A Sports participation a priority Even in densely populated areas, providing room for sports is an important community priority (Hong Kong).
Sport participation has positive and some negative aspects. The benefits of sports are well documented and clearly exceed the negative aspects. The downside of athletic participation need to be identified and addressed [B]. In addition, the recently recognized problems of concussions, repetitive head trauma, and the increased risk of degenerative arthritis in late adult life troubling.
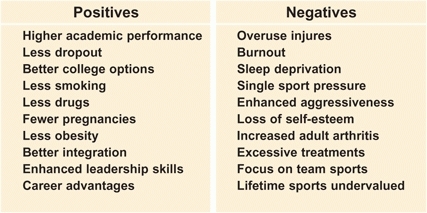
B Participation in sports These tables list the positive and negative aspects of sport participation.
The role of primary care provider is expanding, requiring a need to understand the problems and management of the musculoskeletal system in children.
Advantages of Participation in Sports
Cost-effective
Adding sports adds only about 3% to a school’s budget. Consider sports as just not a diversion, but an important component of education. Sports teaches teamwork, sportsmanship, provides experience with the joy of winning, and coping with losing. It teaches the rewards of hard work, self-discipline, enhances self-confidence, and develop skills in handling competitive situations. These skills learned through sports participation increase the likelihood of success in adult life increasing and becoming a contributing member of society.
Academic
In 1992, a Colorado study showed that sports participation was associated with significantly higher grade-point average, better attendance, a lower dropout rate, and a greater likelihood of going to college.
Social
The demands of sports motivate kids to avoid using drugs, smoking, or becoming pregnant.
Career success
In a 1987 survey of Executives (Vice President level or above) in 75 Fortune 500 companies, 95% had participated in sports during high school. This exceeds the participation in student government (54%), national honor societies (43%), scouting (35%), and school-sponsored publications (18%).
Obesity
Overweight frequency is increasing in most countries, especially in USA [C]. Researchers estimated that if all adolescents played on two or more sport teams per year, the obesity prevalence rate would decrease by about 25%. A New Hampshire/Vermont study found that adolescents who played three sports were 27% less likely to be overweight and 39% less likely to be obese as compared with those not in sport teams. Basically the same findings occurred in children who walked or biked to school.
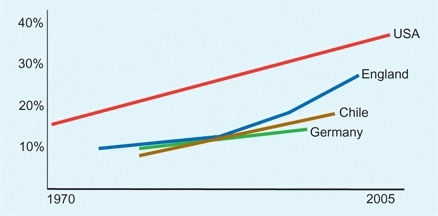
C Overweight children in different countries From Government Office of Science.
Goals
Make sports fun
The child’s sports experience is often diminished by pushy parents, aggressive coaches, and limited options. When the major emphasis is on winning, the chances of a child continuing long-term on the team diminish with time. Most kids eventually get “cut” from the varsity team, most are not lifetime sports. Play is the occupation of the child [A].

A Play, the occupation of the child Play, whether individual or in teams, is a vital part of a child’s life.
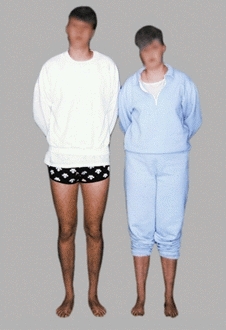
Place for small, not athletic children
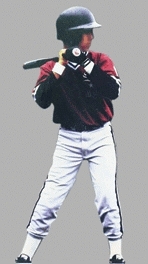
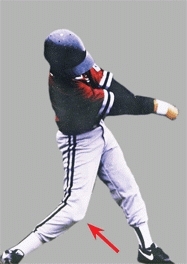
On the downside, the child may be pressured into a sport for which he or she has little ability. The child performs poorly, is embarrassed, and ends up with a damaged self-image. The smaller child often has a disadvantage [B].

