Fig. 10.1
Sport climbing
10.2.1.2 Bouldering
Bouldering consists of ropeless climbing involving a short sequence of powerful and technical moves to complete the graded route on large rocks. Bouldering can be done without a partner and with minimal equipment – climbing shoes and crash pad. Falling onto one’s feet or body is a normal part of bouldering, whether a route is completed or not [4, 30] (Fig. 10.2).

Fig. 10.2
Bouldering
10.2.1.3 Deep Water Soloing
Deep water soloing (DWS), also known as “psicobloc”, is solo rock climbing, practised on sea cliffs at high tide, that relies solely upon the presence of water at the base of a climb to protect against injury from falls. These routes can be up to 20+ metres high, and lately some of the hardest climbs in the world have been established in that styles (e.g. Chris Sharma, Es Pontàs, Spain) (Fig. 10.3).

Fig. 10.3
Deep water soloing
10.2.1.4 Traditional Climbing
Traditional (alpine) climbing (or trad climbing) emphasises the skills necessary for establishing routes in an exploratory fashion outdoors. The lead climber typically ascends a section of rock while placing removable protective devices where possible along the climb. Falls can therefore be longer than those experienced when sport climbing. Unreliable fixed pitons may occasionally be found on older established routes. As physical hazards are likely, the use of a helmet is considered mandatory. Above around 2500 m, psychological altitude-induced adaptations must also be factored into the climbs [4, 30] (Fig. 10.4).

Fig. 10.4
Alpine climbing
10.2.1.5 Indoor Climbing and Competition Climbing
Indoor climbing and competition climbing are performed on artificial structures that try to mimic climbing outdoors but in a more controlled environment. As physical hazards are almost totally eliminated, such climbing became an extracurricular sport in many countries. National and international competitions are held on such walls and involve three major disciplines – lead climbing (i.e. sport climbing), speed and bouldering. Indoor bouldering is performed above thick foam mat flooring [4, 30] (Fig. 10.5).
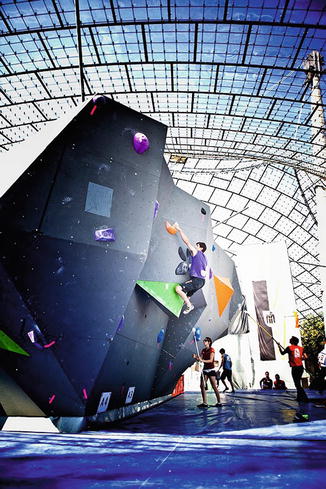
Fig. 10.5
Competition climbing
10.2.1.6 Ice Climbing
Ice climbing normally refers to roped and protected climbing of features such as icefalls, frozen waterfalls and cliffs and rock slabs covered with ice refrozen from flows of water. Equipment includes ice axes for hands and crampons for feet. Physical hazards like avalanches, rock and icefalls are present [4, 30, 31] (Fig. 10.6).

Fig. 10.6
Ice climbing
10.2.1.7 Free Solo Climbing
In contrast to the public perception, real free solo ascents are rare and don’t play a major role in the current climbing sports. Nevertheless if performed they usually get a high media attention, thus mimicking a higher prevalence. The injury and fatality risk is obviously high.
10.2.2 Main Psychological and Anthropometric Characteristics
Based on the fact that climbing is not a cyclic but a poly-structural sport, it is difficult to evaluate the performance-limiting factors, of which many are still not verified [32–36]. One important factor is the anthropometric profile of the athletes, which was subject of a few studies of general climbers and elite competitors in lead climbing (sport climbing) [32, 37–41]. In the scientific literature climbers are described as being relatively small in stature and having a very low percentage of body fat [32]. Unexpectedly, their hand grip strength measured via dynamometer does not differ from non-climbers, because of the nonspecific grip position in this test [36, 38–40]. Elite climbers are also stronger with the left hand (which is more often the nondominant hand) than recreational climbers and non-climbers [38]. The reason is probably connected to the fact that climbing develops strength and agility for both hands [32]. Many components have been proposed which correlate with the overall climbing performance [32, 33, 36]. However, some authors have proven the major importance of the specific strength endurance in sport climbing with strong correlation coefficients [42–44]. More recent studies support the fact that rock climbing requires harmoniously developed physical fitness, technical and tactical skills, as well as mental preparation [43 ] (Fig. 10.7).
