child. Routine ultrasound screening at 28 weeks of gestation revealed concern for a possible right clubfoot deformity. The pregnancy was otherwise uncomplicated, and the baby was born by spontaneous vaginal delivery at full term weighing 3500 g (7 lb and 11 oz). The family history reveals that a maternal uncle had multiple foot surgeries performed at a young age.
FIGURE 4-13. To measure the intermalleolar distance, the child is supine with the lower extremities in extension. The feet are brought together until the femoral condyles just touch; the intermalleolar distance is the distance between the medial malleoli (3 cm in this patient).
Foot deformities are commonly seen in newborn infants, with an incidence of approximately 4% (7). The most common foot deformity is metatarsus adductus with talipes equinovarus and vertical talus much less frequently seen. The physical examination of the foot can easily be performed with the baby lying supine of the examination table or on the parents lap if the child is fussy. The upper extremities, neck, spine, hips, and knees are all examined first and determined to be within normal limits. The foot is then visually inspected and found to have multiple deformities as well as abnormal creases. There is only a single heel crease as well as the presence of a deep medial plantar crease.
Palpation and physical examination of the foot reveals the forefoot is adducted (indicating metatarsus adductus), the arch is high (indicating pes cavus), and the hindfoot is rolled into varus and equinus (Fig. 4-14). The tibiotalar, subtalar, and calcaneocuboid joints are gently taken through a full range of motion and reveal decreased movement compared to the other side.
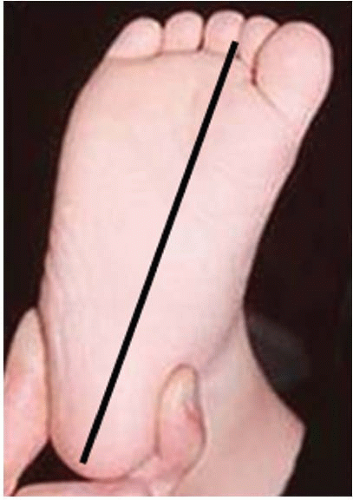
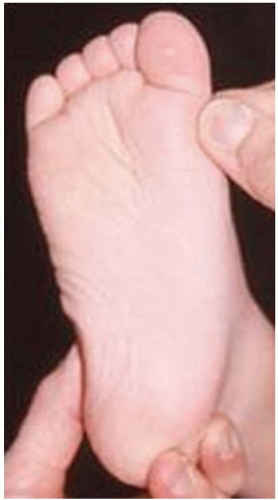
Metatarsus adductus is the most common foot deformity and may be a result of intrauterine positional deformity (Fig. 4-15). Metatarsus adductus has forefoot adductus, but unlike a clubfoot there is no hindfoot equinovarus deformity. It is associated with DDH and torticollis, highlighting the importance of a careful examination of face, neck, and hips (8). The forefoot alignment in relation to the hindfoot can be evaluated by the “heel bisector line” (9). This line is generated by drawing a line down the foot that is center over the calcaneus and parallel to its axis (Fig. 4-16). A normal heel bisector should intersect between the second and the third ray. The metatarsus adductus is mild if the line bisects the third ray, moderate if it bisects the third and fourth rays, or severe if it bisects the fourth or the fifth ray. The lateral border of the foot is inspected and unlike a normal foot that has a straight lateral border, the lateral border is convex or bean shaped indicating metatarsus adductus. A foot that only has metatarsus adductus will have a neutral hindfoot, whereas a clubfoot will have an equinovarus hindfoot deformity. The flexibility of the metatarsus adductus can be assessed by placing the thumb of one hand on the calcaneocuboid joint laterally and grasping the medial forefoot with the other and passively abducting the forefoot (Fig. 4-17). If the metatarsus adductus can be corrected beyond the neutral axis, it is considered flexible. If the metatarsus adductus does not correct beyond the neutral axis, it is considered rigid.
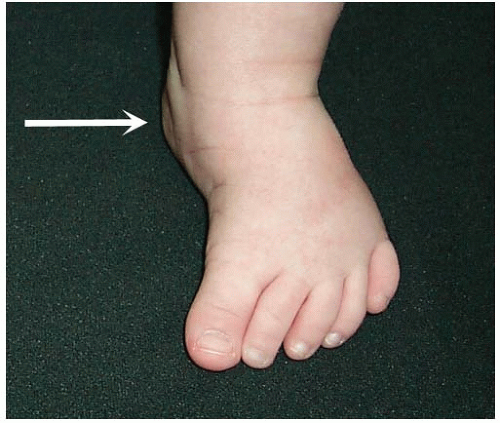
FIGURE 4-14. A clubfoot has forefoot adduction (metatarsus adductus), a high arch (pes cavus), and hindfoot varus and equinus. Depending on the severity of the deformity, a clubfoot may have a posterior and medial skin crease (arrow).