B Size differences in same-age children The largest boy is nearly double the weight of the smallest boy in the team (yellow arrows).
Problems
Overuse Injuries
Overuse injuries are increasing and now account for about half of all childhood injuries. They are best prevented. Most resolve with rest. However, some injuries, like osteochondritis cause joint damage with the potential of long-term disability.
Burnout
The child may experience a conflict between the demands of athletics, their social life and education. Too much sports results in excessive pressure, loss of time for sleep, socialization, and school work. This limitation creates some long-term problems that may result in a withdrawal from sports altogether, an excessive focus on electronic games, etc.
Concussion and traumatic brain injury (TBI)
About 50,000 high school American football players are diagnosed with a concussion per year, representing about 5% of the population of high school football players. Once concussed, athletes are about five times more likely to experience a second, rare, but often lethal injury: Second Impact Syndrome (SIS) that results from relatively minor injury.
Chronic traumatic encephalopathy (CTE) is linked to American football and boxing. Its features include memory impairment, depression, aggression, and dementia that occur in mid to late adult life. In these cases, the brain shows degenerative changes with the accumulation of abnormal proteins.
Degenerative arthritis
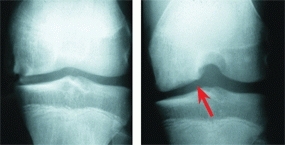
Evidence shows that those who sustain significant joint injuries during adolescence have an increased likelihood of developing degenerative arthritis during adult life [C].


C Effect of meniscectomy during childhood At age 13, this patient sustained a torn medial meniscus while playing football. An arthroscopic meniscectomy was performed. At age 29, the man has disabling pain and significant disability. The radiograph shows severe osteoarthritis (arrows).
Excessive surgery
Some indications for surgery are lowered if the parents are determined to make their child as perfect as possible in preparation for a scholarship and a career as a professional athlete. Examples include open reduction of clavicular fractures, correction of rotational problems in the lower limb, etc.
Injury Statistics
Parents and children are often unaware of the potential of injury from sports. It is useful to educate them with data. Fortunately, most sports injuries are minor and heal rapidly, but some are serious. Injuries (sports-related and not) are the leading cause of childhood death. Significant injuries can cause long-term disability. Most deaths in sports are due to cardiovascular disease or head injuries. Most trauma deaths are the result of high-speed injuries beyond the velocities of childhood sports. Few injuries lead to permanent disability. The most common serious injuries occur in collision sports such as American football [A], which causes ligamentous or meniscal tears in the knee.
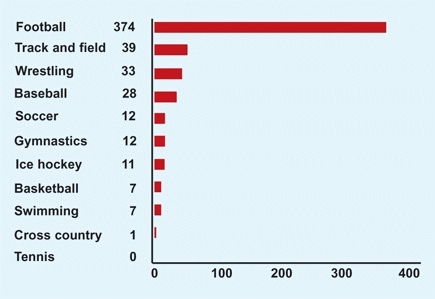
A Fatal and catastrophic injuries in high school sports Based on rates per 100,000 participants. From Cantu and Mueller (1999).
Sport
Injury rates vary considerably among sports [B]. Football and wrestling cause acute injuries, whereas running, throwing, and field events tend to produce overuse problems.
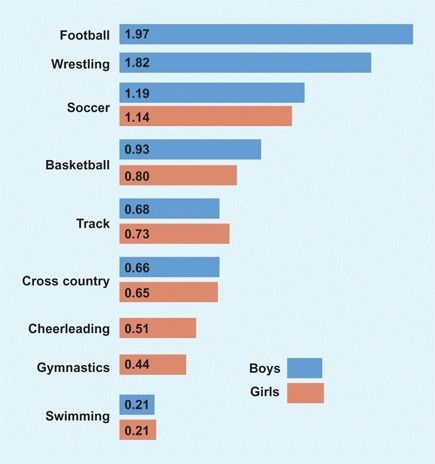
B Injuries in high school athletics per athlete per year in the United States From Beachy et al. (1997).
Age
Injury rates and severity increase with age [C]. The small child simply does not have the speed or mass to cause serious injury. In young children, fractures occur more commonly through bone and less commonly through growth plates, reducing the risk of altering growth.
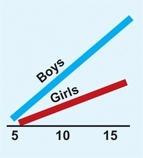
C Injuries by age groups in years From Beachy et al. (1997).
Gender
Boys are injured more frequently than girls [C] because they play the highest risk games, American football and wrestling. When these two sports are removed from the injury profile, overall injury rates between boys and girls are comparable, except for the 2–3 times greater incidence of ACL injuries in girls playing basketball and soccer.
Disability
Disability may occur early from the acute injury or appear later from osteoarthritis due to articular damage.
Short-term disability
from injuries is usually temporary because the majority of injuries are minor [C] and are disabling only during the period required for healing and rehabilitation.
Long-term disability
is most serious and usually due to osteoarthritis in a site that has sustained more than one injury. Twenty years after playing high school football, radiographic changes showed osteoarthritis of the knee [E]. In midadult life, osteoarthritis of the hip severe enough to require total hip replacement is quadrupled in men who had moderate to high exposure to sports [C]. When these men had physically demanding work, their risk increased eightfold above the control group [F]. The majority of college football players who sustained major knee injuries had previously sustained injury to the same knee during high school. Whether modern techniques of meniscal and ACL repair will alter these statistics remains to be determined. However, without such repairs, poor outcomes are inevitable. Studies suggest that injuries from high-impact sports during adolescence are likely to have significant adverse consequences in adult life. These risks should be balanced against the substantial benefits of high school team sports participation.
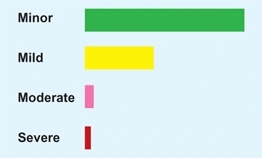
D Injury severity Proportion of injuries by severity. From Beachy et al. (1997).