Fig. 10.7
Correlations between the red point achievements and some of the factors of performance, Michailov (2006) [43]
10.2.3 Psychological and Behavioural Characteristics
The psychological and behavioural characteristics of any climbing subdiscipline are rarely studied, though they are a key performance variable that may additionally have an influence on injuries and fatalities sustained [46–48]. It is generally accepted that those rock climbers high in self-efficacy participate more frequently, take calculated additional risks and attempt harder climbs when they feel confident in their abilities, though this is rarely studied [4, 46].
10.3 Benefits from This Sport
Learning to climb has never been easier with the advent of indoor artificial climbing walls found in many cities [20]. In some schools it even forms part of the sport curriculum [1, 49]. Rock climbing participation is accessible at all ages, toddler to pensioner [1, 33, 49, 50], and is enjoyed by many over a lifetime. In a recent study we analysed our climbing patients between 2009 and 2012, where we saw climbers between a range of 11–77 years of age and 0.3–64 years of climbing [51]. Climbing sport is a lifelong activity with many health benefits, e.g. musculoskeletal training, equilibrium and mental training as well as minor injury risk [1]. Both genders can easily climb together and perform at an even level [1]. Its potential in rehabilitation and physiotherapy is widely used, as well as in behavioural training and social rehabilitation programmes [52–55].
10.4 Acute Injuries and Fatalities
Extensive studies on injuries in general rock climbing [1, 3, 4, 14, 15, 18, 21, 28, 56–65], indoor climbing [6, 18, 20, 24] and competition climbing [8, 49] exist, including analysis of the injury risk per 1000 h. Severe injuries during indoor or competition climbing are rare, but do happen [14, 15, 18–24, 27, 28, 49, 61, 64, 66–71]. Most injuries in rock climbing occur on the upper limbs, notably the fingers, and are generally a result of overstraining rather than acute injuries [19, 29, 69, 72–76]. Nevertheless in some studies more lower limb injuries are found [6, 11, 65]. Most injuries involve fractures, sprains and dislocations [3, 19, 28, 65, 76]. To date no known study has objectively demonstrated that ice and rock climbing are high-risk sports or that those climbing higher grades are more prone to experience severe injuries compared to those climbing lower grades. Nevertheless the media’s lurid depiction of elite rock and ice climbers has helped to create a perception of climbing as being a hazardous and high-risk sport [77, 78]. For example, a 1999 Time Magazine cover featured a sport climber with the headline “Why we take risks” with a subtitle stating “From extreme sports to day trading thrill seeking is becoming more popular” [78].
To objectively analyse and compare injuries from different sports, a common scoring system for the grading of the injuries is essential. In general, when assessing whether a sport presents a high risk of injury or death, a distinction between overstrain (overuse) injuries and acute injuries or accidents should be made [4]. The reason is overstrain injuries are generally less severe and can generally be avoided with informed training, whereas an examination of the injury rate for acute sport-specific injuries, especially their severity, is crucial.
Most authors [5, 10, 11, 65, 76, 79] found that fractures, strains and sprains account for most injuries. Schöffl et al. [76] found the most common climbing injury the closed pulley rupture and the most common overuse injury the tenosynovitis of the finger flexor tendons. These pulley injuries are almost rock climbing-specific pathologies and matter of extensive research [60, 80–85]. Overall the majority of all injuries in the studies on outdoor and alpine climbing as well as bouldering studies were of minor severity (UIAA MedCom 1-2) [10, 15, 28, 60, 62–64, 70, 86].
Few studies examined ice-climbing injuries and overuse syndromes. In our study [31] we found that most of the acute injuries (61.3 %) occurred while lead climbing, 23.8 % while climbing second, and the rest was rare (6.3 % belaying, 3.8 % on return and 2.5 % on approach, other 2.5 %). Most of the acute injuries (73.4 %) happened in a waterfall, few in glacier ice walls (11.4 %) and on artificial ice walls (2.5 %). Climber fall-related acute injuries amounted for 10.5 %.
