Is appropriate in patients with segmental bone loss following tumor resection and in selected nontumor patients. Just as the surgical plan for sarcoma resection is individualized for each patient based on the extent of tumor involvement of bone and soft tissues, selection of the reconstructive procedure must also be tailored to the individual patient based on the functional potential of the remaining bone and soft tissues as well as the patient’s needs and desires.
Shoulder arthrodesis following sarcoma resection is an excellent reconstructive choice for a young patient who desires a strong and stable shoulder girdle. Specifically, for young patients who require an extra-articular resection, (the proximal humerus and glenoid [Fig. 28.1A-C]), arthrodesis with use of an intercalary allograft supplemented with a vascularized fibular graft (Fig. 28.1P) is an excellent reconstructive option.
Likewise, in the nontumor patient, arthrodesis may be an appropriate salvage operation after multiple failed arthroplasties or stabilization procedures and may also be a consideration in a patient with chronic infection or posttraumatic brachial plexus injury. Table 28.1 lists indications for consideration of shoulder arthrodesis.
The goal of shoulder arthrodesis is to achieve a pain-free, stable shoulder girdle that optimizes upper extremity strength. Again, the functional needs and desires of the patient should strongly influence selection of the reconstructive method.
Arthrodesis is contraindicated if another reconstructive procedure can be performed that preserves or restores more function.
In general, arthrodesis is contraindicated when postresection function of the deltoid and rotator cuff musculature is maintained and either the glenoid or proximal humerus can be preserved or adequately reconstructed. For example, isolated resection of the glenoid can be reconstructed with an allograft or custom implant.
TABLE 28.1 Indications for Shoulder Arthrodesis | |
|---|---|
|
 FIGURE 28.1 Wide resection of an osteosarcoma of the proximal humerus in a 15-year-old male patient. A: Plain radiographs of the proximal humerus showing mixed osteolytic and osteoblastic osteosarcoma. B: T1-weighted coronal magnetic resonance image of the proximal humerus showing intra-articular tumor extension after preoperative chemotherapy (arrow). C: T2-weighted axial images after preoperative chemotherapy. D: The incision begins at the midclavicle and courses laterally and distally to include the deltopectoral interval with elliptical excision of the prior biopsy site (if present). A second incision is made at a 90-degree angle from the first incision, beginning medial to the coracoid and coursing superiorly over the clavicle and then distally over the midline of the scapula. (Used Mayo Foundation for Medical Education and Research, with permission.) |
 FIGURE 28.1 (Continued) E: The pectoral is major tendon is divided from its humeral insertion; the underlying visible structure includes the conjoined tendon and long head of the biceps. (Used Mayo Foundation for Medical Education and Research, with permission.) F: Intraoperative photograph showing the elliptical skin incision around the prior biopsy site (white arrow). The pectoralis major tendon has been reflected, and the conjoined tendon is freed from coracoid (black arrow). G: After reflection of the long and short heads of the biceps and pectoralis minor, the neurovascular bundle is identified in the proximal aspect of the wound. The musculocutaneous nerve and radial nerve are identified. (Used Mayo Foundation for Medical Education and Research, with permission.) H: Intraoperative photograph showing a proximal loop around the anterior circumflex vessels and musculocutaneous nerve and a distal loop around the median nerve. |