E Relative percentage with osteoarthritis 20 years after high school football From Moretz (1984).
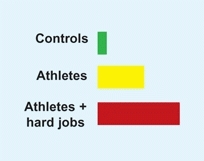
F Relative frequency of total hip replacement by history of activity From Vingard (1993).
Prevention
It is estimated that about half of sports injuries are preventable. Because sports account for about one-third of all childhood injuries, the potential impact on childhood is enormous. Environmental and personal factors are both important.
Environmental Factors
Thermal regulation
is of critical importance in children. Select a cool environment when possible. Avoid excessive clothing and prolonged exposure to sunlight. Insist on adequate fluid intake. Check weight before and after participation to monitor hydration status.
Playing surface
should be as shock absorbing as possible [A]. Avoid running on hard surfaces. Insist on padded surfaces for playgrounds and for field events where falls are common.

A Hard surface This attractive play area for children has a serious flaw: a concrete surface. The children may stay cleaner but are much more likely to sustain injuries with falls.
Motor vehicles
are dangerous in areas of play, especially for sledding and biking.
Encourage adults
to focus more on safety than winning. Emphasize the importance of learning sport skills, the value of team participation, and having an enjoyable experience. Point out that participation sometimes involves losing. Learning to accept and handle losing teaches an important lesson that will be valuable throughout life.
Maintain equipment
in good working condition and be certain the equipment is size appropriate and properly fitted.
Provide medical care
for preparticipation evaluation and early intervention.
Individual Factors
Wear protective devices
Make sure they are appropriate in size and fit. Be sure the children wear protection, such as helmets, face and mouth guards, and body protection in vulnerable sites. Also, they should remove helmets when not involved in a risk of collision.
Proper conditioning
started preseason improves strength, flexibility, and endurance.
Limit rate of increase
in loading or repetitions to about 10% per week (10% rule).
Proper footwear
provides good shock absorption and traction.
Adequate sleep
Those who sleep at least eight hours a night are about 70% less likely to be injured than those who sleep less.
Sporting Environment Control
Preseason medical evaluation
should identify which conditions could be worsened by sports participation and identify musculoskeletal problems that could be improved by rehabilitation before returning to sports.
Provide medical coverage at high-risk events
to provide prompt professional diagnoses and management.
Improved coaching skill
is an important factor. Encourage coaches to avoid coaching by the approach used in their own childhood experience. Help them understand that the primary source of overuse injuries is too much, too soon—not just too much. Coaches should advance progression in sports participation appropriately to avoid placing the young athlete at risk. Too rapid advancement increases risk of injury.
Children with Orthopedic Disabilities
Children with hip dysplasia, clubfeet, and other orthopedic deformities may become outstanding athletes [B]. This is important information to give parents while treating these children.

B Outstanding athlete with childhood orthopedic problem This boy had a clubfoot deformity and became an excellent athlete in many sports.
Elite Athletes
Elite or outstanding athletes can have musculoskeletal problems [C]. It is commonly believed that to become elite athletes, children must start training during their first decade; however, this has not been documented.