FIGURE 4-15. Metatarsus has forefoot adduction, but unlike a clubfoot the hindfoot is in neutral alignment (arrow).
FIGURE 4-16. The normal heel bisector line intersects between the first and second rays.
Talipes equinovarus or a clubfoot presents as a spectrum of deformity characterized by midfoot cavus, forefoot adductus, and hindfoot varus and equinus (CAVE). Inspection of the skin of a clubfoot reveals varying degrees of posterior and medial skin creases depending on the severity of the deformity (Fig. 4-14). The hindfoot is palpated to evaluate the position of the calcaneus. When the calcaneus is markedly plantarflexed (equinus), the heel pad is displaced and appears absent. This phenomenon is termed an “empty heel pad sign.” In a congenital clubfoot deformity, both the foot and calf are typically smaller than the normal side. In addition, the thigh-foot angles (Fig. 4-10) typically reveal internal tibial torsion and a shortened tibia on the side with the clubfoot (10).
The foot is then examined to assess the rigidity of the deformity by gently attempting to correct the midfoot cavus, forefoot adductus, and hindfoot varus and equinus. The most frequently used classification system to objectively quantify clubfoot rigidity is the Dimeglio clubfoot score (11). A clubfoot can also be classified as typical or atypical. A typical clubfoot is the classic clubfoot that is found most often in otherwise normal infants. An atypical clubfoot is often seen in association with other neuromuscular disorders, such as arthrogryposis and myelomeningocele, and is usually less responsive to non-operative management. The atypical clubfoot can be thin or fat and are frequently stiff, short, and chubby and with a deep crease on the plantar surface of the foot and behind the ankle. They may have shortening of the first metatarsal with hyper-extension of the metatarsophalangeal joint reflecting a plantarflexed first ray.
FIGURE 4-17. The flexibility of the metatarsus adductus can be assessed by placing the thumb of one hand on the calcaneocuboid joint laterally and abducting the forefoot with the other hand. If the metatarsus adductus corrects beyond the neutral axis, it is classified as flexible; if the metatarsus adductus does not correct beyond the neutral axis, it is classified as rigid.
A congenital clubfoot deformity is easily differentiated from congenital vertical talus (CVT) even though hindfoot equinus is prominent in both disorders. As opposed to the clubfoot that is typically seen in otherwise normal children, CVT is often associated with neuromuscular disorders including myelomeningocele, arthrogryposis multiplex congenital, spinal muscular atrophy, and prune-belly syndrome. On examination, in contrast to the clubfoot that has forefoot adductus and hindfoot varus, the CVT foot has forefoot abductus and hindfoot valgus, often described as a “rocker bottom foot.” The talar head is palpable on the plantar surface of the foot and creates the apex of the convex plantar surface (Fig. 4-18). In a CVT, the medial border of the foot is convex or bean shaped, whereas in a clubfoot the lateral border of the foot is convex or bean shaped.
FIGURE 4-18. CVT has forefoot abduction and hindfoot equinovalgus, often described as a “rocker bottom foot.” The talar head is palpable on the plantar surface of the foot (arrow).
This boy has a typical right congenital idiopathic clubfoot deformity. The clinician discusses the natural history of the congenital clubfoot deformity as well as the current treatment and recommends that stretching and treatment should begin preferably within the next few weeks.
An 18-Month-Old Boy Is Referred for Developmental Delay and Inability to Walk. The family first suspected a problem when he was 4 months old and was still having difficulty holding his head up. They became more concerned when he was not sitting at 10 months of age. He finally began sitting independently at 14 months of age and he just recently began pulling to standing, but is not yet cruising are the furniture. He was born after a 28-week gestation, with a birth weight of 1100 g (2 lb 7 oz). He had perinatal respiratory difficulties and was hospitalized in the NICU for 2 months. He developed a seizure disorder at 1 year of age, and his seizures are now under good control with medication.
