Chapter 3 Stress Fractures: Their Causes and Principles of Treatment
Introduction
Physical exercise has beneficial effects on a number of physiologic systems, including the skeleton. However, unwise training practices, combined with potential risk factors, may harm these systems. A stress fracture represents one form of breakdown in the skeletal system.1 It can be defined as a partial or complete fracture of bone that results from the repeated application of a stress lower than that required to fracture the bone in a single loading situation.2
Historical perspective
Stress fractures were first described in 1855 by Briethaupt, a Prussian military physician who observed foot pain and swelling in young military recruits unaccustomed to the rigors of training. He considered it to be an inflammatory reaction in the tendon sheaths resulting from trauma and called the condition Fussgeschwulst. It was not until the advent of radiographs that the signs and symptoms were attributed to fractures in the metatarsals.3 The condition then became known as a “march” fracture because of the close association between marching and the onset of symptoms. Stress fractures were first noticed in civilians in 1921 by Deutschlander,4 who reported six cases in women. However, it was not until 1956, more than a century following their identification in military recruits, that they were recognized in athletes.5
A variety of terms have been used over time to describe stress fractures. These include march fractures, Deutschlander’s fractures. pied forcé, fatigue fractures, or crack fractures.4,6–10 Virtually all of these terms have been intended to describe some etiologic attribute of the stress injuries of bone. In recent years the most commonly used term has been stress fracture.
Following the radiographic description of metatarsal stress fractures, many theories were set forth to explain the etiology of this injury. Most of the reports were based on series that were small, and the theories proposed were concerned with either mechanical factors, such as spasm of the interossei, or flat feet,4,11,12 or with inflammatory reactions, such as nonsuppurative osteomyelitis.7,8
Etiology of stress fractures
It is now recognized that the development of a stress fracture represents the end product of the failure of bone to adapt adequately to the mechanical loads experienced during physical activity. Ground reaction forces and muscular contraction result in bone strain. It is these repetitive strains that are thought to cause a stress fracture. Bone normally responds to strain by increasing the rate of remodeling. In this process, lamellar bone is resorbed by osteoclasts, thereby creating resorption cavities that subsequently are replaced with more dense bone by osteoblasts. Because there is a lag between increased activity of the osteoclasts and osteoblasts, bone is weakened during this time.13,14 If sufficient recovery time is allowed, bone mass eventually increases. However, if loading continues, microdamage may accumulate at the weakened region.14,15 Remodeling is thought to repair normally occurring microdamage.16,17 The processes of microdamage accumulation and bone remodeling, both resulting from bone strain, play an important part in the development of a stress fracture. If microdamage accumulates, repetitive loading continues, and remodeling cannot maintain the integrity of the bone; a stress fracture may result.15,18,19 This may occur because the microdamage is too extensive to be repaired by normal remodeling, because depressed remodeling processes cannot adequately repair normally occurring microdamage, or because of some combination of these factors.18
Epidemiology
Stress fracture injury rate
Stress fracture rates in athletes
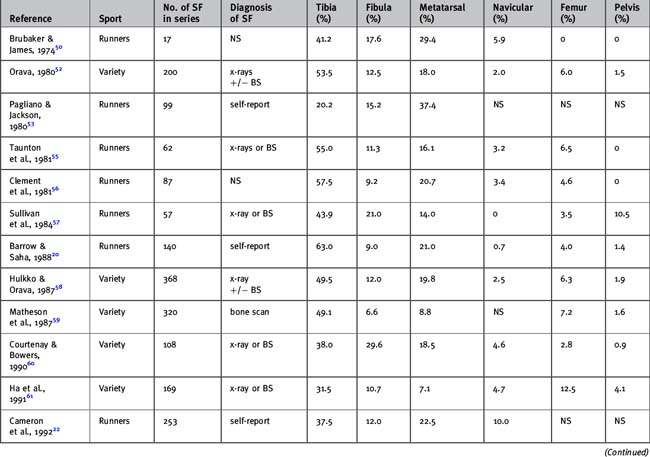
Studies investigating stress fracture rates in athletes are shown in Table 3-1.20–31 Of these, only two allow a direct comparison of annual stress fracture rates in different sporting populations.28,29 Johnson et al.28 conducted a 2-year prospective study to investigate sports-related injuries in collegiate male and female athletes. In total, 34 stress fractures were diagnosed during the study period. Track accounted for 64% of stress fractures in women and 50% of stress fractures in men. The stress fracture incidence rate (expressed as a case rate) in males was highest for track (9.7%), followed by lacrosse (4.3%), crew (2.4%), and American football (1.1%). The stress fracture incidence rate in women was highest for track athletes (31.1%), followed by crew (8.2%), basketball (3.6%), lacrosse (3.1%), and soccer (2.6%). No athlete sustained a stress fracture in fencing, hockey, golf, softball, swimming, or tennis.
