Chapter 6 Surgical Approaches to the Elbow
General principles
The application to the elbow of general surgical principles is probably more important than when these principles are applied to any other anatomical site.1,2 The following should be carefully considered when elbow surgery is undertaken:
Clinical Pearl 6.1
Anticipate common patterns of injury when preparing and deciding on the surgical approach.
Exposure is an important part of the procedure but reconstruction and repair are as critical.
Use full-thickness flaps when exposing the elbow.
Always maintain anatomical orientation during the procedure to decrease neurovascular complications.
Lateral approaches
Several intermuscular intervals have been described. Kocher’s approach utilizes the interval between the anconeus and the extensor carpi ulnaris and can be extended proximally and distally.3 Kaplan described an approach in the interval between the extensor digitorum communis and the extensor carpi radialis brevis and longus.4
Kocher approach
Technique
Either a posterior skin incision with dissection of a full-thickness lateral fasciocutaneous flap or a limited distal lateral skin incision may be used. The anconeus and extensor carpi ulnaris muscles are identified by palpation. A thin strip of fat can almost always be observed in the interval between these muscles (Fig. 6.1). The muscle fibres of the anconeus and the extensor carpi ulnaris muscles tend to blend together towards the insertion, so it is easier to develop the interval in its distal part and then progress proximally. The deep fascia is then opened and the interval is developed by dissecting the anconeus posteriorly. The lateral elbow capsule with the annular ligament is identified and incised longitudinally anterior to the lateral ulnar collateral ligament.

Modifications
For reconstruction of the lateral ulnar collateral ligament, this approach can be extended proximally above the lateral epicondyle by developing the interval between the triceps and the brachioradialis (Fig. 6.2A). Once this is done, the rest of the extensor mass can be sharply incised from the epicondyle, respecting the insertion of the lateral ulnar collateral ligament. In order to achieve adequate exposure of the crista supinatoris, the anconeus along with the lateral aspect of the triceps tendon are reflected posteriorly (Fig. 6.2B).5
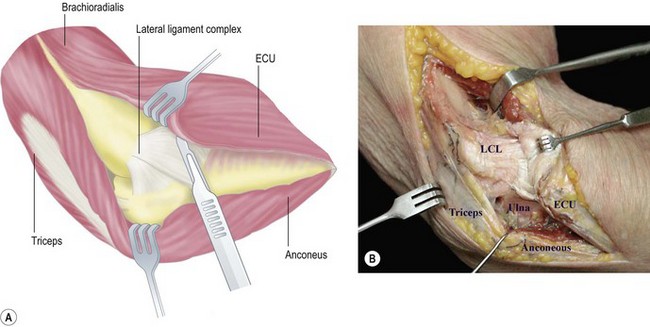
Reproduced with permission of Sales JM, Llusá M, Forcada P, et al. Orozco. Atlas de osteosíntesis. 2nd edn. Fracturas de los huesos largos. Vías de acceso quirúrgico. Barcelona: Elsevier-Masson; 2009.24
Mansat and Morrey described the use of a limited proximal lateral approach for capsular release for stiff elbows, which they termed the ‘column procedure’.6 This exposure may be a proximal extension of the Kocher approach or a focused isolated proximal approach. The exposure is based on a dissection made anteriorly to the lateral border of the distal humerus, elevating the distal aspect of the brachioradialis and the extensor carpi radialis longus from the humerus and entering the interval between the brachialis and the capsule. Access to the posterior capsule involves elevation of the triceps to form the posterior part of the humerus.
Kaplan approach
Technique
A skin incision is made on the lateral aspect of the elbow from the epicondyle extending distally 4 cm towards the ulnar styloid process. The interval between the extensor digitorum communis and the extensor carpi radialis brevis and longus is developed exposing the underlying capsule which is incised longitudinally to gain access to the radial head (Fig. 6.3).