C Elite athletes These patients are excellent athletes. The boy (left) had DDH as an infant and underwent a pelvic osteotomy for correction of residual acetabular dysplasia. He is an outstanding soccer player. The brother and sister (right) have contracture of the heel-cords and secondary overuse syndromes but are still outstanding runners.
Studies have demonstrated that the injury rate in elite juvenile athletes is lower than that of average-ability athletes. Elite athletes are stronger and more flexible than their peers. Because many will progress to participate in impact sports in late adolescence and adulthood, they risk long-term disability from osteoarthritis later in life. The risk of osteoarthritis is sport specific, and greater for those participating in collision sports.
Focused juvenile athletes are preoccupied with their sports. This is beneficial in enhancing self-esteem; promotes a healthy lifestyle by discouraging the use of drugs, smoking, and obesity; and possibly provides scholarships or other sport-generated income. On the downside, academic achievement, socialization, interpersonal skills, and other broadening experiences may be limited. The cost to girls may be greater. Menstrual irregularities, possibly shortened stature, and eating disorders may occur. The preoccupation with thinness in gymnasts and dancers creates special problems for girls.
Special Children
Children at both ends of the spectrum of ability have special needs. They are vulnerable to over- or underparticipation. Each has its unique problems. These children are in special need of the Bill of Rights for Young Athletes, as detailed by Sullivan [A].
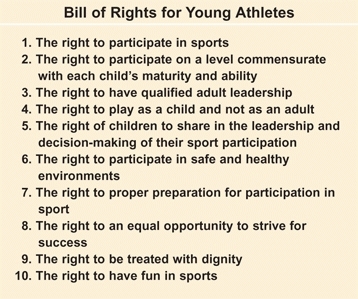
A Bill of rights From The Pediatric Athlete, Sullivan (1988).
Children with Disabilities
Children with disabilities need physical activity as much as or more than other children. An objective of management is the normalization of these children’s lives [B]. This often requires special efforts by the family, sponsoring organizations, and medical providers.
B Limb deficient child This child with a right lower limb amputation is an excellent baseball player. The only sign is the upper rim of the prosthesis visible in unusual positions (arrow).
Skiing programs
are useful for children with limb deficiencies and mild cerebral palsy.
Wheelchair sports,
such as basketball and racing [C], are excellent choices for providing exercise with little risk.

C Wheelchair sports This child has paraplegia and is an outstanding athlete.
Organized sports
participation requires a supportive system by the adults as well as other children to succeed. An integrated play environment is healthy not only for the disabled child but also for the teammates. The teammates gain understanding and are more likely to befriend the child with a disability.
Special summer camps
are effective in providing supervised programs [D] with medical support.

D Swimming This child with arthrogryposis is learning to swim. This can be a lifetime sport.
Horseback riding
programs are popular, but they require close adult supervision to prevent falls. Therapeutic riding associations offer this experience at reduced costs. When done appropriately, this experience is worthwhile.
Family programs
are most important. Encourage the family to include the special child in their normal activities [E]. Unfortunately, families often overprotect the child, limiting the child’s experiences and thereby harming the child. Encourage families to go ahead with the travel and physical activities that they would normally undertake and to include the whole family.

E Playing Selecting play equipment that is stable, rounded, and lightweight increases safety.
Injury Types
Injury types from athletic participation include acute and overuse injuries. Acute injuries are the same as those that occur in nonsporting accidents. Stress injuries result from repetitive microtrauma and are unique to sports medicine. These injuries are the focus in this chapter.
Acute Injuries
Contusions
are common injuries and usually heal quickly and completely. Secondary hematomas are less common in children, presumably due to enhanced hemostatic control in children. Rarely do contusions lead to formation of myositis ossificans. This is most common in the quadriceps. Avoid prolonged immobilization. These lesions mature over time. They may be confused with osteogenic sarcoma.
Ligament injuries
Because ligaments are two to three times stronger than bone in children, avulsion fractures are common during growth. Ligaments tend to fail suddenly, in contrast to physeal injuries, which occur with more slowly applied loads. Ligamentous injuries can be graded [A] as follows:
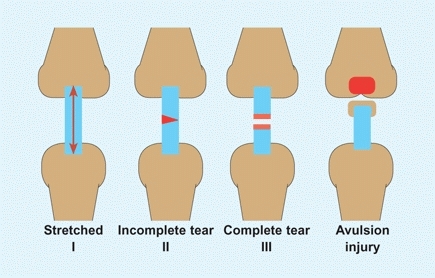
A Grading of ligamentous injury These may be graded into three categories. Avulsion with a bone fragment (right) is common in children and does not fall into the numerical classification.
Grade I
represent stretch injuries without disruption of fibers that cause tenderness and swelling but without detectable instability.
Grade II
are partial tears that allow greater mobility but with a definite endpoint.
Grade III
are complete tears involving greater soft tissue injury, including the joint capsule and leading to joint instability.
Ligament injuries are most common around the ankle and knee and, when associated with capsular disruption, cause joint instability. They may coexist with bony injuries, as seen in tibial spine fractures. When the tibial spine is avulsed, the anterior cruciate ligament is stretched, leading to residual laxity following bony union.
Bone injuries
Acute bony injuries can fall into the same patterns as those occurring from accidental trauma in nonathletic situations (they are covered in Chapter 4).
Musculotendon injuries
can occur at many sites [B]. Complete separations are rare, and healing usually occurs spontaneously because no discontinuity occurs.
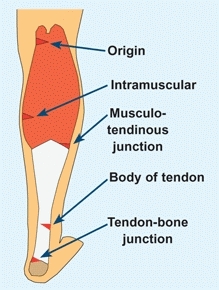
B Musculotendon injuries Injuries of this complex may occur at different locations.
Synchondrosis disruptions
Accessory ossification centers may become separated from their parent bone. The classic examples are the bipartite patella [C], accessory tarsal navicular, and accessory ossicles below the ankle malleoli.

