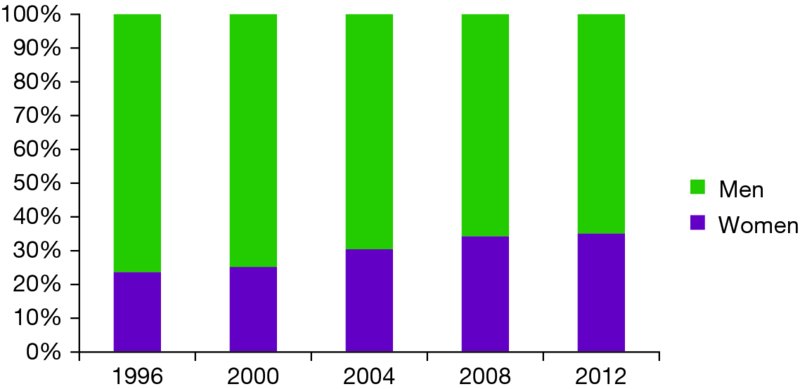
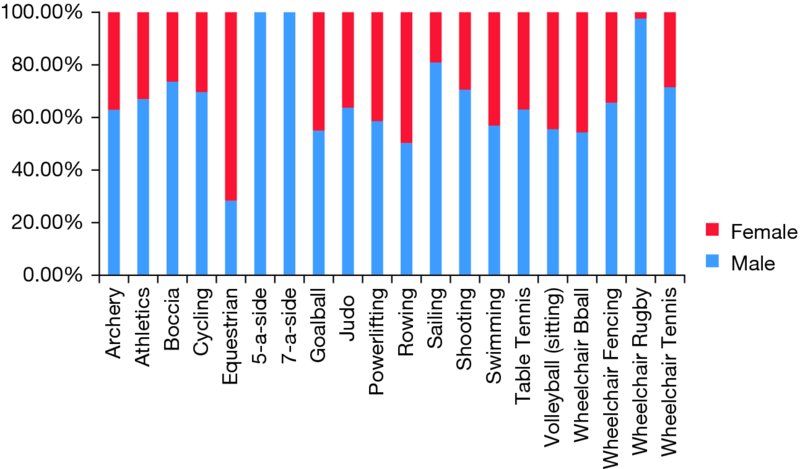
Chapter 13 Cheri A. Blauwet Department of Physical Medicine and Rehabilitation, Spaulding Rehabilitation Hospital/Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA Since the inception of the Paralympic Movement, the unique needs of female Paralympic athletes have remained a growing area of focus and attention. The Paralympic Movement is said to have originated in Stoke Mandeville, England in 1948. At that time, a total of 16 athletes (14 men, 2 women) competed in the sport of archery, with a predominant focus on the use of sport as a proactive tool for rehabilitation and physical fitness. The first modern Paralympic Games took place in 1960 in Rome, Italy, at which time Paralympic athletes competed in the same city, utilizing the same venues as their Olympic counterparts. With the growth of the Games and an expansion in the number of sports included on the Paralympic schedule, increasing numbers of female athletes have become involved in Paralympic sports (Figure 13.1). Concurrently, there has been a progressive shift of the Games from a tool for medical rehabilitation to the elite, competitive sporting event it is today. At the most recent London 2012 Paralympic Games, 1501 female athletes competed, representing 35% of the total athlete count and a 10% proportional increase from the Sydney 2000 Paralympic Games only 12 years prior (Figure 13.1). Currently, 18 of the total 20 sports on the summer Paralympic schedule include female competitors (Figure 13.2). Additionally, via Paralympic sport, women with varied categories of impairment are offered the opportunity to compete on the world’s stage. These include women with spinal cord injury (SCI), spina bifida, cerebral palsy, achondroplasia, visual impairment, and limb loss, among others. Ongoing advocacy initiatives remain focused on expanding these opportunities and increasing the representation of female Paralympic athletes globally. Figure 13.1 Gender participation by proportion at the summer paralympic games, 1996–2012 (Courtesy of the International Paralympic Committee). Figure 13.2 Gender participation by sport at the London 2012 Paralympic Games (note: athletics is the international nomenclature for track and field) (Courtesy of the International Paralympic Committee). As the role of women in Paralympic sport grows, the unique health needs of female athletes with disabilities have come to the forefront as an area of study and professional focus for sports medicine practitioners. The vast majority of the health and medical needs of women with disabilities remain similar to their able-bodied counterparts. In this way, team physicians, athletic trainers, and allied health professionals are qualified to provide medical care to athletes with a disability, whether in a one-on-one clinical setting or via team or mass participation event coverage. Issues of sports-related injury and illness, bone health, genitourinary function, and autonomic control do in fact vary for female athletes with a disability. For these topics, this chapter will provide an overview as to the needs of this specific population. Additionally, the sociopolitical context of female athlete participation in Paralympic sport will be briefly discussed. In Paralympic sport, the incidence and characteristics of both injury and illness are disability and sport specific. An increased awareness of the quantity and type of injuries that athletes may incur while in major international competition enables team medical staff to more adequately prepare for event coverage and anticipate the needs of female Paralympic athletes. In 2002, the Paralympic Injury Surveillance Study (ISS) was initiated at the winter Paralympic Games in Salt Lake City as a means of providing longitudinal tracking of injuries as well as for monitoring injury prevention strategies. Following successful implementation of the Paralympic ISS during the 2002, 2006, and 2010 Winter Games, the project was expanded at the London 2012 Summer Games to include tracking of both sports-related injuries and also medical illnesses. With few exceptions, the incidence of injury and medical illness in Paralympic sport are similar when comparing male and female athletes. For example, at the Vancouver 2010 Winter Paralympic Games, 33 injuries were recorded among 124 female athletes (incidence proportion = 26.6%), while 87 injuries were recorded among 381 male athletes (incidence proportion = 22.8%) (Webborn et al., 2012). There was no significant difference in the incidence proportion (IP) of injury based on sex. For those sports in which female athletes competed, alpine skiing showed the highest IP of injury at 21.6%, although it remains unknown if this varied for male versus female athletes. Data regarding injury and medical illness in summer Paralympic sport reveals similar trends when comparing male