24
Rheumatic Disorders
1. Identify causes of arthritis.
2. Discuss different types of arthritis.
3. Discuss similarities and differences for osteoarthritis and rheumatoid arthritis.
4. Discuss the effects and benefits of exercise with arthritis.
5. Discuss common methods of management and rehabilitation of arthritic conditions.
6. Discuss principles of joint protection.
7. Discuss general pharmacologic interventions for arthritic conditions.
8. Discuss the different surgical options for arthritic conditions.
9. Discuss pathophysiology and management of rheumatic disorders.
Arthritis affects the lives of 37 million Americans, and it is the leading cause of disability in American adults. The Centers for Disease Control and Prevention (CDC) estimate that by the year 2020 nearly 60 million people will be affected by rheumatic disease, a blanket term covering the more than 100 different conditions that may cause pain, stiffness, and sometimes swelling in or around joints.2,15 Individuals affected with arthritis can suffer from pain, joint stiffness, swelling, and overall decrease in functional ability.23 The causes of arthritis are not fully understood, but there are certain characteristics that can predispose an individual to developing arthritis, include obesity, inactivity, age, and gender.15,23 Though the prevalence of arthritis increases with age, it is more commonly found in women than in men.15,23
ARTHRITIS
Osteoarthritis
Osteoarthritis (OA) is the most common form of arthritis and generally the most painful and disabling joint disorder.2,15,19,26 There is no single cause of osteoarthritis; however, it may be a combination of biomechanical, metabolic, and genetic factors.24,26 Prevalence of OA has been shown to increase with age and is more common in women older than 45 years of age. Risk factors associated with OA include obesity, trauma, infection, and repeated joint overuse.2,15,19,26
OA primarily affects the articular cartilage (which is composed of type II collagen, chondrocytes, and proteoglycans) that surrounds the subchondral bone (Fig. 24-1).2,24 Patients with OA have decreased synthesis and increased catabolism of the cartilage matrix. OA initially damages the cartilage, causing it to become thinner and thereby decreasing proteoglycan synthesis. Initially chondrocytes can maintain the cartilaginous matrix (which consists of proteoglycans and collagen), but after time focal synovial membrane inflammation develops, releasing cytokines, which increase the release of metalloproteinases.2 Metalloproteinase further breaks down cartilage collagen and proteoglycans.2,15 Generally OA is not considered to have any inflammatory response, but new research shows signs of inflammation can exist.2,15
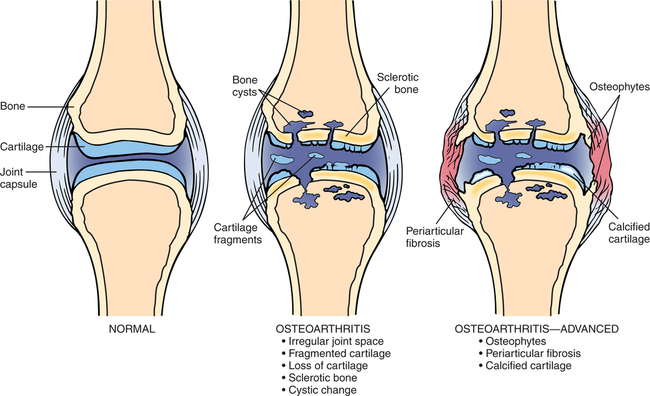
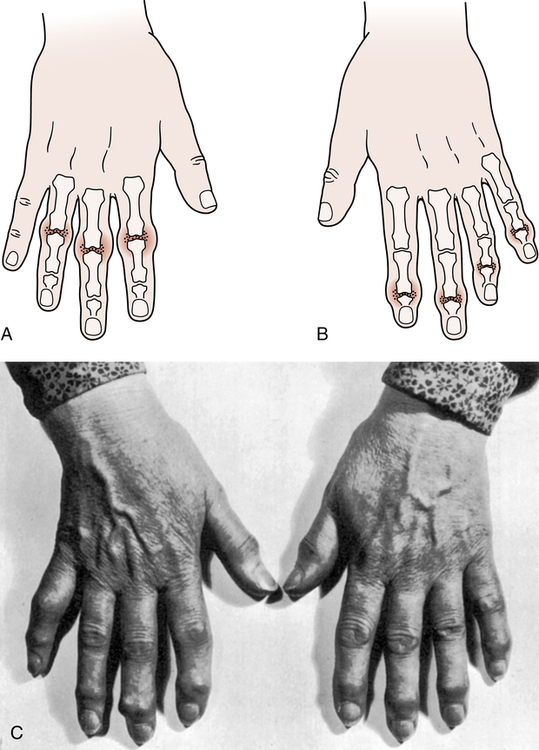
Osteoarthritis most commonly effects weight-bearing joints, such as the knee, hip, or spine.2,15,23,24 Joints in the hands can also be affected: the first carpometacarpal joint, distal and proximal interphalangeal joints (DIP and PIP joints, respectively), and the first metatarsophalangeal joint are other common sites for OA.24 In patients with OA of the hands, Bouchard and Heberden nodes, bony overgrowths at the PIP joints and the DIP joints, are often present (Fig. 24-2).19,24,27 Pain associated with OA usually occurs with activity and is relieved with rest.19,24 Other signs of OA include morning stiffness lasting 20 to 30 minutes, joint locking, a gel sensation in the joint, a bony appearance of the joint, crepitus, and effusion.19,24 Radiographic imaging can show a progression of subchondral bone sclerosis and cysts, osteophytes, and joint space narrowing.13,24 Carpal tunnel syndrome can even be caused by both osteoarthritis and rheumatoid arthritis (RA).27
Management of Osteoarthritis
