Surgical Excision of Intradural Spinal Tumors
Gerald E. Rodts Jr.
Daniel Refai
PATHOGENESIS
Intradural tumors are rarely the result of metastatic spread of malignant cells. The main categories of intradural tumors are intradural extramedullary and intradural intramedullary. Some tumors will exhibit characteristics of both intramedullary and extramedullary or exophytic growth.
Intradural tumors of the spine are less common than primary or metastatic tumors of the bone or epidural space. Their surgical removal requires delicate technique and maximal avoidance of injury to the spinal cord and nerve roots.
The most common types of tumor that are found in the intradural extramedullary space are benign meningioma, schwannoma, and neurofibroma.
Teratoma is a more rare intradural tumor that often is both intramedullary and extramedullary.
The most common intramedullary tumors are spinal cord ependymoma, hemangioblastoma, lipoma, astrocytoma, and glioblastoma. They are rarely exophytic except for ependymomas that occur at the conus medullaris.
Nerve sheath tumors (schwannoma, neurofibroma) usually present with radicular symptoms, and myelopathic symptoms develop once the tumor has enlarged to the point where it is causing compression of the spinal cord.
In the lumbar spine (below the conus medullaris), intradural extramedullary tumors commonly cause radicular symptoms (pain, paresthesias, weakness), and low back pain can develop and rapidly progress to an excruciating level when the tumors grow to occupy the majority of the spinal canal.
Intradural intramedullary tumors can cause axial or radicular pain, but the most common presentation is myelopathy. The progression is typically very slow over many months, unless the pathology is the malignant glioblastoma of the spinal cord. A careful preoperative evaluation must eliminate other pathology of the spinal cord parenchyma such as sarcoidosis, transverse myelitis, multiple sclerosis, etc.
PATIENT HISTORY AND PHYSICAL FINDINGS
Presenting symptoms of both intramedullary and extramedullary spinal cord tumors include axial or appendicular/radicular pain. The pain is usually persistent when either active or at rest.
Myelopathic symptoms present as numbness, tingling (paresthesias), gait instability, small motor/hand incoordination (cervical), increasing urinary voiding frequency, difficulty voiding, and general motor weakness.
Upper motor neuron signs such as hyperreflexia, Hoffman sign, spreading of reflexes, myoclonus, and Babinski signs are typical.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Magnetic resonance imaging (MRI) is the imaging technology of choice for intramedullary and extramedullary spinal cord tumors. Contrast enhancement is necessary.
Intramedullary tumors have fairly characteristic appearances on MRI.
Astrocytomas will demonstrate variable contrast enhancement and almost never have a solid, homogenous area of enhancement.
Ependymomas consistently have a homogenously enhancing mass within the parenchyma of the spinal cord (FIG 1A).
T1-weighted images will show low intensity within the tumor mass that enhances brightly on contrast administration.
Often, T2-weighted images will demonstrate surrounding edema within the spinal cord.
Hemangioblastomas typically have a cystic area of low signal intensity on T1-weighted images with a smaller contrast-enhancing nodule on the inside wall of the cyst.
Intramedullary lipomas will be nonenhancing and exhibit the typical high signal on T1- and T2-weighted images as seen in bodily adipose tissue.
Extramedullary tumors such as meningiomas will usually enhance positively with contrast in a very homogenous pattern, and often, a “tail” of enhancement will be seen in the location of attachment to the dura (FIG 1B,C).
Schwannomas and neurofibromas can have homogeneous or heterogeneous enhancement patterns. Some schwannomas will exhibit little to no enhancement, but this is less common.
For patients that cannot undergo an MRI (eg, those with pacemakers, defibrillators, spinal cord stimulators), computed tomography (CT) myelography can be used and can delineate an area of spinal cord swelling or even myelographic block that would indicate the location of intramedullary tumors. Extramedullary tumors are usually well outlined by CT myelography.
NONOPERATIVE MANAGEMENT
Asymptomatic patients with minimal or no upper motor neuron signs can be watched closely with serial neurologic and MRI examination.
Patients with lumbar intradural tumors that are asymptomatic can similarly be watched carefully, but one needs to make sure that even subtle signs of lower motor neuron bladder dysfunction are in fact not present.
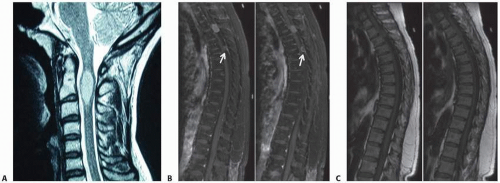 FIG 1 • A. Ependymoma on contrast-enhanced MRI. B,C. T1-weighted MRIs with and without contrast, respectively. Intradural extramedullary meningioma enhanced with contrast. Note dural tail sign (arrows in B). |
SURGICAL MANAGEMENT
Intradural Extramedullary Tumors
The indications to proceed with surgical resection of intradural tumors of the spine include severe, progressive axial or radicular pain; progressive weakness due to nerve root compression or involvement; and myelopathic symptoms of an upper motor neuron bladder, spastic gait disturbance, incoordination of the upper extremities, generalized weakness, and sensory loss or disturbance.
Preoperative Planning
Surgery for intradural extramedullary tumors is usually done via a posterior approach. Preoperative intravenous antibiotics with good central nervous system (CNS) penetration such as Nafcillin or Ancef are administered within 1 hour of the skin incision.
Positioning
Patients with tumors located between the skull base and the upper thoracic spine (approximately T4-T5) are positioned on chest rolls with the head in the table-mounted, three-pin headholder.
A slightly flexed position is used for most cervical tumors.
If posterior fusion with instrumentation is planned, a more neutral sagittal position is preferred. A urethral catheter is placed in most cases.
Intradural Intramedullary Spinal Cord Tumors
Preoperative Planning
The most common tumor type encountered within the parenchyma of the spinal cord is ependymoma, astrocytoma, hemangioblastoma, and lipoma.
The presenting symptoms of intramedullary tumors are less radicular and mostly myelopathic.
Deep axial or radicular pain is uncommon. Numbness, spasticity, disturbance of bladder function, and quadriparesis are most commonly the presenting symptoms.
Needle biopsy is not recommended due to the risk of spinal cord injury and hemorrhage. Therefore, open biopsy and resection is the standard practice for primary intramedullary tumors.
Patients should be counseled extensively regarding the much higher risk and expectation of new postoperative deficits compared with extramedullary tumors.
Almost all patients will experience some degree of new or increased sensory or motor disturbance as a result of removal of an intramedullary spinal cord tumor.
In the early postoperative state, it is difficult to ascertain what new deficits will be transient and which changes may be permanent. Most patients, however, experience improvement of new neurologic findings over time. Some patients will have new permanent deficits, and in some patients, there will be progressive neurologic deficits as seen in patients with a malignant, incompletely resected astrocytoma of the spinal cord. Often, these tumors respond poorly to radiation therapy and chemotherapy.Related posts:
 Occipitocervical and C1-C2 Fusion with Instrumentation
Transforaminal and Posterior Lumbar Interbody Fusion
Costotransversectomy for Canal Decompression and Anterior Column Reconstruction via a Posterior Approach
Revision Lumbar Surgery
Anterior Interbody Arthrodesis with Instrumentation for Scoliosis
Posterior Cervical Approach
Occipitocervical and C1-C2 Fusion with Instrumentation
Transforaminal and Posterior Lumbar Interbody Fusion
Costotransversectomy for Canal Decompression and Anterior Column Reconstruction via a Posterior Approach
Revision Lumbar Surgery
Anterior Interbody Arthrodesis with Instrumentation for Scoliosis
Posterior Cervical Approach

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