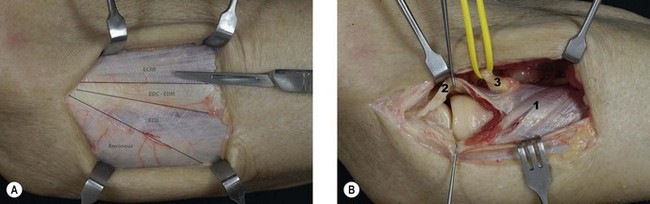
The radial nerve is at particular risk during this approach but this can be reduced by pronation of the forearm, which moves the nerve away from the operative field.7
Kocher posterolateral extensile triceps sparing approach
Technique
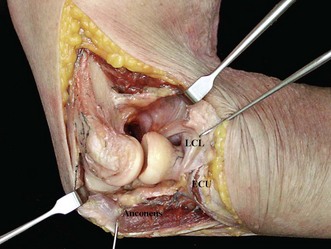
This exposure is an extension of the limited exposures described earlier and involves the release of the collateral ligaments and capsule. A midline posterior skin incision is used. The triceps is elevated from the posterior aspect of the humerus, and dissected anteriorly from the brachioradialis and the extensor carpi radialis longus. The Kocher interval is identified and developed to expose the joint capsule. The anconeus is elevated from the ulna and the triceps attachment to the lateral epicondyle is also reflected posteriorly, leaving its insertion to the olecranon intact. The lateral collateral ligament is then released from the humeral origin, allowing dislocation of the elbow joint by applying a varus stress (Fig. 6.4).
Modifications
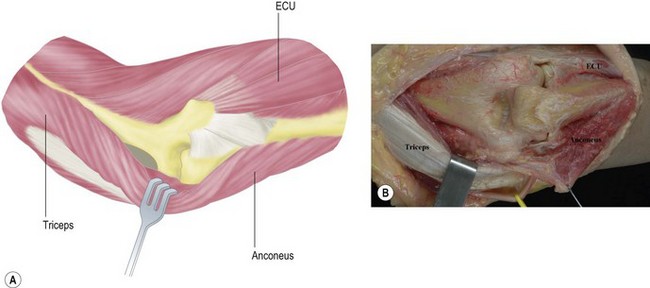
This approach was modified in the Mayo Clinic to include complete release of the triceps from the olecranon, reflecting the triceps mechanism and anconeus from lateral to medial. The triceps and anconeus sleeve is reflected from the tip of the olecranon by releasing Sharpey’s fibres (Fig. 6.5).2
Medial approach
Medial approaches to the elbow are less frequently used than lateral approaches to the joint. They may be indicated to address pathology of the ulnar nerve, injuries of the medial collateral ligament, fractures of the coronoid process and contracture release. Recently, less invasive approaches through the pronator teres have been described for medial joint surgery, including medial ligament reconstruction and other procedures that affect medial structures.8
Extensile medial approach (Hotchkiss)9
Technique
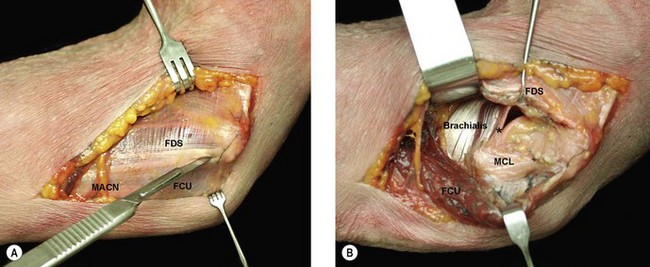
The subcutaneous dissection must be performed cautiously to avoid injury to the medial antebrachial cutaneous nerve. This nerve can be localized running on top of the superficial fascia (Fig. 6.6A). The ulnar nerve should be identified proximally and mobilized. The medial intermuscular septum should then be released for a distance of about 5 cm. An incision is made on the supracondylar ridge 5 cm proximal to the medial epicondyle and continued distally towards the pronator and a portion of the common flexor tendon. A portion of the flexor carpi ulnaris tendon is left attached to the epicondyle posteriorly as this facilitates closure at the end of the procedure. A Cobb elevator is helpful in elevating the anterior structures from the distal humerus until a wide retractor can be introduced (Fig. 6.6B).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


