Rotating Hinge for Revision Total Knee Arthroplasty
Richard E. Jones
Most patients who require revision total knee arthroplasty (TKA) can be managed adequately with posterior stabilized or varus-valgus constrained prostheses. However, if there is massive loss of bone or substantial compromise of soft tissue support and stability, a rotating hinge prosthesis may be necessary.
Walldius (1) described the initial use of a hinge for TKA, and it was used in primary and occasionally, in revision circumstances. Early hinge designs had unidirectional sagittal plane motion, metal-to-metal articulations, a paucity of sizes, and flat trochlear grooves, resulting in high rates of implant failure and complications (2,3).
Hinged TKA designs evolved, with dual articulations with built-in rotation introduced, when it was recognized that rotation is necessary to preserve some degree of gait kinematics and to ensure reasonable midterm implant survivorship. Newer designs had broad articulation surfaces to decrease deleterious stresses and better distribute load. Also, greater availability of implant sizes and manufacturing techniques produced more reliable clinical outcomes with contemporary rotating hinge TKA (4, 5, 6).
INDICATIONS
The goals of revision TKA surgery include bone preservation, restoration of symmetrical soft tissue support, establishment of the joint line, and alignment and balance of the knee. In principle, the extent of implant constraint should be consistent with the clinical situation. This chapter describes the surgical indications and technique for one particular system, the S-ROM rotating hinge (DePuy, Warsaw, IN), when maximum constraint is necessary during revision TKA.
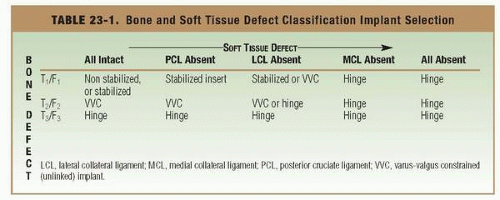
The indications for a rotating hinge knee arthroplasty for revision TKA include (a) loss of the medial and/or lateral collateral ligaments, (b) extensive bone loss of Engh type II (metaphyseal loss with cortical shell intact) or Engh type III (loss of metaphyseal and cortical shell, including collateral insertions), (c) severe flexion-gap imbalance necessitating a linked system, and (d) sagittal instability with non-reconstructible extensor mechanism loss (Table 23-1).
In primary TKA, the rotating hinge option has provided positive outcomes for patients with neuromuscular diseases and conditions (e.g., poliomyelitis) that result in a flail or back-knee deformity from quadriceps weakness. The hinge axle-yoke mechanism of several rotating hinge knee arthroplasty systems provides for 5 degrees of hyperextension with a positive stop. This allows knee stabilization and an acceptable gait pattern for such patients. Patients undergoing TKA for traumatic arthrosis or take- down of a prior arthrodesis may have large flexion gaps at reconstruction, which may require use of a rotating hinge TKA.
 |
SURGICAL TECHNIQUE
Appropriate preoperative assessment is essential, and good planning is the hallmark of successful surgical outcomes. The use of a hinge is often a backup contingency, because many patients will require less constraint than anticipated at the time of reconstruction. Nonetheless, when ultimate constraint is needed, a rotating hinge is a practical option (Figs. 23-1 and 23-2).
The revision knee is evaluated under anesthesia for alignment, stability, and length. Selection of a skin incision in a knee with multiple previous incisions is dictated by the cutaneous vascular anatomy predominantly coursing from the medial side. Typically, the most lateral incision should be selected and excised upon approach. Thick fasciocutaneous flaps maintain the best blood supply. After arthrotomy, complete debridement of the often-thickened synovial scar removes debris and pathologic tissue and helps mobilize the extensor mechanism for retraction and exposure.
The author’s favored approach is midvastus parapatellar arthrotomy, extending 5 to 7 mm distal, along the medial tibia to elevate a continuous sleeve of soft tissue. This allows patella subluxation without eversion, and external tibial rotation and forward subluxation expose the lateral tibial plateau. This exposure precludes the need for rectus snip, tibial tubercle osteotomy, or other quadricepsplasty techniques and is stable upon closure. It has been the author’s surgical approach technique in more than 300 consecutive revision TKAs.