C Bipartite patella Stress injuries can disrupt the chondral junction between the patella and the ossicle, causing a synchondrosis disruption.
Physeal injuries
are classified by the fracture patterns [D]. Repetitive stress injury may damage the growth plate in a unique fashion. These stress-induced physeal injuries are most common about the wrist and upper humerus in the child. Stress results in a disruption of the growth plate, as seen in type 5 injuries. Unlike the usual simple physeal fracture, the growth plate becomes widened, irregular, and tender but not grossly unstable. Such injuries may result in physeal damage and altered growth. Type 5 injuries occur in the distal radial epiphysis in gymnasts and in the proximal humeral epiphysis in pitchers.
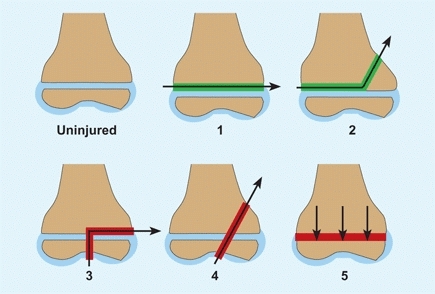
D Salter-Harris classification of growth plate injuries These are classified as types 1 through 5, based on the fracture pattern. Types 1 and 2 (green lines) do not traverse the epiphysis and usually do not cause growth problems. Types 3 to 5 (red lines) may cause growth arrest and progressive deformity.

E Sites of traction injuries These are common sites and activities leading to the injury.
Traction and compression bone injuries
Traction injuries may be acute or chronic and cause bony failure or inflammation at the tendon-bone junction [E, previous page]. Compression injuries are usually chronic, with the classic example being the lateral compartment of the elbow in “little league elbow.” Throwing causes compression of both the capitellum and radial head, which may cause vascular damage and bone necrosis.
Juvenile Osteochondroses
This is a term describing a heterogeneous group of conditions that are characterized by sclerosis and fragmentation of the epiphysis or apophysis in the immature body. Irregular ossification may be a normal variation of ossification or represent a disorder. Classic descriptions include many sites [A]. More details are found in Chapter 1.
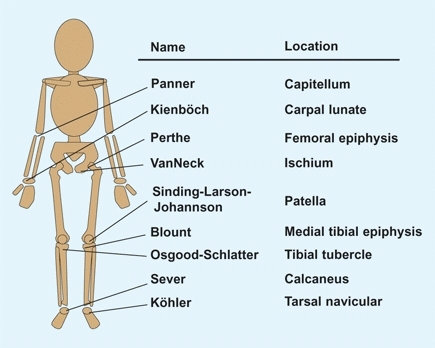
A Classic list of osteochondroses Name and location are shown.
Osteochondritis Dissecans
Osteochondritis dissecans (OCD) is a segmental avascular necrosis of articular subchondral bone. These OCD lesions are most common at the end of growth and during early adult life and are more common in joints subjected to repetitive microtrauma. OCD lesions may be familial and may occur in several locations in the same individual.
These are lesions that affect the subchondral bone and cartilage of a joint. These lesions are discussed in chapters on their various anatomic locations, but some general features are appropriately discussed under sports because the lesions are often seen in the immature athlete and pose questions in management and athletic participation.
Etiology
The causes of OCD are probably multiple. The predisposing factors include marginal vascularity, possible constitutional factors such as a coagulopathy, and repetitive microtrauma.
Classification
Lesions may be classified anatomically [B] and based on radiographic or MR imaging. Assess activity and healing potential by dynamic bone scan in younger patients.
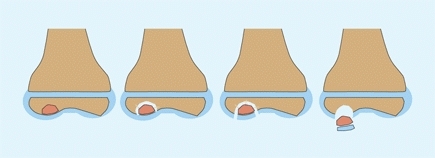
B Osteochondritis dissecans These are the stages of this disease. Over time the lesion may become unstable and finally separate into the joint and become a loose body.
Location of lesions
Lesions occur in the knee [C], talus, capitellum, patella, radial head, and femoral head. Femoral head OCD may be idiopathic but usually complicates LCP disease and avascular necrosis secondary to trauma and infection.