Table 3-1 Stress fracture (SF) rates in athletes expressed as participant rates unless otherwise stated
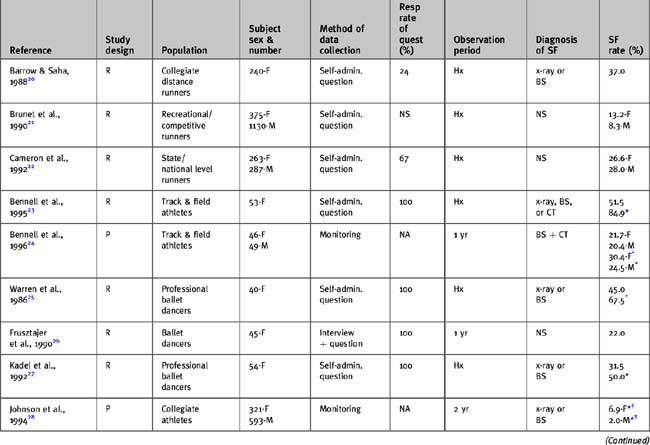
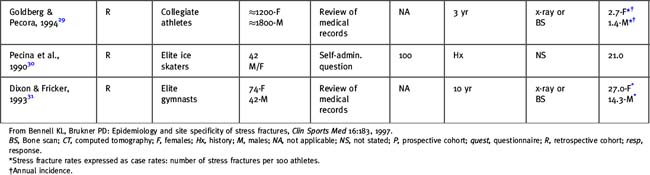
Goldberg and Pecora29 reviewed medical records of stress fractures occurring in collegiate athletes during a 3-year period. Approximate participant numbers were available to allow calculation of estimated incidence case rates in each sport. The greatest incidence occurred in softball (19%), followed by track (11%), basketball (9%), lacrosse (8%), baseball (8%), tennis (8%), and gymnastics (8%). However, participant numbers were small in some of these sports, possibly leading to a bias in incidence rates.
Both studies suggest that track athletes are at one of the highest risks for stress fracture. However, because neither expressed incidence in terms of exposure, it may not be strictly valid to compare the risk of stress fracture in such diverse sports. To our knowledge, there is only one athlete study that has expressed stress fracture incidence rates in terms of exposure.24 This 12-month prospective study followed a cohort of 95 track and field athletes. Results showed an overall rate of 0.70 stress fractures per 1000 training hours. Further research is needed to quantify incidence rates in this manner to allow more valid comparison between studies.
Retrospective studies have measured stress fracture rates in specific sporting populations, mostly runners and ballet dancers.20–23,25–27,29–31 Variation in reported rates reflects differences in methodology, particularly cohort demographics and method of data collection. A history of stress fracture has been reported by 13% to 52% of female runners. The lowest rate was found in one study that included recreational, as well as competitive, runners. Ballet dancers are another population in which stress fracture rates appear high, with 22% to 45% of dancers reporting a history of stress fracture. However, most studies failed to confirm the accuracy of subject recall, a failure that may introduce bias into the figures reported. Nevertheless, it is clear that stress fracture is a relatively common athletic injury.