and female athletes. With expansion of the Paralympic Injury and Illness Surveillance Study to the London 2012 Summer Paralympic Games, athlete exposure data was also collected, thus allowing for the calculation of incidence rate (IR) of injury, defined as injuries per 1000 athlete days. Overall, this revealed 196 injuries in 1218 female athletes, yielding an IR of 11.5 injuries per 1000 athlete days (95% CI 9.9–13.2) (Willick et al., 2013). Similarly, 437 injuries in 2347 male athletes were recorded, yielding an IR of 13.3 injuries per 1000 athlete days (95% CI 12.1–14.6). For the total Games period, there was no significant difference in the IR of injury in female versus male athletes. Of note, female athletes did experience a higher IR of injury in the precompetition period (IR = 16.7, 95% CI 12.8–21.4) when compared to the competition period (IR = 10.1, 95% CI 8.4–11.9). This may be due to poor health care access for many female Paralympains in their home nations, thus leading athletes to seek care for both acute and chronic injuries upon first arrival to the Games and prior to the start of competition. Overall, for both male and female Paralympic athletes, the shoulder was the most commonly injured anatomical region, representing 17.7% of all injuries over the total study period. Given these findings, it can be extrapolated that medical professionals covering major Paralympic events (assuming a team size of 100 athletes over a 10-day period) should expect to see approximately 11–12 injuries in female athletes, with a predominance of upper extremity involvement. Regarding rates of medical illness at the summer 2012 Paralympic Games, overall 251 illnesses in 1218 female athletes were recorded, yielding an IR of 14.4 (95% CI 12.6–16.3) (Schwellnus et al., 2013). In comparison, 2347 male athletes experienced 424 illnesses yielding an IR of 12.5 (95% CI 11.4–13.8). There was no significant difference between male and female athletes with respect to the IR of illness. For female athletes, the sports of athletics (track and field), archery, and equestrian revealed the highest incidence rate of illness. In these sports as well as several others, greater than 20% of female athletes experienced illness during the Summer Paralympic Games. Illnesses most commonly involved the respiratory system followed by the skin and subcutaneous tissue. Overall, these findings can be extrapolated to conclude that medical professionals covering major Paralympic events (again, assuming a team size of 100 athletes over a 10-day period) should plan to see approximately 14–15 medical illnesses in female athletes, with a predominance of these involving the respiratory system (Figure 13.3). Figure 13.3 Female summer Paralympic athletes show high incidence rates of illness in the sports of athletics, archery, and equestrian (Photo courtesy of Mr Herman Verwey). Issues of bone health remain of utmost importance for injury prevention strategies and to optimize sports performance. For nonambulatory female Paralympic athletes, the effects of decreased bone mineral density due to a low weight-bearing status may be compounded by the more commonly observed age-related changes and/or the female athlete triad. For these athletes, attention must be given to the optimization of bone health and the prevention of fracture during sports competition. Female athletes with a disability may experience a decrease in weight bearing status via several distinct mechanisms. For some athletes this may occur acutely, as in the case of adult onset neurologic disability such as SCI. In these athletes, a rapid decrease in trabecular bone mineral content below the level of neurologic injury may occur at a rate of up to 4% per month post injury, with an estimated 40% reduction in bone mineral density by several years post injury (Dauty et al., 2000). Additionally, trabecular bone loss in postmenopausal women with complete SCI may be greater than in ambulatory postmenopausal women (Slade et al., 2005). For female athletes with a disability that has been present from a young age such as cerebral palsy, bone health may depend on the degree of weight bearing longitudinally over time. Although the relative decrease in bone mineral content for these athletes is less dramatic than in those with a new onset acute neurologic injury, overall bone mineral density is frequently reduced when compared to their age-matched peers. In cases of acute sports-related trauma in nonambulatory female athletes, sports medicine professionals must maintain a high index of suspicion for fracture. For example, in females with SCI, the most common sites for lower extremity fracture include the distal femur and proximal tibia (Vestergaard et al.
The paralympic female athlete
Introduction and background
Injury and illness prevention

Bone health
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel






Full access? Get Clinical Tree