Although there is no cure for OA, preventive measures can be taken to slow down the progression of the disease or better manage the symptoms. Obesity places extra stress on joints and is a key risk factor that can be prevented or remedied with proper diet and exercise.19,24 The addition of vitamin D and calcium to a patient’s diet can also reduce the occurrence and progression of OA.19 Muscle weakness and repetitive motions or trauma contribute to the onset of OA.24 Studies also have shown that immobilizing the joint for longer than 30 days can increase the risk of cartilage damage.4 Given the positive and negative effects of changes in behavior it is imperative to educate the patient on joint protection, health behavior changes, and the importance of exercise to the management of arthritis.
Education is the most important component to the management of OA. Patients must be educated on the progression of the disease and management of pain with supportive devices, alteration in activities of daily living (ADLs), or thermal modalities. Exercise and weight control are key components to a patient’s success with OA.2,24
Research has shown that every pound of body weight increases the forces in the knee by 2 to 3 pounds during single leg stance.38 Exercise, specifically flexibility, and strength training, has been shown to decrease pain and improve function in individuals with OA.24 Maintaining flexibility is an important first step because it helps decrease stiffness and allows for more comfortable movement.2 Slow progression of the exercise program is important so as to not exacerbate symptoms. Patients should be progressed to 15 minutes of stretching without an increase in symptoms before initiating strength training.2,24 Strength training improves the ability to absorb shock, support joints, and protect from injury.2,26 When choosing an appropriate exercise it is important to keep in mind how much stress in being placed on the joint. Closed-chain weight-bearing exercises can create shear and compressive forces across the lower extremity joints and may be a contraindication pending severity of OA. Open-chain exercises, therefore, are encouraged in patients with OA.
Rheumatoid Arthritis
Rheumatoid arthritis is the second most common form of arthritis, and while it can be equally disabling as OA, it can also lead to increased mortality. This increased mortality has been shown in some research to have systemic causes.12 The progression of RA also leads to difficulty with ADLs and disability. Along with most arthritic conditions, RA affects women more commonly than men and occurs at 20 to 40 years of age.2,14,19 Both genetic and environmental factors have been linked as causes of RA.14,19
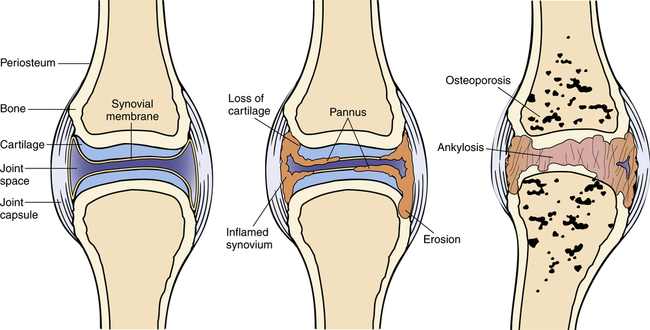
Although the exact etiology of RA is unknown, it is believed to start with a viral or bacterial infection that triggers an autoimmune response.2,14 The immune response causes the body to attack its own tissue, leading to breakdown of joints.2,14 RA affects the synovium lining, which then expands, damaging the extracellular matrix, cartilage, and bone.2,14,26 This autoimmune response also activates T cells, which secrete cytokines, causing expansion of the synovial layer. Cytokines increase activation of fibroblast-like cells and macrophages leading to breakdown of cartilage and bone (Fig. 24-3).2,14
Early signs and symptoms associated with RA include fatigue, weight loss, fever, and musculoskeletal pain. Later signs or symptoms include pain, tenderness, swelling, redness, and stiffness in specific joints.2,7,14,19 Unlike OA, RA morning stiffness can last hours and even all day. Fatigue in patients with RA may cause the patient to need to rest through the day.2 Extraarticular manifestations can affect the lungs, heart, blood vessels, eyes, skin, and other organs.2,7,19 It is important for the physical therapist assistant (PTA) to be able to distinguish the main differences between OA and RA (Table 24-1).
