Chapter 25 Rehabilitation of Medial Ligament Injuries
CLINICAL CONCEPTS
Medial ligament injuries are among the most frequently treated problems of the knee joint. Whereas isolated superficial medial collateral ligament (SMCL) ruptures are common, concomitant damage to the anterior cruciate ligament (ACL) occurs in many cases, especially in young and active patients.1–4,9 The majority of isolated acute injuries that involve damage to the SMCL alone, or to the SMCL and posteromedial capsule (PMC), do not require surgery. Patients who have medial ligament tears classified as first degree (tear involving a few fibers), second degree (partial tear, no instability, ≤3 mm of increased medial joint opening), or third degree (complete rupture) who demonstrate either a mild to moderate increase in medial joint opening at 30° of flexion and no increase at 0° do not require acute medial ligament reconstruction. These knees are treated with the conservative rehabilitation program, and if concomitant injury exists to other ligaments, the decision of whether to reconstruct those structures is based on the extent of the injury, patient goals, and other issues addressed for the ACL in Chapter 7, Anterior Cruciate Ligament Primary and Revision Reconstruction: Diagnosis, Operative Techniques, and Clinical Outcomes, the posterior cruciate ligament (PCL) in Chapter 21, Posterior Cruciate Ligament: Diagnosis, Operative Techniques, and Clinical Outcomes, and the posterolateral ligament structures in Chapter 22, Posterolateral Ligament Injuries: Diagnosis, Operative Techniques, and Clinical Outcomes.
Critical Points CLINICAL CONCEPTS


An acute third-degree injury consisting of gross major disruption of all of the medial structures (SMCL, deep medial collateral ligament, meniscus attachments, PMC, posterior oblique ligament [POL], and semimembranosus attachments), either alone or in combination with cruciate ligament tears, often require surgical intervention. In these knees, large increases in medial joint opening are present at 30° of flexion, and at least 5 mm of increased medial joint opening exists at 0°. In addition, repair of medial meniscus attachments is indicated to retain meniscus function. Chronic deficiency of the medial ligament structures that causes partial giving-way during athletic activities may require reconstruction. In these knees, partial or complete ACL deficiency is frequently noted. The indications for medial ligament surgery and the appropriate candidates are discussed in detail in Chapter 24, Medial and Posteromedial Ligament Injuries: Diagnosis, Operative Techniques, and Clinical Outcomes.
CONSERVATIVE TREATMENT OF MEDIAL LIGAMENT INJURIES
The goals of rehabilitation of medial ligament injuries are to
 Provide appropriate protection initially after the injury to allow the disrupted medial ligament structures to “stick-down” and heal with the least amount of residual ligament elongation or abnormal medial joint opening.
Provide appropriate protection initially after the injury to allow the disrupted medial ligament structures to “stick-down” and heal with the least amount of residual ligament elongation or abnormal medial joint opening.





The treatment rationale for patients with acute medial ligament ruptures is shown in Figure 25-1. The algorithm is divided into three major sections based on the extent of injury to the SMCL and PMC/POL. The first- and second-degree injuries are treated initially with a functional brace, weight-bearing as tolerated, and the rehabilitation program summarized in Tables 25-1 and 25-2. Some second-degree injuries may have considerable medial pain and swelling, and in these cases, an extension brace and assistive ambulatory devices are used for the initial 1 to 2 weeks after the injury. The type of functional brace varies from a medial/lateral hinge elastic type to a long-leg postoperative brace in select cases in which more support is required.
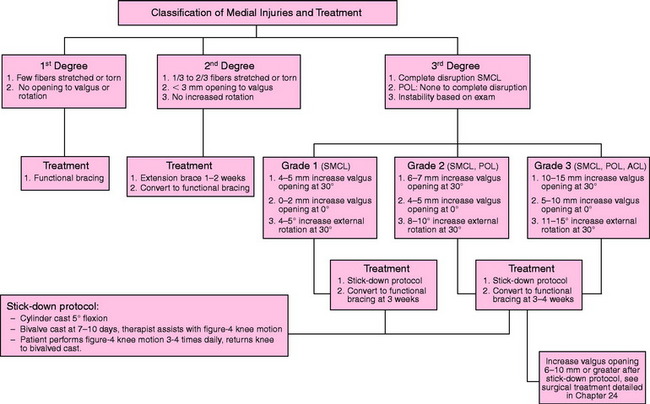
Table 25-1 Conservative Management of First-Degree Medial Ligament Injuries
ROM, range of motion.
Table 25-2 Conservative Management of Second-Degree Medial Ligament Injuries
• Progress to agility, proprioceptive, neuromuscular, sports-specific activities upon resumption of full weight-bearing as tolerated. |
ROM, range of motion.