This patient has developmental delay so the standard physical examination will also include a detailed neurologic examination and developmental assessment. An 18-month-old boy with developmental delay will usually not be apprehensive, and it is convenient to begin the physical examination with the boy in the supine position. The clinician grasps his hands, gradually pulling him into the sitting position, while looking for head and trunk control. A child will usually have head control by 2 to 4 months of age and trunk control by 6 to 8 months of age (Table 4-1). In children, there are a series of primitive reflexes, including the Moro, grasp, neck-righting, symmetric tonic neck, and asymmetric tonic neck reflexes, which are present at birth and then gradually disappear with normal development by 3 to 10 months of age (Table 4-3). If these reflexes persist beyond 10 months of age, it may be a sign of a neuromuscular disorder.
TABLE 4-3 Primitive and Postural Reflexes
Reflex
Age When It Disappears
Primitive reflex
Moro
6 mo
Grasp
3 mo
Neck righting
10 mo
Symmetric tonic neck
6 mo
Asymmetric tonic neck
6 mo
Postural reflex
Foot placement
Early infancy
Parachute
12 mo
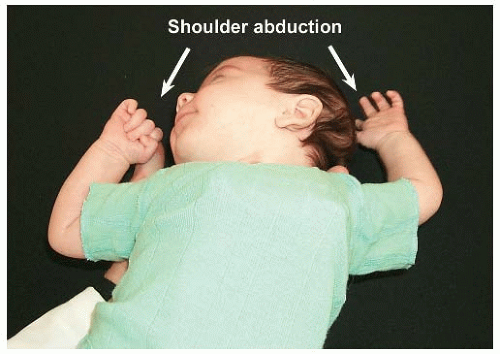
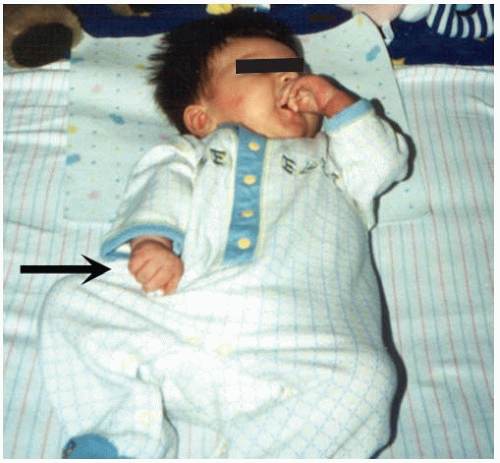
The Moro reflex is elicited by introducing a sudden extension of the neck. The sudden neck extension causes the reflex where the shoulders abduct and the upper limbs extend, with spreading of the fingers, followed by an embrace (Fig. 4-19). The Moro reflex usually disappears by 6 months of age (12). The grasp reflex is elicited by placing a finger in the infant’s palm from the ulnar side. The infant’s fingers will firmly grasp the clinician’s finger. If traction is applied to the hand, the grasp reflex is so strong that the clinician can lift the infant’s shoulder off the table (Fig. 4-20). The grasp reflex usually disappears by 3 months of age. The neck-righting reflex is elicited by turning the head to one side; it is positive if the trunk and limbs spontaneously turn toward the same side. This reflex usually disappears by 10 months of age. The symmetric tonic neck reflex is elicited by flexion of the neck, which causes flexion of the upper limbs and extension of the lower limbs. Similarly, extension of the neck causes extension of the upper limbs and flexion of the lower limbs. The asymmetric tonic neck reflex is elicited by turning the head to the side, which causes extension of the upper and lower extremities on the side toward which the head is turned, and flexion of the upper and lower extremities on the opposite side. This position is termed the “fencing position.” The symmetric and asymmetric tonic neck reflexes usually disappear by 6 months of age.
FIGURE 4-19. The Moro reflex is elicited by gently lifting the infant with the right hand under the upper thoracic spine and the left hand under the head. The left hand is dropped to allow sudden neck extension. The infant abducts the upper limbs, with spreading of the fingers, followed by an embrace.
FIGURE 4-20. The grasp reflex is elicited by placing a finger in the infant’s palm from the ulnar side (arrow). The infant’s fingers will firmly grasp the finger and if traction is applied to the hand, the grasp reflex is stronger.
The extensor thrust, an abnormal reflex, is elicited by holding the infant under the arms and touching the feet to the floor, which causes a rapid extension of all of the joints of the lower limb, progressing from the feet to the trunk. A normal infant will flex rather than extend the joints of the lower extremities when placed in this position. These primitive reflexes need to resolve with growth and development before the child will be able to walk independently.