The revision TKA sequence begins with establishment of a stable tibial base. Careful removal of the tibial component is best accomplished by interrupting the interface with a small oscillating saw blade (Fig. 23-3). Cement chisels, punches, mallet, and extraction devices can be used to remove the tibial component (Fig. 23-4). Cement, wear debris, and interface tissues are completely excised with a combination of saws, burrs, curettes, and rongeurs. Jet lavage is essential to expose a clean, vascular bone bed.
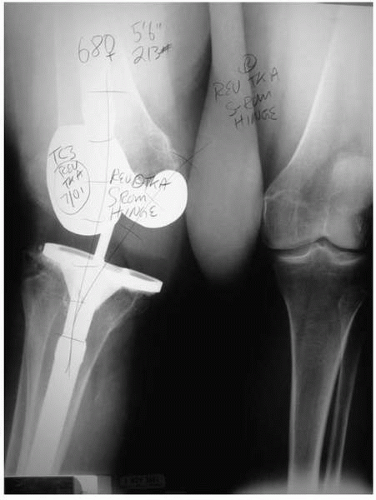 FIGURE 23-1 Preoperative anteroposterior radiograph of a 68-year-old female after revision total knee arthroplasty, with a varus-valgus constrained but unhinged implant with medial collateral deficiency. |
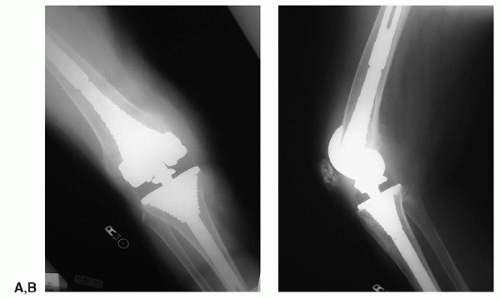 FIGURE 23-2 (A,B) Postoperative anteroposterior and lateral radiographs 48 months after S-ROM Rotating Hinge revision total knee arthroplasty. |
This author prefers an intramedullary mounted instrument system, which requires progressive reaming of the tibia to achieve a cortical diaphyseal fill, anchoring the stem in good bone, followed by use of a tapered metaphyseal sleeve (Figs. 23-5 and 23-6). Larger metaphyseal defects may require the 150-mm stem, rather than the standard 100-mm stem, to provide the most stable construct.
Intramedullary pilot stems sized to the reaming diameter are mounted on metaphyseal sleeve broaches, and the tibial metaphysis is broached. Broach sizes are progressively increased until rotational stability is achieved and metaphyseal filling occurs (Fig. 23-7). Bone is trimmed using the top of the sleeve as a guide, and an appropriately sized tibial base plate is applied (Fig. 23-8
 Traditional Medial Approaches to the Knee
Managing Patella Problems in Primary Total Knee Arthroplasty
Varus and Valgus Deformities
Simultaneous Total Knee Arthroplasty and Femoral Osteotomy
Impaction Bone Grafting for Large Bone Defects
Unicompartmental Total Knee Arthroplasty With Conventional Instrumentation
Traditional Medial Approaches to the Knee
Managing Patella Problems in Primary Total Knee Arthroplasty
Varus and Valgus Deformities
Simultaneous Total Knee Arthroplasty and Femoral Osteotomy
Impaction Bone Grafting for Large Bone Defects
Unicompartmental Total Knee Arthroplasty With Conventional Instrumentation




Related posts:
Traditional Medial Approaches to the Knee
Managing Patella Problems in Primary Total Knee Arthroplasty
Varus and Valgus Deformities
Simultaneous Total Knee Arthroplasty and Femoral Osteotomy
Impaction Bone Grafting for Large Bone Defects
Unicompartmental Total Knee Arthroplasty With Conventional Instrumentation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