Third-Degree Injuries: Weeks 1 to 3
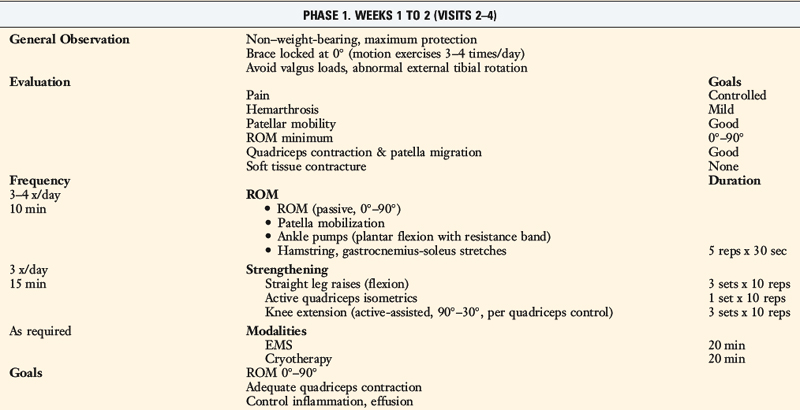
At 7 to 10 days, the cylinder cast is split into an anterior and a posterior shell (Fig. 25-2) to permit the patient to begin passive range of motion (ROM) exercises, which are initially assisted by the therapist. The cast is used for an additional 2 weeks to allow for early stick-down of the medial ligament structures. The patient is allowed to bear 25% of her or his body weight as long as the cast is in place. ROM exercises are initiated in a figure-four position from 0° to 90° in order to avoid valgus and external rotation loads on the healing ligaments (Fig. 25-3). A 4-inch tubular stocking is double-wrapped around the foot and ankle to allow the patient under her or his own power to flex the knee. This protected ROM program is performed three to four times a day for 10 to 15 minutes per session. Quadriceps strengthening exercises including