Table 24-1
Differential Diagnosis between Rheumatoid Arthritis and Osteoarthritis
| Differential | Rheumatoid Arthritis | Osteoarthritis |
| Joints affected | Any joint | DIP > PIP Spine Hip Knee |
| Age | Any age Most common ages 20-60 years | More common >40 years |
| Gender | More common in women | More common in men <45 years and women >45 years |
| Relative severity | More than OA | Less than RA |
| Disease pathogenesis | Autoimmune: Immune system attacks body | Condition of wear and tear with aging or injury |
| Joint involvement | Symmetric | Asymmetric |
| Joint destruction | Due to inflammation | Due to biomechanical stress |
| Deformities | Swan neck Ulnar deviation Wrist subluxation Boutonniere deformity | Heberden nodes Bouchard nodes |
| Erythrocyte sedimentation rate | Markedly increased | Mild increase |
| Connective tissue flexibility | Increased | Decreased |
| Morning stiffness | >1 hour | <30 minutes |
| Rheumatoid factor | Positive in 70% | Negative |
| Imaging | Juxtaarticular osteoporosis, erosions | Osteophytes Eburnation Reduced joint space |
| Management | Physical therapy/occupational therapy NSAIDs Gold Penicillamine | Paracetamol Weight loss Joint replacement Exercise |
| NSAID response | Usually some relief | Variable relief |
A unique feature of RA is the rheumatoid nodules, which occur on bony prominences, extensor surfaces, or pressure points.2,19 There are several common physical changes that occur36:











Management of Rheumatoid Arthritis
When treating a patient with RA, education and prevention are vital. Some important objectives of physical therapy all have a common theme of prevention: prevent pain, deformities, loss of normal function, and loss of normal social, physical, and work capabilities. An exercise routine should start with stretching and range of motion (ROM) exercises in pain-free ranges,2,14 and patients with RA should be informed not to overstretch an inflamed tissue to avoid any tears. To prevent contractures and muscular atrophy it is crucial to maintain full ROM of joints through a graded exercise routine.14 Muscle conditioning is also a key component of management, and strength can be increased through isometric and dynamic exercise. Application of heat before exercise can result in better performance.19 Generally during an acute exacerbation, isometric exercises are recommended. During subacute and chronic phases patients can implement dynamic exercise. Do note that vigorous activity should be avoided during an exacerbation of symptoms. Any exercise that causes pain longer than 1 hour after exercise should be eliminated.19
The current management approach with medication is to start early with disease-modifying antirheumatic drugs (DMARDs) because they have been shown to slow RA progression. Nonsteroidal antiinflammatory drugs (NSAIDs) are the most commonly used drugs to decrease pain and swelling and increase ROM. Corticosteroids are also used for swelling, pain, and fatigue and tend to decrease symptoms faster. Biological response modifiers block cytokines, therefore decreasing the breakdown of cartilage and bone.14 More in-depth explanation of the pathophysiology of these drugs will be explained later.
Reactive Arthritis
Reactive arthritis, or Reiter syndrome, is most commonly an abrupt onset of arthritis in young men presenting with the triad, conjunctivitis, urethritis, and oligoarticular arthritis.7,18,19 Conjunctivitis is also known as pinkeye, which is inflammation of the conjunctiva (outermost layer of eye and inner surface of eyelid). Urethritis is inflammation of the urethra and presents as painful urination. Oligoarthritis is a form of arthritis with inflammation in two to four joints. Reiter syndrome usually presents within days or weeks of a dysenteric or sexually transmitted infection.18,19 The arthritis is usually asymmetrical and involves the weight-bearing joints, such as the toes, ankles, and knees, then ascends to the axial skeleton and upper extremities.7,18,19 Other symptoms present with Reiter syndrome are oral ulcers, penile lesions, keratoderma blennorrhagicum, and plantar heel pain.7,19 Approximately 80% of individuals with Reiter syndrome are positive for human leukocyte antigen B27 (HLA-B27).7,19 The human leukocyte antigen system is the name of the major histocompatibility complex in humans. The major HLA antigens are essential elements in immune function. Sacroiliitis is observed in about 60% of patients with chronic Reiter syndrome. Management of Reiter syndrome includes NSAIDs and physical therapy similar to that used to treat ankylosing spondylitis.
