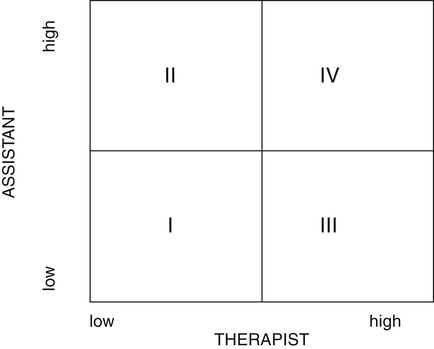
In some states, therapy assistants need a license to practice. The fields of occupational therapy and physical therapy have separate practice acts and different licensing agencies, which can affect the staffing options of hand therapy programs. Typically, OTAs must work under the supervision of OTs and follow an occupational therapy plan of care,1 and PTAs must work under the supervision of PTs and follow a physical therapy plan of care. A PTA with hand experience can be added to a hand therapy program only if the assistant reports to a PT. However, more OTs practice hand therapy than do PTs. These types of considerations affect staffing decisions. The therapist sets the standard of care for the program. The assistant is responsible for adhering to these standards. Ideally, therapists and assistants work collaboratively. The term collaboration has more than one definition; in this sense, it means “working together, especially in a joint intellectual effort.”2 By definition, collaboration implies a hierarchy with the assistant reporting to the therapist. The hand therapist is responsible for the care that the client receives; the therapist also determines the level of supervision that an assistant requires. The assistant aids in the client’s goal setting and contributes ideas for the client’s program.1 Assistants’ responsibilities are increased as appropriate, depending on their clinical skills. All therapists and assistants are responsible for learning about and following their state laws concerning supervision and scope of practice. The hand therapy experience matrix (Fig. 10-1) is a model of collaborative roles for therapists and assistants.3 The x axis represents the therapist’s level of experience in hand therapy. The y axis represents the assistant’s level of experience in hand therapy. The hand therapy team’s goal is to move to a higher quadrant through supervision and training with competencies demonstrated in a manner consistent with state and facility guidelines. In quadrant III, an experienced therapist is working with an inexperienced assistant. The therapist can help train the assistant, and competencies can be achieved in accordance with the facility’s guidelines, maximizing the assistant’s potential to broaden clinical skills. In this team, it is important for the therapist to supervise the assistant closely. The therapist should create a structured learning program with the assistant’s assistance, identifying reading assignments, reviewing cases, and sharing resources from conferences and journals. This enrichment is more meaningful if it is shaped to match existing clients. For example, if a client has just been referred to you and your assistant for therapy after repair of the flexor pollicis longus, try to make that diagnosis your topic of study so that it is relevant to your case. If you have a client with adhesions, study scar management with your assistant and ask the OTA or PTA how the knowledge gained can be applied to the client’s treatment. Box 10-1 presents a tool that can help assistants develop their clinical reasoning capabilities in reviewing hand therapy cases. BOX 10-1 Clinical Reasoning Tool for Hand Therapy Case Reviews Client: ______________________________________ Diagnosis: ___________________________________ Date: _______________________________________
Roles of Therapy Assistants in Hand Therapy
Hand Therapy Experience Matrix
Wounds
Drainage
Edema
Pain
Scar
AROM limitations
PROM limitations
Intrinsic tightness
Extrinsic extensor tightness
Extrinsic flexor tightness
Joint tightness
Joint end-feel
Hard
Spongy
Soft
Precautions
Structures to treat
Interventions
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Roles of Therapy Assistants in Hand Therapy