fibrosarcoma, malignant fibrous histiocytoma, and extraskeletal osteosarcoma (10).
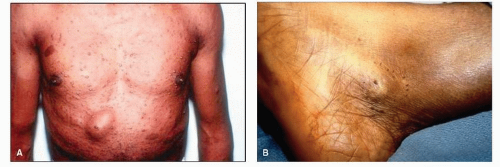 Figure 92.1 A: A patient with von Recklinghausen disease. Note the cutaneous and subcutaneous nodules and the numerous cafe au lait spots. B: The same patient presented with a neurofibroma in the tarsal tunnel. |
sometimes regress over time. Stage 2 (benign, active) lesions are histologically benign, are intracapsular, and also do not metastasize. Although intracompartmental, these lesions may distort or compress natural barriers. They are often painful and actively enlarge. They are freely movable within the soft tissues. Stage 3 (benign, aggressive) lesions are histologically benign. They are sometimes extracapsular and can cross compartmental barriers. Usually, these masses are painful, rapidly growing, and fixed to the underlying tissues. Most important, these lesions may undergo malignant transformation.
TABLE 92.1 Histologic Classification of Soft Tissue Tumors | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 92.2 American Joint Commission Staging System for Soft Tissue Sarcomas | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 92.3 Enneking System for Staging Soft Tissue Sarcomas | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 92.4 Hajdu System for Staging Soft Tissue Sarcomas | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
otherwise may have gone unrecognized if not in the foot, the lesion may be more readily diagnosed, leading to better treatment options.
TABLE 92.5 Enneking System for Staging Benign Soft Tissue Masses | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Figure 92.2 Measurement of size of a tumor on the plantar aspect of the foot. |
involvement is present, the patient may be able to map out an area of parasthesias distal to the lesion or surrounding the lesion that is indicative of the particular nerve involved (Fig. 92.5).
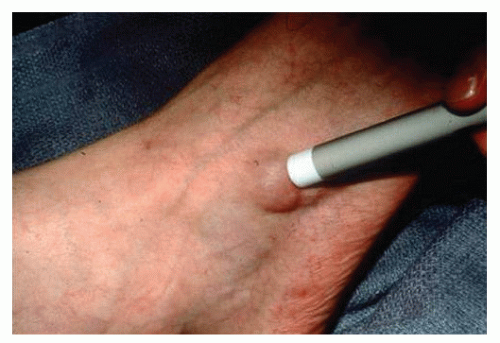 Figure 92.3 A penlight held against a cystic mass, such as a ganglion, transilluminates (i.e., causes light to pass through the walls of the mass). Conversely, a solid mass does not transilluminate. |
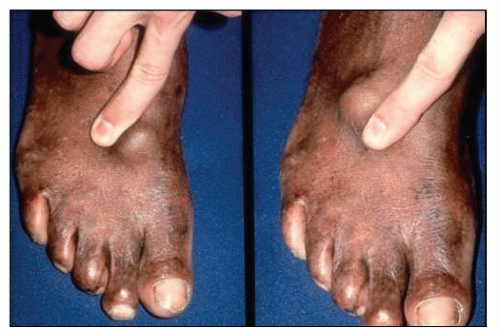 Figure 92.4 A mass on the dorsum of the foot that is freely movable. This strongly suggests that the mass is subcutaneous and is not underneath the deep fascia. |
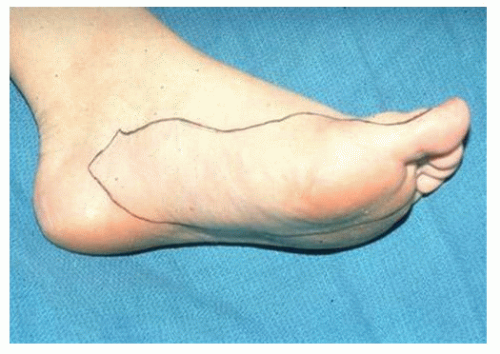 Figure 92.5 A patient can be given a marker and asked to outline the area of pain or sensory distortion. In the case of a nearby soft tissue mass, this can provide the clinician with clues about potentially compressed nerves. In this figure, a mass is present in the arch, and the patient has roughly outlined the distribution of the medial plantar nerve, thus strongly intimating that this nerve is compressed by the mass. |
ultrasound enhanced by duplex ultrasonography (19). Since the advent of computed tomography (CT) and magnetic resonance imaging (MRI), ultrasound has become a less frequently used diagnostic tool for the evaluation of soft tissue masses.
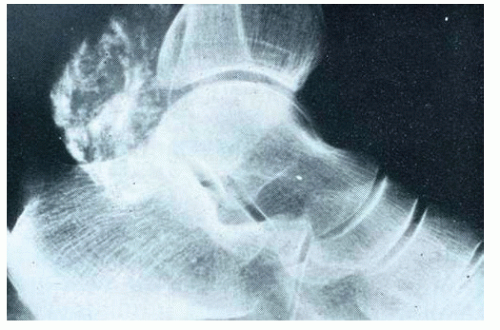 Figure 92.6 Soft tissue mass in the tarsal tunnel. Radiographs of the ankle demonstrated significant intralesional calcification of the mass. This mass was examined by biopsy and was found to be a malignant schwannoma. |
 Figure 92.7 Soft tissue mass of the forefoot. Radiographically, one can see pressure changes from the mass on the second metatarsal and the increased soft tissue density in the area. This mass was ultimately determined to be a benign fibrolipoma. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