Psoriatic Arthritis
Psoriatic arthritis is a seronegative inflammatory joint disease affecting a small percentage of people with psoriasis.13,19 Psoriasis is an inherited chronic inflammatory skin disease that is characterized by silvery scales on a bright red plaque (Fig. 24-4).5,13 In most cases the skin disease precedes the arthritis symptoms by several months to years.9 Psoriatic arthritis closely resembles rheumatoid arthritis, but has differences such as DIP involvement, psoriasis or family history, nail pitting, and “sausage” appearance of digits.7,14,19 Gender does not appear to predispose one to psoriatic arthritis, but it generally begins at ages 30 to 50 years.9,13,18 Psoriatic arthritis is usually asymmetric and involves the small joints of hands and feet.7,13,32 However, larger axial joints such as the sacroiliac joint can be affected in later phases of disease. Sacroiliitis usually occurs unilaterally, whereas ankylosing spondylitis is bilateral.13,18 Imaging reveals a “pencil-in-cup” deformity caused by erosion and destruction of the phalanx bones that makes them look like a sharpened pencil at the end of the bone (Fig. 24-5).5,7,32 Furthermore, psoriatic arthritis can cause fingernail thickening, pitting, and separation from the nail bed.9 Finally, periosteal reactions (formation of new bone) can be seen on x-rays.


Management for psoriatic arthritis is similar to that of rheumatoid arthritis.7,18,32 Although there is no cure for psoriatic arthritis, NSAIDs can be used to treat inflammatory symptoms.5,13 Most of the time the disease is mild and not destructive; therefore treatment consists of symptom management.5,13
Juvenile Rheumatoid Arthritis
Many rheumatic diseases in children exist, consisting of both acute and chronic conditions, with juvenile rheumatoid arthritis (JRA) being one of the most common.44 JRA, a chronic inflammatory disease, actually covers three types of childhood arthritis: pauciarticular, polyarticular, and systemic.7,13,32,44 The etiology of JRA is unknown, but is thought to be triggered by environmental factors or infection in children with genetic predisposition.13,44 “JRA is similar to adult RA in the fact that the immune system mistakenly attacks the joints and organs, causing inflammation, destruction, fatigue, and other local and systemic effects.”13 JRA occurs before the age of 16 years and affects girls more commonly.7,13,44 To confirm diagnosis the child must have the arthritis for at least 6 consecutive weeks.44 Other symptoms of JRA are fever, rash, fatigue, anemia, loss of appetite, stiffness, irritability, altered mobility, and change in ADLs.44
Pauciarticular JRA is characterized by asymmetric synovitis of four or less joints.7,13,44 There are usually no systemic features and it most commonly affects the knee, elbow, and ankle (Fig. 24-6).13,44 Two subtypes of pauciarticular JRA exist: early onset and late onset.7,13,44 Early onset pauciarticular JRA occurs before the age of 5 years and usually affects girls. Early onset pauciarticular JRA left untreated can result in iridocyclitis that can lead to visual impairments.7,13,44 The second subtype, late onset pauciarticular JRA, occurs between the ages of 10 and 12 years and is more common in boys. This subtype affects large weight-bearing joints and entheses (insertion point of tendon into bone).44 These children often have spinal involvement that may develop into a spondyloarthropathy.13,44

Polyarticular JRA is synovitis in more than four joints and is more common in girls.7,13,44 It usually manifests with symmetrical involvement of the small joints of the hands or feet, wrists, elbows, shoulders, knees, hips, ankles, cervical spine, and temporomandibular joints.13,44 Bursitis and tendinitis can occur because they too are lined with synovial tissue. Unlike pauciarticular JRA, polyarticular JRA can have systemic features, including low grade fever, anemia, leukocytosis, mild hepatosplenomegaly, and lymphadenopathy.44
The last type of JRA is systemic JRA (Still disease) which can occur at any age and does not favor girls or boys.13,44 Systemic JRA is characterized by a rash, synovitis in one or more joints, and an intermittent high grade fever.7,13,44 The fever usually occurs in the afternoon and evenings and will return to normal with the child feeling better.13,44 Because the fever can precede all other symptoms these children are often initially evaluated for fever of unknown origin.44 The rash usually appears with the fever and is salmon pink, 2 to 5 mm in diameter, and has an erythematous perimeter.44 Other signs and symptoms of systemic JRA include malaise, irritability, anemia, hepatitis, peptic ulcer disease, leukocytosis, thrombocytosis, lymphadenopathy, hepatomegaly, splenomegaly, pericarditis, and pleuritis.13,44