As there was an inconsistency in the use of scores for climbing studies and thus a lack of inter-study comparability, the Medical Commission of the UIAA (International Mountaineering and Climbing Federation) gave a consensus statement on injury and illness definition in mountain sports and proposed a new UIAA MedCom-Score88, which showed its value already in recent studies by Neuhof et al. [79] and Schöffl et al. [6]. The UIAA MedCom Score uses the OSICS 10 [88–90] tables for injury distribution and a new classification (Table 10.1). In addition a fatality risk classification and guidelines to evaluate a time-related injury risk are given [87].
Table 10.1
UIAA MedCom Score 2011 [87]. Injury and Illness Severity Classification (IIC) – UIAA MedCom Score
Score | Description |
|---|---|
0 | No injury or illness |
1 | Mild injury or illness, no medical intervention necessary, self-therapy (e.g. bruises, contusions, strains) |
2 | Moderate-severe injury or illness, not life threatening, prolonged conservative or minor surgery, outpatient therapy, doctor attendance within a short timeframe (days), injury-related work absence, heals without permanent damage (e.g. undisplaced fractures, tendon ruptures, pulley ruptures, dislocations, meniscal tear, minor frostbite) |
3 | Major injury or illness, not life threatening, hospitalisation, surgical intervention necessary, immediate doctor attendance necessary, injury-related work absence, heals with or without permanent damage (e.g. dislocated joint, fractures, vertebral fractures, cerebral injuries, frostbite with amputations) |
4 | Acute mortal danger, polytrauma, immediate prehospital doctor or experienced trauma paramedic attendance if possible, acute surgical intervention, outcome: alive with permanent damage |
5 | Acute mortal danger, polytrauma, immediate prehospital doctor or experienced trauma paramedic attendance if possible, acute surgical intervention, outcome: death |
6 | Immediate death |
10.4.1 Fatalities
While some forms of rock climbing, such as solo climbing or alpine traditional climbing and clean climbing, show a larger injury risk, indoor and bolted sport climbing proved to be relatively safe [3, 4, 10, 12, 13, 18, 20, 65]. Nevertheless there is still a risk of a fatal injury. Few studies give exact data on a fatality rate, as many are conducted retrospectively. Statistics of the German Alpine Association reported seven deaths in the years 2006 and 2007 [91]. These statistics do not differentiate between traditional, ice and sport climbing. A retrospectively conducted study on mountaineering overall calculated an incidence of 0.13 fatalities per 1000 h [63]. For alpine climbing (traditional climbing), a death rate (fatality rate) was documented by Bowie [28] – 13 from 220 injured climbers died – a case fatality rate of 6 %. As most of analyses done in these climbing injury studies were conducted retrospectively through questionnaires, the fatality rate is frequently biased. The “older” studies (20 years ago) [28, 63, 64] reported the most severe injuries and the highest fatality rates, while recently a prospectively conducted study on bouldering [12] reported no fatalities.
The general death numbers in ice climbing can be analysed through the injury and fatality reports of the various Alpine clubs [31]. The Canadian [92] and the American Alpine Club [93] have statistically recorded and analysed all mountain accidents since 1951. In the USA, up to the year 2005, there were 6111 accidents with a total of 1373 (12 %) fatalities [93]. Two hundred fifty-four (4 %) of the accidents happened in ice, though no further evaluation of the ice-climbing injuries was given. Nevertheless if 4 % of all injuries are to be accounted to ice climbing, also 4 % of the deaths can be assumed to be related to ice climbing. This would calculate to 55 fatal ice-climbing injuries in 54 years, in average one ice-climbing fatality per year within the USA. The numbers for Canada are similar [92]. Over 30 years, 92 mountaineers were injured while ice climbing, 30 fatally. Overall the major ice-climbing countries, Switzerland and Canada, report about one death per year [92, 94]; nevertheless these numbers were rising in recent winters [31]. This is probably due to the fact that ice climbing itself became much more popular. For further understanding the UIAA MedCom also published a fatality risk classification [87] (Table 10.2).