C Osteochondritis dissecans Lesion not seen on AP radiograph, but shown on notch (red arrow) and lateral (yellow arrow) views.
Natural history
OCD has the potential to cause permanent disability [E] and is one of the more serious sports-related problems for the young athlete. The prognosis is better for smaller lesions, early onset, and a favorable location. Most small lesions in children heal spontaneously. Disability is more likely for large lesions in load-bearing areas of joints, such as the lateral femoral condyle, that progress to separation [D].
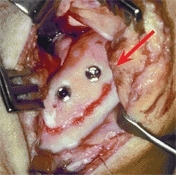
D Replaced large osteochondritic fragment This large lesion was replaced and fixed with two screws.

E Age and outcome for OCD lesion of the knee Based on 509 OCD lesions from Hefti (1999).
Management
Treatment depends upon the age of the patient and the location, size, and stage of the lesion. In younger patients, small lesions that are stable may require only nonoperative management, primarily rest. Larger unstable lesions, especially in weight-bearing locations, are best managed more aggressively [D]. See Chapters 9 and 10, respectively, for the foot and knee.
Overuse Injuries
Between 30% and 50% of injuries of immature athletes are due to overuse. This varies from about 15% in soccer to 60% in swimmers. Sports that require repetitive acts are most likely to cause overuse problems. As compared with acute injuries, overuse injuries take longer to heal and result in more time away from competition.
Most injuries are the result of excessive demands on an unprepared system. Extremity malalignment, limited flexibility, excessive demands, and improper equipment and playing surfaces increase the risks.
Overuse injury seldom occurs in the normal play of children. The protective mechanism of pain limits overuse and promotes recovery. This protective mechanism is often repressed during regimented childhood sports. Addition risk factors are the long seasons and single sport participation. A large portion of sports medicine in children deals with the care of these overuse conditions.
Mechanism
Overuse injuries result from repetitive submaximal loading. The injuries from this microtrauma are usually reversed by rest. Repetitive microtrauma without intervals of rest is cumulative and causes stress injuries.
Stress injury to bone creates a progression of inflammation, periosteal swelling, and endosteal and cortical disruption. Stress injuries in children include fractures through the growth plate [A] or bone [B] and disruption of bone to tendon or muscle junctions. They may also affect the vascularity of bone, resulting in bone necrosis, as seen in osteochondritis dissecans. Before an overt fracture occurs, the injuries are referred to as stress reactions.
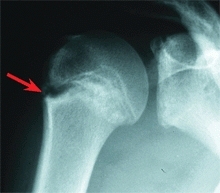
A Physeal stress injuries This adolescent pitcher developed a stress reaction causing widening of the proximal humeral physis (red arrow).

B Spondylolisthesis This gymnast had back pain and a grade I spondylolisthesis. This is due to a stress fracture through the pars.
Sites of Overuse Injuries
The location of the injury depends upon the stresses created during specific activities of each sport. For example, wrist and back pain from overuse are common among gymnasts, swimmers have shoulder pain, whereas runners’ injuries occur in the lower limbs [C].