Stress fracture rates in the military
Reports of the incidence of stress fractures in male recruits undergoing basic training for periods of 8 to 14 weeks are remarkably similar and generally range from 0.9% to 4.7%.32–40 However, in two particular studies involving the Israeli army, the reported incidence was 31%41 and 24%.42 The authors attributed this much higher incidence to several factors, including meticulous follow-up, a high index of suspicion, and the use of the radioisotope bone scan for diagnosis. In addition, asymptomatic areas of uptake on bone scan also were classified as lesions, and this would inflate the reported figures. Stress fracture rates in female military recruits during basic training generally are higher than those in males, ranging from 1.1% to 13.9%.32,33,35,37,39,43
Stress fracture recurrence rates
Clinically it seems that recurrence of stress fractures at new sites is common. In female track and field athletes, half of those who reported a history of stress fracture had experienced a stress fracture on more than one occasion.23 However, few studies have reported recurrence rates in either athletes or the military. When male and female track and field athletes were followed prospectively for 1 year, 60% of those who sustained a stress fracture had a previous stress fracture history.24 The athlete recurrence rate in this study was particularly high at 12.6%. A large number of male military recruits were followed for a minimum of 1 year after basic training.44 The recurrence rate of stress fractures at a different site in those who had sustained a stress fracture during basic training was 10.6%. In the control group of 60 recruits who did not develop a stress fracture during basic training, the incidence of stress fracture after basic training was only 1.7%. This finding could indicate the persistence of risk factors in susceptible individuals.
Comparison of stress fracture rates in different age groups
It is unclear whether age, as an independent factor, influences the risk of stress fracture because results in the military are conflicting and there are no studies in athletes investigating the incidence of stress fractures in different-aged individuals engaged in identical training. In a retrospective cohort study of 20,422 military recruits, review of clinical records found a positive association between increasing age in the range 17 to 34 years and the incidence of stress fractures in both men and women.35 Similar results, even after adjusting for pretraining physical activity, were reported by Gardner et al.36 in a large prospective study. These suggest that increasing age, within the range studied, may be associated with a higher incidence of stress fractures. It is surmised that this may be because bone of older individuals is less resistant to fatigue failure.45,46
However, a prospective study by Milgrom et al.42 in the Israeli army contradicts the hypothesis that stress fracture incidence increases with age in military recruits. For each year of increase in age from 17 to 26 years, the risk for stress fracture at all sites decreased by 28%. The authors suggested that the decreasing risk with age may be related to increased structural maturity, increased bone density, larger cross-sectional moment of inertia, or changes in bone quality in the older recruits. It also is possible that injury-prone older individuals may be less likely to apply for military training. However, it should be noted that the number of recruits older than the age of 19 was very small in this study.
A case series of 1407 patients presenting to a sports medicine center found that stress fractures or periostitis comprised a greater percentage of injuries in the “younger” group (mean age of 30 years), compared with that in the “older” group (mean age of 57 years).47 However, because of the study design, it is not known whether this reflects selection of stress fracture-resistant individuals in the older group, modification of training regimens to lower musculoskeletal stress, or an independent age effect on stress fracture development.
Comparison of stress fracture rates in men and women
It often is suggested that women sustain a disproportionately higher number of stress fractures than men. The relative risk of stress fracture for women compared with men from studies in which stress fracture rates can be directly compared is shown in Table 3-2. In the military, reported incidence rates during an 8-week training period vary from 1.1% to 13.9% in women and from 0.9% to 3.2% in men. These studies consistently show that female recruits have a greater risk of stress fracture than male recruits, with relative risks ranging from 1.2 to 10.32,33,35,37,39,43 This increased risk persists even when training loads gradually are increased to moderate levels and when incidence rates are separated by age and race. The most likely explanation for these findings in the military is lower initial physical fitness in the female recruits. Other possible reasons include differences in bone density and geometry, gait, biomechanical features, body composition, and endocrine factors, particularly estrogen status.