Management of Juvenile Rheumatoid Arthritis
Management for children with JRA is a combination of medication, physical therapy, and occupational therapy. Main objectives of therapy should be to control pain and inflammation, promote mobility, and improve function.13,44 Control of pain and inflammation is usually done with NSAIDs, which have been shown to decrease stiffness, pain, and swelling in children with JRA. Other medications used with JRA are corticosteroids, DMARDs, infliximab, and immunosuppressants.13,44 ROM is the strongest indicator of functional disability in children with systemic JRA.13 Therefore, all joints should be stretched through the full ROM twice a day to maintain good mobility. 44 Heat can be used before stretching to help warm the muscles and decrease pain before stretching. Splinting and serial casting can also be used to help maintain or gain ROM.44 Resistive exercise is also important and has been shown to change the immune response, with lower levels of cytokines and higher levels of antiinflammatory compounds.13 Aquatic therapy is an appropriate management for JRA because the heat can help relax the muscles and decrease pain.44 Even though the patient with JRA is only a child, education in joint protection and energy conservation is still important. Furthermore, always try to make the exercise program fun, interesting, and interactive to keep the child involved.44
Septic Arthritis
Septic arthritis is the invasion of a joint by an infectious agent causing arthritis. Septic arthritis usually occurs from a bacterial infection, but can be viral, mycobacterial, or fungal. Bacteria are introduced into the joint by the bloodstream from an infection elsewhere or from direct penetration after a wound, surgery, or local infection.42 Two common types of septic arthritis are gonococcal and nongonococcal.19,42
Gonococcal Arthritis
Gonococcal arthritis usually occurs in healthy individuals and is two to three times more common in females.19,42 Initially the patient will experience 1 to 4 days of noninflammatory joint pain in the wrist, ankle, knee, and elbow. Chronic arthritis or tendonitis are common symptoms preceding gonococcal arthritis.42 Patients tend to have a characteristic asymptomatic skin lesions with 2 to 10 small necrotic pustules over the extremities, especially the palms and soles.19
Nongonococcal Arthritis
Nongonococcal bacterial infections are primarily monoarticular and in large weight-bearing joints and wrists.19,42 Previous joint damage from a disease like RA or intravenous drug users have increased risk of infection.19,42 Staphylococcus aureus is the most common cause of nongonococcal septic arthritis.19,42 Nongonococcal septic arthritis is marked by a sudden onset of acute arthritis with pain, swelling, and heat in one joint.19 The hip, wrist, shoulder, and ankle can all be affected, but the knee is the most common. Chills and fever often accompany the symptoms of nongonococcal septic arthritis.19
Management of nongonococcal arthritis
Management should be initiated quickly with systemic antibiotics addressing the causative organism. If the specific organism cannot be determined then bacterial antibiotics are recommended.19 Aspiration of the affected joint will keep the joint free of destructive exudates.19,42 Early intervention is important because ankylosis and articular damage can occur if management is delayed. Immobilization and heat can help decrease the joint pain.19 Rest, elevation, and immobilization are used during the acute phase of the disease.
As stated before, early diagnosis and management are important because of the potential for harm if septic arthritis goes untreated.42 Risk factors to keep in mind are infection elsewhere in the body, very old or young age, presence of other systemic diseases, recent joint aspiration or surgery, prosthetic joints, immunosuppression, and intravenous drug abuse.13,42 An infected joint will be painful, tender, and have limited motion, but may not have redness, heat, and swelling, especially if treatment includes immunosuppressants.42 Finally, remember that prevention is always a key component of physical therapy, so passive and then active ROM should be started as soon as possible to prevent contractures and loss of strength.42