Class | Description |
|---|---|
I | Fatalities are technically possible, but very rare. No objective danger, e.g. indoor climbing |
II | Few objective dangers, fatalities rare, falls are not very dangerous, risk is mostly calculable – e.g. sport climbing, low elevation and technically easy peaks |
III | High objective danger, risk is difficult to calculate, falls lead frequently to injuries, fatalities more frequent – e.g. traditional climbing, high Himalayan (7000–8000 m) or difficult peaks |
IV | Extremely dangerous, falls have a high fatality rate, totally unjustified to normal mortals |
10.5 Overstrain Injuries
Chronic overuse injuries occur most often on the upper extremities at the elbow and the fingers [15, 76, 79]. As hand and finger injuries are the most common injuries [1, 29, 60, 95], many studies focus on these anatomical regions [16, 29, 57–60, 69, 76, 95–99]. Schöffl et al. [51, 76] found over 10 years the most common climbing injury being the closed pulley rupture and the most common overuse injury the tenosynovitis of the finger flexor tendons. These pulley injuries are almost rock climbing-specific pathologies and matter of extensive research [60, 80–85]. Other finger injuries which are climbing specific are the “lumbrical shift syndrome” [100], “extensor hood syndrome” [101], “epiphyseal fractures” [75], “FLIP-syndrome” [102], “finger amputations – rope tangling injuries” [57], M. Dupuytren in young age [103] and osteoarthritis of the fingers [58, 104, 105]. In recent publications back problems (“climbers back” [106]) and shoulder pathologies (SLAP and biceps tendon tears [56, 107, 108]) as well as feet deformations were evolving [5, 109–111].
In ice climbing overstrain injuries are rare and hard to distinguish from other climbing training in its origin, as few climbers only practise ice climbing [31].
10.6 Diagnosis and Therapy of the Most Important Conditions
10.6.1 Pulley Injuries
Injuries to the finger flexor pulley system are the most common finger injuries in rock climbers [60]. The pulley system of the second to fifth finger consists of five annular (A1-5) and three cross (C1-3) ligaments (pulleys). Caused mainly through the crimping position, the A2, A3 or A4 pulleys, which are considered the most important ones, can either be strained or ruptured. The most frequently injured pulley is the A2 pulley.
Mostly the climber reports of an acute onset of pain while crimping on a small edge [30]. Sometimes a loud “snapping” sound can be heard. The climber complains about palmar-sided pain at the level of the injured pulley, pressure tenderness, swelling and rarely haematoma. The pain can extend into the palm or the forearm. After clinical suspicion and exclusion of a fracture via radiograph, ultrasound examination leads to its detection. If multiple pulleys are ruptured, a clinical “bowstring” becomes visible. With the ultrasound an enhanced distance of the flexor tendons to the phalanx (tp) can be observed. If the ultrasound fails to give an exact diagnosis, an MRI should be performed. Based on a grading system and an algorithm proposed by Schöffl et al. [60], single ruptures receive a conservative and multiple ruptures a surgical therapy. Biomechanical analyses and strength measurements after conservative pulley ruptures of single pulley injuries proved no strength deficit of the injured finger, and the climbers gained their original climbing level back after 1 year. The outcome after surgical repair of multiple pulley injuries is also good, with mostly a full regain of climbing ability. Nevertheless often a minor restricted range of motion is persisting [112]. After pulley injury a protective taping with the biomechanical developed H-tape is recommended [30, 113] (Table 10.3, Fig. 10.8).
Grade I | Grade II | Grade III | Grade IV | |
|---|---|---|---|---|
Injury | Pulley strain | Complete rupture of A4 or partly rupture of A2 or A3 | Complete rupture of A2 or A3 | Multiple ruptures, as A2/A3, A2/A3/A4 or single rupture (A2 or A3) combined with mm. lumbricalis or ligamental trauma
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