There are other primitive reflexes that gradually disappear in normal children at different stages of development, including the rooting, startle, Gallant, and Landau reflexes. The rooting reflex is elicited by touching the corner of the mouth, which causes the mouth and tongue to turn toward the side that was stimulated. The startle reflex is elicited by making a loud noise, which causes a mass myoclonic response resembling a Moro reflex, except that the elbows remain flexed. The startle reflex may persist into adulthood. The Gallant reflex is elicited by stroking the side of the trunk, which causes the infant to bend the spine toward the side that was stimulated, creating a scoliosis convex to the opposite side that was stimulated. The Landau reflex is elicited by supporting the infant by the trunk in the horizontal prone position; the typical response is extension of the neck, spine, and extremities. If the infant collapses into an upside-down U, it may indicate hypotonia.
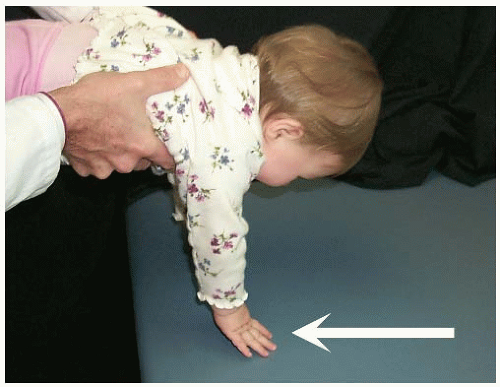
There is another group of reflexes (postural reflexes) that gradually appear with normal development of the nervous system, including the parachute reflex and the foot-placement reaction (Table 4-3). The parachute reflex is elicited by holding the infant in the air in the prone position, then suddenly lowering the infant headfirst toward the table, simulating a fall (Fig. 4-21). The reflex is positive if the infant extends the upper extremities to break the fall. This reflex usually appears by 12 months of age and remains into adulthood. The foot-placement reaction is elicited by holding the infant under the arms, then gently lifting the infant so that the dorsum of the foot or the anterior surface of the tibia touches the side of the table. It is positive if the infant picks up the extremity and steps up onto the table (Figs. 4-22). The foot-placement reaction usually develops early in infancy and may persist until the age of 3 or 4 years.
Bleck (12) evaluated 73 children who were 12 months of age or older and were still not yet walking to determine their prognosis for walking. He used seven tests to predict if an infant would subsequently walk. One point was assigned for each primitive reflex that was still present, and one point was assigned for each postural reflex that was still absent (Table 4-4). A score of two points or more indicated a poor prognosis for walking, a one-point score indicated a guarded prognosis, and a zero-point score indicated a good prognosis.
The physical examination continues by evaluating the spine for any scoliosis or kyphosis. The upper and lower extremities are examined to assess range of motion and to document any contractures. If a contracture is identified, the clinician attempts to passively correct it to determine if it is flexible or rigid. An 18-month-old boy with cerebral palsy and spastic diplegia will typically have contractures that can be passively corrected, whereas a similar child with cerebral palsy and spastic quadriplegia may have already developed rigid contractures. When the clinician gradually attempts to passively correct a rigid contracture, if the contracture has continuous resistance to passive correction, it is termed “leadpipe rigidity.” If the contracture has discontinuous resistance to passive correction, it is termed “cog-wheel rigidity” (12). A patient with cerebral palsy and athetosis may have purposeless type movement patterns, particularly involving the hands and upper extremities. If the athetosis is of the tension type, it can often be “shaken out” of the limb by the clinician. The reflexes are also tested to determine if the patient has hyperreflexia, clonus, and a positive Babinski reflex. This boy has cerebral palsy with spastic diplegia.
FIGURE 4-21. The parachute reflex is elicited by holding the infant in the air in the prone position, then suddenly lowering the infant headfirst toward the table, simulating a fall. The reflex is positive if the infant extends the upper extremities as if to break the fall (arrow).
FIGURE 4-22. The foot-placement reaction is elicited by gently lifting the infant so that the dorsum of the foot or the anterior surface of the tibia touches the side of the table. It is positive if the infant picks up the extremity and steps up onto the table.
TABLE 4-4 Prognosis for Walking
Reflex
Points
Primitive reflex
Asymmetric tonic neck
1
Neck righting
1
Moro
1
Symmetric tonic neck
1
Extensor thrust
1
Postural reflex
Parachute
1 if absent
Foot placement
1 if absent
Prognosis for walking: 2 points, poor; 1 point, guarded (might walk); 0 points, good.