Table 3-2 Relative risk of stress fracture for women compared with men from studies in which stress fracture rates can be directly compared
In contrast, a gender difference in stress fracture rates is not as evident in athletic populations.21,22,24,28,29,31 Studies either show no difference between male and female athletes or a slightly increased risk for women, up to 3.5 times that of men (see Table 3-2). A possible confounding variable is that, unlike the military, in which the amount and intensity of basic training is rigidly controlled, it is difficult to assume equivalence of training between men and women in most of these studies. However, Bennell et al.24 found no significant difference between gender incidence rates even when expressed in terms of exposure. Women sustained 0.86 stress fractures per 1000 training hours, compared with 0.54 in men. It is feasible that a gender difference in stress fracture risk is reduced in athletes because female athletes may be more conditioned to exercise than female recruits; hence the fitness levels of male and female athletes may be closer.
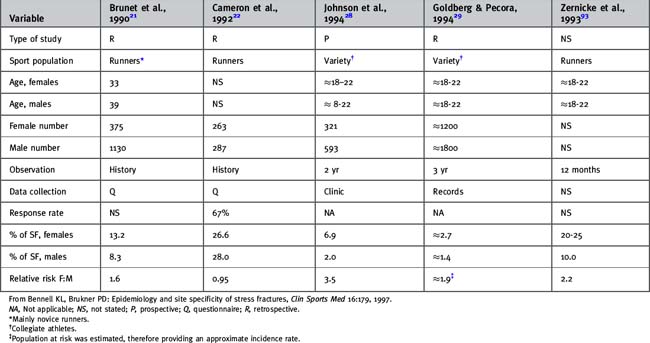
Comparison of stress fracture rates in different races
Both male and female Caucasians appear to be at greater risk for stress fractures than blacks, with relative risks ranging from 2.3 to 24 (Table 3-3). This may be related to higher bone density in blacks48 or to different biomechanical features that may be protective against stress fractures.49
Relative frequency of stress fractures as a proportion of total injuries
Numerous case series have reported that stress fractures comprise between 0.7% and 15.6% of all injuries sustained by athletic populations.31,50–54
In those investigating runners only, the relative frequency is much higher, ranging from 6.0% to 15.6%. In track and field athletes, stress fractures appear to comprise a large proportion of overuse injuries: 34.2% in women and 24.4% in men reported by one study,24 and 42.0% by men and women combined in another.50 In elite gymnasts, stress fractures comprised 18.3% of overuse injuries in women and 9.2% in men.31 It seems that the relative frequency of stress fractures is greater in female than in male athletes. The variation in results probably reflects differences in the composition of each case series.
Stress fracture sites
Athletes
Stress fractures are most common in bones of the lower extremity but also occur in nonweight-bearing bones, including the ribs, upper limb, and pelvis. Numerous studies have reported the anatomic distribution of series of stress fractures20,22,24,27–29,50,52,53,55–63 (Table 3-4). Although there is great variation in the percentage of stress fractures reported at each bony site, the most common sites appear to be the tibia, metatarsals, and fibula. A number of factors may influence the reported distributions of stress fractures. These include type and level of activity, gender, age, and, in particular, method of diagnosis. For example, tarsal navicular stress fractures rarely are evident on radiographs. If diagnosis is confined to radiographs, these therefore will be underreported in comparison with stress fractures at other sites.