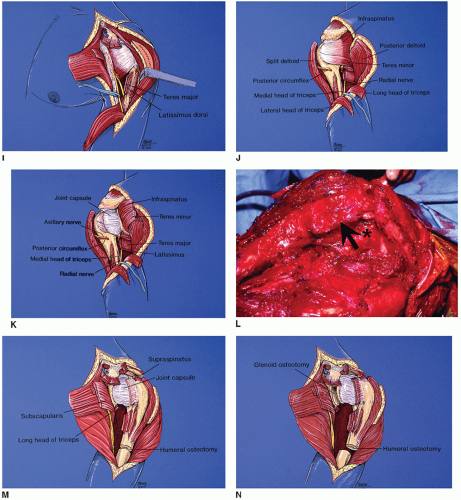 FIGURE 28.1 (Continued) I: The broad insertion of the latissimus dorsi is divided from the humerus and just posterior to this is the insertion of the teres major. The radial nerve is identified and protected. (Used Mayo Foundation for Medical Education and Research, with permission.) J: The posterior dissection begins with the deltoid released from the acromion and scapular spine and divided along the posterior aspect of the biopsy site, and the posterior aspect of the rotator cuff musculature is identified. The posterior humeral circumflex vessels are ligated, the axillary nerve is transected (if necessary), the long head of the triceps is released from the inferior glenoid, and the lateral head of the triceps is released from the proximal humerus. The posterior humeral circumflex vessels and axillary nerve are located in the quadrangular space formed by the teres minor (superior), long head of the triceps (medial), teres major (inferior), and lateral head of the triceps (lateral). (Used Mayo Foundation for Medical Education and Research, with permission.) K: The infraspinatus and teres minor are divided to expose the posterior capsule of the shoulder joint. (Used Mayo Foundation for Medical Education and Research, with permission.) L: Intraoperative photograph showing division of the infraspinatus and teres minor (arrow), with exposure of underlying posterior capsule (asterisk). M: Attention is directed again anteriorly, and the supraspinatus and supscapsularis are transected to expose the anterior and superior joint capsule. (Used Mayo Foundation for Medical Education and Research, with permission.) N: Drawing of the anterior aspect of the glenoid osteotomy medial to the joint capsule. (Used Mayo Foundation for Medical Education and Research, with permission.) |
 FIGURE 28.1 (Continued) O: Intraoperative photograph of the posterior aspect of the glenoid osteotomy. Vessel loops identify the axillary nerve (proximally) and the radial nerve (distally). The distal humeral osteotomy is made, the marrow sampled for frozen-section analysis, and the specimen removed. P: Illustration of the reconstruction with an intercalary allograft bridging the remaining scapula and humerus (acromion and clavicle not illustrated) with vascularized fibular graft spanning from scapula to humerus. (Used Mayo Foundation for Medical Education and Research, with permission.) Q: Intraoperative photograph of intercalary allograft. The articular surface of the allograft is cut to match the glenoid osteotomy with the allograft in the desired position of arthrodesis. Contact is also made between the allograft and the denuded undersurface of the acromion. Large cannulated screws are first placed across the proximal allograft into the host glenoid and scapula. A pelvic reconstruction plate is then contoured and fixed from the scapular spine to the allograft. R: Postoperative radiograph. After placement of the pelvic reconstruction plate, the vascular anastomosis for the fibula is then performed, followed by placement of a second plate to fix the distal allograft to the host residual humeral diaphysis and screws to fix the vascularized fibular graft. Supplemental cancellous bone graft is placed at both the proximal and distal osteotomy junctions. Note cement augmentation of allograft intramedullary canal and near-complete spanning of allograft with fixation. Ideally, there is overlap of the plate fixation. |
 FIGURE 28.1 (Continued) S: At 3 years after surgery, the patient is disease free, with a solid arthrodesis and active abduction and forward flexion of 85 degrees. |
With resection of only the proximal humerus, reconstructive options include an allograft-prosthetic composite, proximal humeral replacement implant, osteoarticular graft, or fibular graft (vascularized or nonvascularized), as described elsewhere in this volume.
Patients with degenerative shoulder arthropathy and nonreconstructable rotator cuff disease may be candidates for reverse total shoulder arthroplasty.
Specific contraindications for shoulder arthrodesis include lack of active scapulothoracic motion.
Patients at high risk of nonunion such as elderly patients or those with neuropathic arthropathy are poor candidates.
Because of postoperative functional limitations, bilateral shoulder arthrodeses should not be performed.
the location of the mouth underneath the surgical drapes should be identified; while determining the position of arthrodesis, the surgeon verifies that the patient’s hand can reach his or her mouth without excessive scapular winging. Surgery can also be performed with the patient in a lateral position; I favor the supine beach chair position to facilitate appropriate positioning of the arthrodesis.
TABLE 28.2 Preoperative Preparation for Shoulder Arthrodesis | ||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 28.3 Suggested Position of Arthrodesis | ||||
|---|---|---|---|---|
|