A 3-Month-Old Boy Is Referred for Evaluation Because He Is Not Moving His Right Arm. Shortly after delivering a healthy 5250 g (11 lb 9 oz) baby boy, the mother was told that the baby was not moving his right arm. The pregnancy was normal, but the delivery was difficult because of right shoulder dystocia. The delivery team had to apply considerable traction on the head to deliver the baby. They noted some swelling and tenderness on the right side of the baby’s neck shortly after birth, but this resolved in the first week. At the 2-month appointment with the pediatrician, he was moving his hand but always kept the upper extremity at his side.
After a pediatric orthopaedic history and physical examination, the clinician focuses on a detailed examination of the upper extremities, comparing the paralyzed right side with the uninvolved side. It is important to distinguish between a brachial plexus palsy (a traumatic paralysis involving the upper extremity) and a pseudoparalysis secondary to osteomyelitis of the proximal humerus, septic arthritis of the shoulder, or a birth fracture. The treatment for each of these conditions is different, and a delay in treatment of osteomyelitis or septic arthritis can be devastating. An infant with osteomyelitis, septic arthritis, or a birth fracture will usually have swelling at the site, whereas an infant with traumatic brachial plexus palsy will have no swelling in the extremity, but may have swelling in the neck. An infant with a brachial plexus birth palsy or birth fracture of the humerus will usually have paralysis at birth, whereas an infant with osteomyelitis or septic arthritis may be normal after birth, and then suddenly develop the pseudoparalysis.
Traumatic brachial plexus palsy is a common birth injury, typically seen in primigravida mothers with large babies after difficult deliveries. It occurs because of traction and lateral tilting of the head to deliver the shoulder. If the baby is in the breech presentation, it occurs because of traction and lateral tilting of the trunk and shoulders to deliver the head. Traumatic brachial plexus palsy may have an associated fracture of the clavicle or humerus. There are three types of brachial plexus palsies, depending on which part of the brachial plexus is affected.
The Erb palsy affects the upper roots (C5-C6), the Klumpke palsy affects the lower roots (C8 and T1), and total plexus palsy affects all of the roots in the brachial plexus. The Erb type is the most common and the Klumpke type is rare in newborns. The prognosis for recovery depends on the level and magnitude of the injury and the time at which certain key muscles recover function. If the biceps recovers function before 3 months of age, the prognosis is excellent for a full recovery. The presence of a Horner syndrome usually indicates a poor prognosis (13).
FIGURE 4-23. Paralysis of C5 and C6 causes the shoulder to be held in adduction and internal rotation, with the elbow in extension, the forearm in pronation, and the wrist and fingers in flexion. This posture is termed the waiter’s tip, as if the infant is cleverly asking for a tip (arrow).
On physical examination, an infant with upper brachial plexus palsy is easily recognized by the absence of active motion of the involved extremity in the Moro reflex (Fig. 4-19), or the asymmetric tonic neck reflex. The paralysis of C5 and C6 causes the shoulder to be held in adduction and internal rotation, with the elbow in extension, the forearm in pronation, and the wrist and fingers in flexion. This posture is termed the “waiter’s tip” as if the infant is cleverly asking for a tip (Fig. 4-23). This posture is not seen in an infant with osteomyelitis, septic arthritis, or birth fracture.
An infant with a lower brachial plexus palsy or total brachial plexus palsy is recognized by an absence of the grasp reflex in the involved extremity (Fig. 4-20). The hand is flaccid, with little or no voluntary control. When there is total plexus involvement and the entire extremity is flaccid, the Moro (Fig. 4-19) and grasp (Fig. 4-20) reflexes are both absent. A Horner syndrome refers to the constellation of signs resulting from the interruption of sympathetic innervations to the eye and ocular adnexae. The clinical findings include a triad of ipsilateral blepharoptosis, pupillary miosis, and facial anhidrosis. If the infant has a Horner syndrome, the prognosis for spontaneously recovery is decreased.
This 3-month-old boy is already starting to show biceps motor function at 3 months of age, so the prognosis for recovery is good.
An 18-Month-Old Boy Is Referred Because He Refuses to Walk After His Mother Fell While Carrying Him. The mother states that she was carrying her son on her hip when she twisted her foot and fell going down the stairs. She was fine but her son immediately began crying and refused to walk. When she tried to stand him up, he would not put any weight on his right lower extremity. She believes that when she fell, she may have landed on his right leg. She has not noticed any swelling and he stopped crying after she gave him some anti-inflammatory medication. He is in good health and he has not had any chills or fever. She is a single mother with four other children. She called the pediatrician who evaluated him and recommended a radiograph. The radiograph showed a fractured tibia so he referred them for evaluation and treatment.