Table 3-4 Anatomic distribution of stress fractures (SFs) in athletes expressed as a percentage of the total number of stress fractures in each series
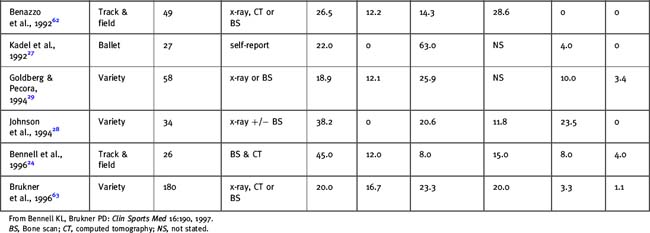
Stress fractures develop at skeletal sites that are subjected to repetitive mechanical loading during a particular activity. The site specificity of stress fractures was illustrated in a prospective study in 95 track and field athletes.24 Although stress fracture incidence rates were similar in power and endurance athletes, the site distribution differed. Power athletes (sprinters, hurdlers, and jumpers) sustained significantly more foot fractures, whereas endurance athletes (middle-distance and distance runners) sustained more long bone and pelvic fractures. In a series of 180 stress fractures, the percentage distribution of sports among the five most common sites is shown in Table 3-5.63 Dancers were the most common group sustaining metatarsal stress fractures, and track and distance runners sustained the most tibial stress fractures, whereas distance runners and dancers were prominent among fibula stress fractures. Track athletes were by far the most common among the navicular stress fractures. Pars fractures were seen in athletes in field events, racquet sports, cricket, dancing, and basketball. It therefore is apparent that different sports show typical patterns of stress fractures; these are summarized in Table 3-6.64 Other sports associated with certain stress fractures are rowing or golf (rib stress fractures), pitching (humeral fractures), and gymnastics (pars fractures).

Table 3-6 Sports and activities commonly associated with different stress fracture sites
Rights were not granted to include this table in electronic media. Please refer to the printed book.
From Brukner PD, Khan KM: Clinical sports medicine, rev ed 2, Sydney, 2002, McGraw-Hill Book Company.
Conditioned athletes may sustain stress fractures different from those in persons unaccustomed to activity. In a series of 368 fractures, competitive athletes had stress fractures in the tibia significantly more often, whereas recreational athletes had significantly more metatarsal and pelvic bone fractures.52,58 It also has been reported that females sustain more metatarsal,52,58 pelvic,52,58 and navicular stress fractures28 than males. Age differences also may play a part; Matheson et al.59 found significantly more femoral and tarsal stress fractures in older athletes and more tibial and fibular stress fractures in younger athletes. However, an interaction between age and site of stress fracture was not confirmed in another large series.58
Military recruits
The location of stress fractures in military personnel has appeared to change over the years, probably as a result of changes in training, with a greater emphasis on running instead of marching; changes in footwear, with athletic shoes often replacing combat boots; and changes in initial fitness levels with fitter recruits. Original reports described primarily injuries of the foot, with most diagnosed stress fractures occurring in the metatarsals.10,65 However, in the last 2 decades, a greater number of stress fractures have been found in the leg, particularly the tibia, thus more closely approximating that observed in athletic populations. In a recent prospective study in 626 male U.S. Marine Corps recruits, 27 stress fractures were sustained.40 The most common site was the tibia (41%), followed by the metatarsals (26%), the femur (19%), and the tarsals (15%). The site distribution of stress fractures in military populations has been well reviewed by Jones et al.43
Risk Factors for Stress Fractures
Genetic predisposition
A large component of the variation in bone mass can be attributed to genetic factors.66 Not surprisingly, then, a family history of osteoporosis is considered to be a risk factor for low bone density and osteoporosis in both men and women.67,68 Similarly, a significant relationship between a family history of osteoporosis and yearly change in bone density has been demonstrated in studies of runners and nonrunners.69 It therefore is feasible that some individuals may be genetically predisposed to stress fractures when exposed to suitable environmental conditions, such as vigorous exercise. This was implied in a case report in which a pair of 18-year-old monozygotic twins undergoing basic military training sustained identical multiple stress fractures in the femoral and tarsal bones.70 The authors proposed that identical environmental conditions served to unmask a genetically determined deficiency in the affected bones. Although Myburgh et al.71 failed to find a difference in the incidence of a family history of osteoporosis in a group of 25 athletes with stress fractures and a group without stress fractures, this may reflect the small sample. At present, there is little evidence to show that genetic factors predispose an athlete to this injury.
