Stretching
Angela Vitale
INDICATIONS AND CONTRAINDICATIONS
Tight or shortened muscles are vulnerable to injury, especially when there is demand for repetitive use of a particular muscle as required in sports-related events. Tendinitis, the inflammation of a tendon, is usually the result of overuse. Just as muscles may benefit from lengthening with a safe stretching program, tendons too may benefit from stretching that is needed to combat initial trauma and prevent further inflammatory processes.
Stretching is a term used to describe manual or passive lengthening of soft tissue such as muscle or tendon that has been pathologically shortened. Stretching may be indicated for muscle tightness, adhesions from immobilization, and scar tissue adhesions from mechanical or chemical irritation (1). Stretching is as important to an athlete as strength training. Stretching of a muscle can assist in strengthening, help restore the normal pattern of movement and reduce the pain of musculoskeletal injuries, diminish a muscle spasm, or control muscle length in hypertonicity from a central nervous system (CNS) lesion.
Certain athletic activities, such as dance and gymnastics, require ranges of motion greater than those needed by the average person. Certain sports demand overstretching in order to participate. A ballet dancer that lacks good enough “turnout” may use a physiotherapist to improve this motion, usually through active training, warm-ups, and manual stretching techniques (1).
Although the benefits of stretching generally outweigh the risks, it is still important to remember that there is the potential for injury from “overstretch.” Stretching could be harmful if a joint is unstable or hypermobile during activity. If the structures supporting the joint, that is, the muscles, ligaments, or capsule, have been damaged or compromised, then both therapist and trainer should demonstrate caution i.e. in the treatment of a shoulder dislocation. Stretching is often contraindicated or at least limited for a period of time, for example, during treatment of a Bankart repair of the shoulder or an Achilles tendon rupture.
Signs of injury from overstretch may include edema and inflammation of the involved area. Microtearing of the muscle fibers is possible with overstretch trauma and could result in hemorrhage and decreased ability to produce tension, especially the first few days following injury. In the anterior tibialis muscle of a rabbit, scar tissue developed when a stretch injury was induced in the elastic region of the load-deformation relation, while the resulting damage occurred near the myotendinous junction of this same muscle.
Prolonged joint pain or muscle pain lasting greater than 24 hours may be an indication of overstretching. Stretching is contraindicated at a fracture site that is immobilized and healing. Stretching should be provided with caution for individuals with osteoporosis. And individuals that have a chronic history of anticoagulant drug use or steroid use are also at potential risk of injury, if the stretching is too aggressive.
MUSCLE SPINDLE INFLUENCE
Muscle lengthening is necessary for the physiologic movement we observe and is controlled
by input into the CNS. The muscle spindle, a neuroreceptor within the muscle, stretches when a muscle is overstretched and provides information to the CNS that controls the length of the muscle (2) (Fig. 12.1). There are several muscle spindle receptors in a muscle and the spindle density varies from muscle group to muscle group. Muscle spindles are described as having intrafusal fibers enclosed in connective tissue capsules, which exist within the muscle bulk. The intrafusal fibers are arranged in parallel to the extrafusal fibers. The center of the muscle fibers is nonstriated and has a concentration of nuclei. The nuclei can exist within a central bunch (nuclear bag fibers) or as a central chain (nuclear chain fibers) (2). The ends of the intrafusal fibers are striated and can contract (3). Both ends of the spindle are attached to connective tissue of the muscle and therefore indirectly anchored to the muscle tendons (3).
by input into the CNS. The muscle spindle, a neuroreceptor within the muscle, stretches when a muscle is overstretched and provides information to the CNS that controls the length of the muscle (2) (Fig. 12.1). There are several muscle spindle receptors in a muscle and the spindle density varies from muscle group to muscle group. Muscle spindles are described as having intrafusal fibers enclosed in connective tissue capsules, which exist within the muscle bulk. The intrafusal fibers are arranged in parallel to the extrafusal fibers. The center of the muscle fibers is nonstriated and has a concentration of nuclei. The nuclei can exist within a central bunch (nuclear bag fibers) or as a central chain (nuclear chain fibers) (2). The ends of the intrafusal fibers are striated and can contract (3). Both ends of the spindle are attached to connective tissue of the muscle and therefore indirectly anchored to the muscle tendons (3).
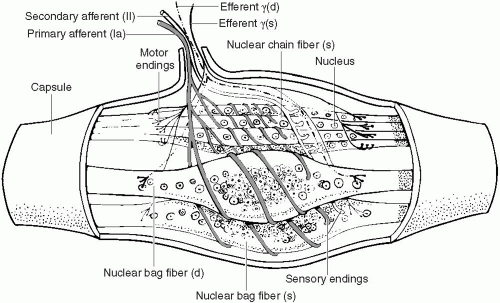 FIGURE 12.1. Anatomy of a muscle spindle, showing the chain fibers and nuclear bag. (From Shumway-Cook A, Woollacott M. Motor control: theory and practical application. Baltimore: Williams & Wilkins, 1995:53.) |
The Ia and II afferent fibers of the muscle spindle both increase their firing rate as the length of the muscle increases. They decrease their firing rate as the length of the muscle decreases. The afferent fibers keep their firing rate constant if the length of the muscle remains constant. In addition to informing the CNS of change in muscle length, the Ia fiber also signals of the velocity with which the muscle lengthening is occurring (2). When a muscle is stretched too much, the muscle spindle is stretched as well. This leads to a contraction of the muscle and the spindle, and less overall stretch. This is the body’s reflexive protection. The Ia afferent neuron of the spindle fibers sends a message that travels via the dorsal horn of the spinal cord. Sensory integration occurs between the neurons of the dorsal horn and the neurons of the anterior horn of the spinal cord. The gamma motor neuron of the anterior horn stimulates motor neuron output in the muscle. This causes an increase in muscle contraction that causes a decrease in muscle stretching (2).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