A minimally displaced spiral fracture involving the distal tibia in a toddler between 9 months and 3 years of age is termed a “toddler’s fracture.” Although toddler’s fractures are relatively common, it is important to review the details concerning the history, physical examination, and radiographs to rule out nonaccidental trauma or “battered-child syndrome.” Although children have been harmed by their caregivers for centuries, the medical profession did not officially acknowledge the battered-child syndrome until 1962 (14). The age of the boy is important because most child abuse involves children younger than 3 years of age. It has been estimated that 10% of cases of trauma seen in emergency departments in children under 3 years old are nonaccidental (15). Although a number of risk factors have been identified, it is important to remember that children of all socioeconomic statuses, backgrounds, and ages can be victims of abuse.
The clinician spends time in a quiet environment talking with the mother about the details surrounding the injury to determine if the history is consistent with the child’s physical findings. If the history is not consistent with the physical findings, it may cause the clinician to suspect child abuse. While going over the details of the injury, the clinician closely observes the mother’s demeanor to determine if she is being forthright with her answers. If the mother seems nervous or uneasy in describing the circumstances surrounding the accident, it should raise a red flag alerting the clinician that someone may have deliberately harmed the child. After reviewing the details of the mechanism of injury, the clinician reviews the past medical history to determine if this is her son’s first fracture. A history of multiple previous fractures may be consistent with battered-child syndrome or osteogenesis imperfecta. The birth and developmental history are reviewed to determine if there is any underlying disorder that may make this child more susceptible to fracture. The clinician reviews the family history, review of systems, and personal and social history to evaluate for any family issues and to get a better feel for the home environment.
To check that the history is accurate and further evaluate the home environment, the clinician interviews other family members about the injury. It is important to rule out battered-child syndrome because if missed, there is possibility that the child will be injured again, and the next injury could be life threatening. Each year, more than 1 million children in the United States sustain injuries that are inflicted by their caregivers.
In this case, the physical examination includes the whole child, as the clinician is looking for other injuries that may indicate a battered-child syndrome. The height and weight are recorded to determine if there is any evidence of growth retardation or failure to thrive (16). The skin is closely inspected for any contusions, echymoses, abrasions, welts, or burn scars. Skin lesions are the most common presentation of physical abuse and may be the only physical finding. Bruises are common over the shins and knees in 18-month-old boys, but bruises over the buttocks or genitalia should raise a red flag. The head, eyes, ears, nose, and throat are closely examined for bruises or contusions. Head trauma is the most frequent cause of morbidity and mortality in abused children.
After the skin is inspected, the soft tissues and bones of the upper and lower extremities are palpated to evaluate for injuries. An 18-month-old boy should not have any discomfort when the clinician gently squeezes his arms, forearms, thighs, and legs, but will have considerable discomfort if there is a contusion or fracture. After skin lesions, fractures are the second most common presentation of physical abuse. If the clinician believes there is any question about the possibility of battered-child syndrome, it may be beneficial to contact the referring pediatrician to determine if any question of neglect has ever previously been considered. If the story is straightforward and the mother is forthcoming, treatment of the tibia fracture can proceed without any further studies.
A 4-Year-Old Boy Is Referred Because He Began Limping Yesterday and When He Awoke This Morning, He Refused to Walk on His Right Lower Extremity. He was apparently in good health until yesterday afternoon, when his mother noticed that he seemed to be limping on the right side at the grocery store. Later that evening, his limp became more obvious and he complained of pain in his right knee. This morning he awoke complaining of right knee pain and refused to walk. They called their pediatrician who evaluated him and referred him for a possible infection in the right knee. The past history reveals that 2 weeks ago he had a fever and cough that lasted for 5 days.
The clinician understands that although the history is typical for a patient with transient synovitis of the hip, it may also be consistent with septic arthritis, osteomyelitis, or Legg-Calvé-Perthes disease. A 4-year-old boy will often describe exactly where it hurts and may point to the groin, thigh, or the knee. It is important to remember that pain can be referred, and a hip problem presenting as knee pain is a classic example of referred pain. The clinician asks if the pain is constant or intermittent as children with infections tend to have constant pain. The fever and cough 2 weeks ago is an important part of the history, as an upper respiratory infection is often a precursor of transient synovitis of the hip.
Only gold members can continue reading. Log In or Register to continue