Menstrual disturbances
Although progesterone may be a promoter of bone formation, particularly in cortical bone,72 and luteal phase deficiency in athletes is associated with lowered progesterone levels, a possible link between luteal phase deficiency and stress fracture risk has not been sought. Research to date has focused on the relationship between stress fracture incidence and menstrual irregularity (amenorrhea and oligomenorrhea), age of menarche, and use of the oral contraceptive pill (OCP).
The findings of numerous studies suggest that stress fractures are more common in athletes exhibiting menstrual disturbances20,25–27,71,73–78 (Fig. 3-1). Although not all results were statistically significant, power may have been limited by relatively small samples in some studies. In general, athletes with menstrual disturbances had a relative risk for stress fracture that was between two and four times greater than that of their eumenorrheic counterparts. However, in ballet dancers, logistic regression analysis showed that amenorrhea for longer than 6 months’ duration was an independent contributor to the risk of stress fracture, with the estimated risk being 93 times that of a dancer with regular menses.27
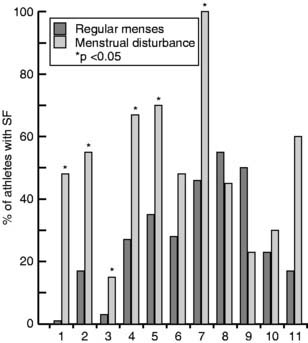
Figure 3-1 Studies in which the percentage of athletes with stress fractures could be compared in groups with and without menstrual disturbances. 1, Lindberg et al., 198473; 2, Marcus et al., 198574; 3, Lloyd et al., 198675; 4, Warren et al., 198625; 5, Nelson et al., 198776; 6, Barrow and Saha, 198820; 7, Myburgh et al., 199071; 8, Frusztajer et al., 199026; 9, Grimston et al., 199177; 10, Cameron et al., 199222; 11, Kadel et al., 1992.27
The risk of multiple stress fractures also seems to be increased in those with menstrual disturbances.20,79 Clark et al.79 found that, although amenorrheic and eumenorrheic groups reported a similar prevalence of single stress fractures, 50% of the amenorrheic runners reported multiple stress fractures, compared with only 9% of those regularly menstruating.
Grimston et al.80 developed a menstrual index that summarized previous and present menstrual status. They found no relationship between this menstrual index and the incidence of stress fractures in 16 female runners. Conversely, Barrow and Saha20 found that lifetime menstrual history did affect the risk of stress fracture. They showed the incidence of stress fracture to be 29% in the regular group and 49% in the very irregular group. The results of a prospective study also demonstrated that those with a lower menstrual index were at greater risk of stress fracture. Myburgh et al.71 found that, although athletes with stress fractures had a higher frequency of current menstrual dysfunction than athletes without stress fractures, there was no difference in past menstrual status. This suggests that changes associated with menstrual dysfunction are reversible and do not affect future stress fracture risk if regular menses return.
In summary, it would appear that there is a higher incidence of menstrual disturbances in female athletes with stress fracture than in those without. These findings have led some authors to assume that this is a direct result of decreased bone mineral density (BMD) in athletes with menstrual disturbances. However, athletes with menstrual disturbances also exhibit other risk factors, such as lower calcium intake,81 greater training load,82 and differences in soft tissue composition.83 Because these were not always controlled for in the studies discussed, it is difficult to ascertain which are the contributory factors.
The relationship between age of menarche and risk of stress fracture is uncertain. Some authors have found that athletes with stress fractures have a later age of menarche,25,84,85 whereas others have found no difference.26,27,71 In a prospective study, age of menarche was an independent risk factor for stress fracture, with the risk increasing by a factor of 4.1 for every additional year of age at menarche.78 However, the mechanism for this relationship is unclear, because a later age of menarche also is associated with an increased likelihood of menstrual disturbance,86 a lower energy intake,87 decreased body fat or weight,87 and excessive premenarcheal training,86 all of which could influence stress fracture risk.