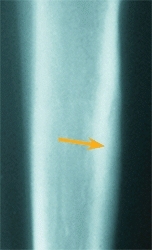
C Tibial stress fracture A 17-year-old female cross country runner has had “shin splints” for 3 months. The proximal tibia is tender. A plain radiograph (left) is negative, whereas the bone scan shows an area of increased uptake over the upper tibia (red arrow), and the CT scan shows sclerosis (orange arrow).
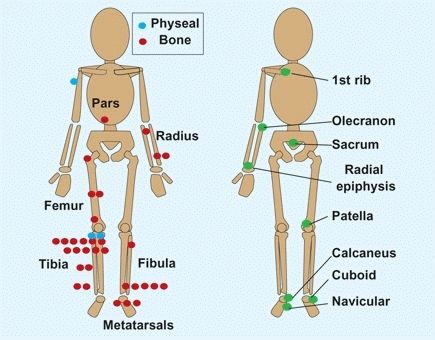
D Common and rare sites of stress fractures in children Common sites (red and blue dots) include both physeal and bony fractures. Rare sites of stress fractures (green dots) are shown on the right. Each dot represents a case in the series. From Walker (1996).
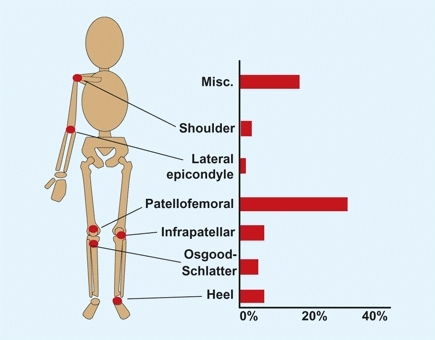
E Sites of overuse injuries Based on 139 athletes aged 9–16 years, from Dalton (1992).
Diagnosis
Make an accurate diagnosis to be certain that some more serious problem is not the cause of pain.
History
should include the type of sporting activity associated with the onset, training (including frequency and duration), previous injuries, new techniques or equipment, and whether the patient is in a period of rapid growth. Detail the onset, character, location, and pain relationships with activity and time of day. Beware of night pain, as this can be a sign of a tumor.
Pain severity
Based on the history, it is often useful to grade pain severity.
Grade I
pain with excessive activity.
Grade II
pain with moderate activity.
Grade III
pain with routine daily activities.
Examination
Localize the pain and determine the site of maximum tenderness. This will often help to establish the diagnosis [D and E, previous page]. Localized tenderness to the tibial tubercle is classic for Osgood-Schlatter disease, and tenderness over the origin of the plantar fascia and insertion of the Achilles tendon are classic findings for the common heel pain in children. Look for evidence of malalignment problems in lower limbs, such as the combination of femoral antetorsion and external tibial torsion or malalignment of the quadriceps mechanism.
Assess the interaction of the parent(s) and patient. Overzealous and controlling parents may aggravate the problem. Be concerned if the parent talks more than the child and makes comments that do not fit the appearance of the child. Such comments as “best athlete on the team,” “tough minded,” or “plays with pain” may be used to describe a child who is detached and unathletic appearing.
Attempt to assess the patient’s attitude regarding physical education: Is participation a positive or negative experience for the patient? Does the patient exaggerate the disability in an attempt to get a PE excuse, or is the injury being minimized to reduce the risk of being benched, or is the injury overplayed to avoid unwanted participation forced on the patient in the first place?
Differentiating stress fractures from neoplasm or infection
This is usually not difficult. Stress fractures occur in specific locations and show typical clinical and imaging features [A and B]. Assess the effect of rest. With rest, the pain and tenderness of stress fractures resolve or improve over a period of days. If the clinical features are atypical and the early differentiation important, image with CT scans to show the fracture line, bone scans to exactly localize the lesion, and laboratory studies of CRP and ESR to aid in differentiating infections.

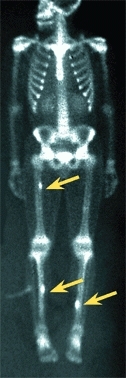
A Imaging stress fractures Often the location and radiographic appearance of stress fractures is diagnostic on plain radiographs, such as this proximal tibia (red arrow). Stress fractures may be multiple, as shown by a bone scan (yellow arrows).


B Metatarsal stress fracture This 14-year-old runner complained of foot pain and demonstrated localized tenderness over the third metatarsal. Initial radiographs (left) were negative. Radiographs three weeks later show the fracture and callus (arrow).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