Some authors have claimed that the OCP may protect against stress fracture development. Barrow and Saha20 found that runners using the OCP for at least 1 year had significantly fewer stress fractures (12%) than nonusers (29%). This was supported by the findings of Myburgh et al.71 Although no difference in OCP use was reported in ballet dancers with and without stress fractures,27 few dancers were taking the OCP. Because these studies are cross-sectional or retrospective in nature, it is not known whether the athletes were taking the OCP before or following the stress fracture episode. In addition, athletes may or may not take the OCP for reasons that in themselves could influence stress fracture risk. A prospective study did not support a protective effect of OCP use on stress fracture development.78 Nevertheless, it is not known whether the risk of stress fracture is decreased in athletes with menstrual disturbances who subsequently take the OCP. This is an important area for future research.
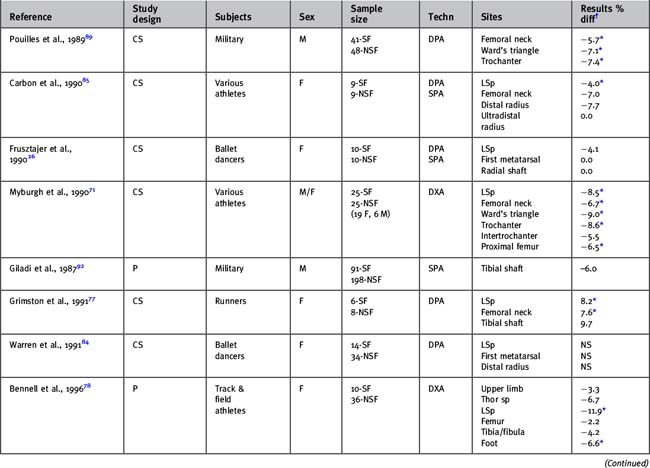
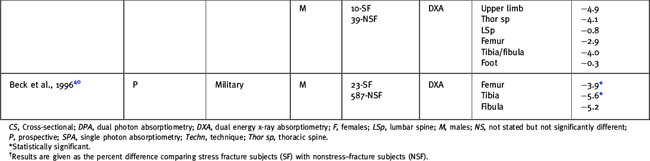
Low bone density
Theoretically, low BMD could contribute to the development of a stress fracture by decreasing the fatigue resistance of bone to loading and by increasing the accumulation of microdamage.45,88 Results from a limited number of studies comparing regional bone density in military or athletic groups with and without stress fracture have been inconclusive26,40,71,77,78,84,85,89,90 (Table 3-7). The discrepancy may reflect differences in populations, type of physical activity, measurement techniques, and bone regions. However, the findings of a 12-month prospective study using dual energy x-ray absorptiometry (DEXA) to measure bone mass indicate that low bone density is a risk factor for stress fractures in women and possibly in men.78 Female athletes who sustained tibial stress fractures had 8.1% lower tibia/fibula BMD than athletes without stress fractures (p < .01). In the men, the tibial stress fracture group had 4.0% less tibia/fibula BMD than the nonstress fracture group, although this was not significant (p = .17). However, it is important to note that in this study the athletes with stress fractures still had bone density levels that were similar to or greater than less-active control subjects. This implies that the level of bone density required by athletes for short-term bone health is greater than that required by the general population.
Bone geometry
Bone geometry influences the ability of the bone to resist mechanical loads. A prospective study of 295 male Israeli military recruits assessed the influence of bone geometry on stress fracture risk.91,92 Significantly fewer stress fractures were sustained by those with a greater mediolateral tibial width, measured using standard radiographs, than by those with a narrower tibia. This may be due to a greater area moment of inertia and hence increased ability of the bone to resist bending forces in the anteroposterior direction. However, the incidence of stress fractures did not correlate with cortical thickness. These findings were confirmed by a recent prospective study of 626 U.S. male recruits.40 Using DEXA to derive structural geometry, the authors found significantly smaller tibial cross-sectional area, smaller tibial section modulus, and smaller tibial width in the stress fracture cases. These remained after adjusting for body weight differences between groups. There are no data that investigate whether bone geometry predisposes to stress fractures in athletes.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