isometrics and flexion straight leg raises are emphasized. TheraBand resistance for plantar flexion is used to maintain gastrocnemius tone. Ice, compression, and elevation are used for pain and swelling control.


Critical Points CONSERVATIVE TREATMENT OF MEDIAL LIGAMENT INJURIES















Third-Degree Injuries: Weeks 4 to 6
Emphasis during this time period focuses on ligament protection during gait and exercise. The progression of exercise allows knee motion to be restored within normal limits. Muscle strengthening includes both closed-chain and table exercises (straight leg raises). Emphasis is placed on hip and core control plus progression of quadriceps strengthening (Table 25-3).
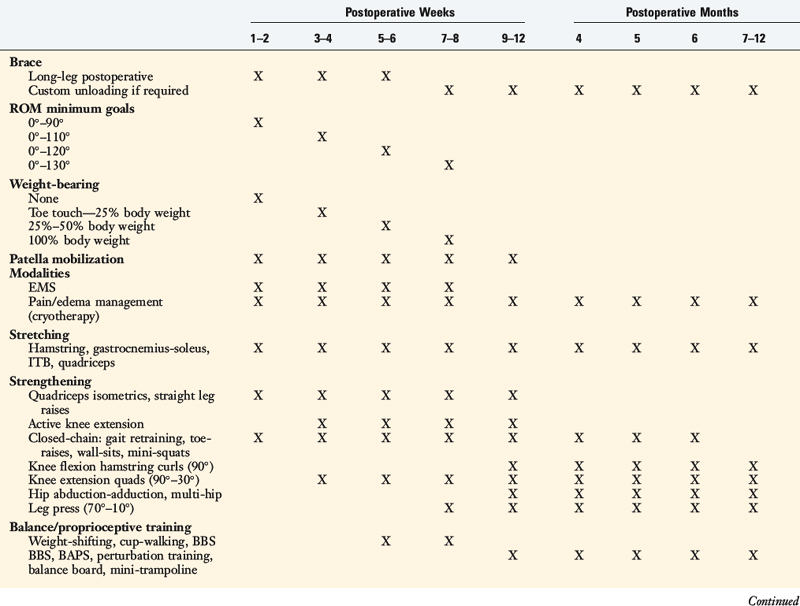
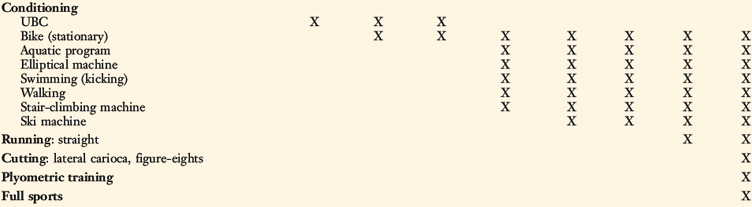
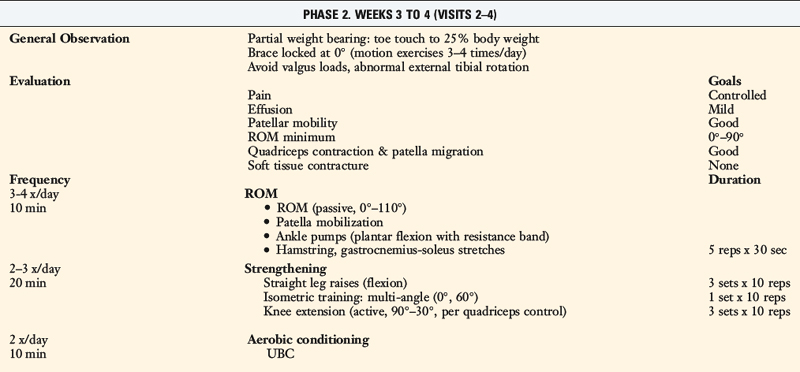
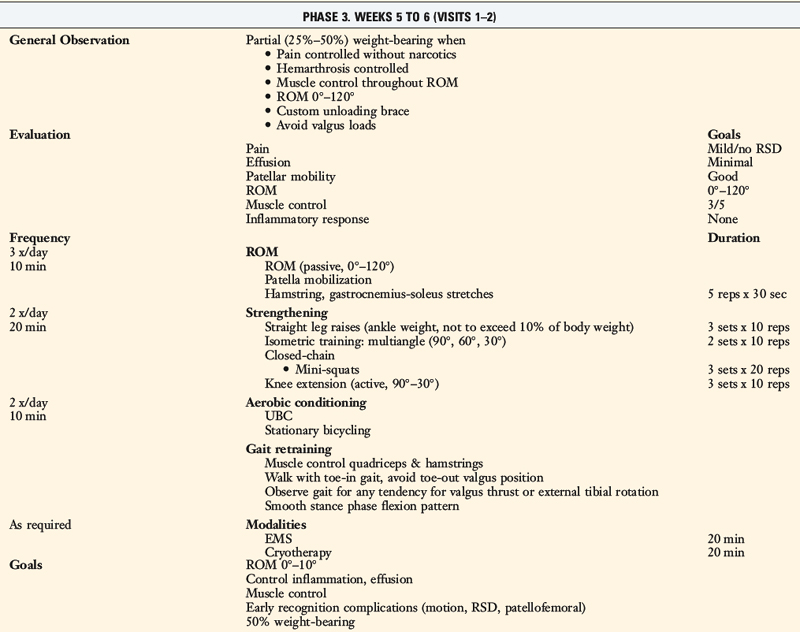
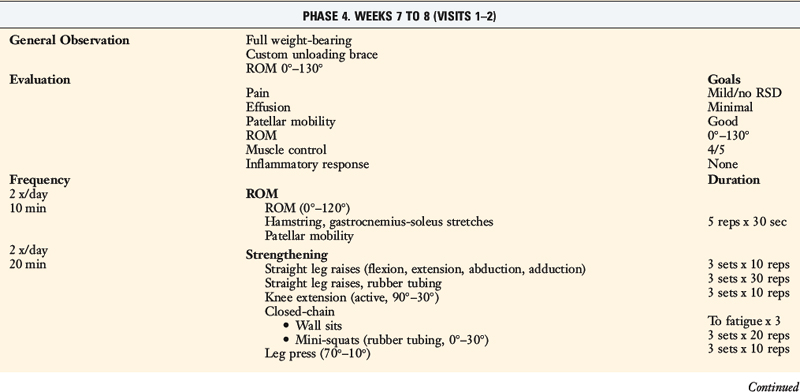
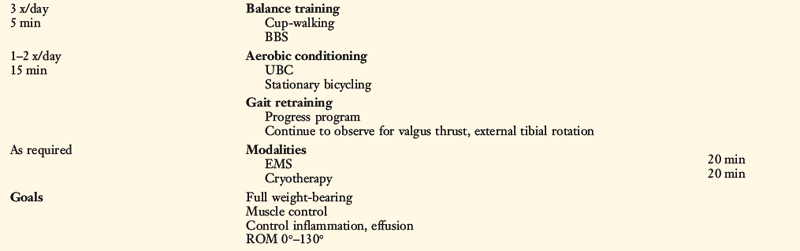
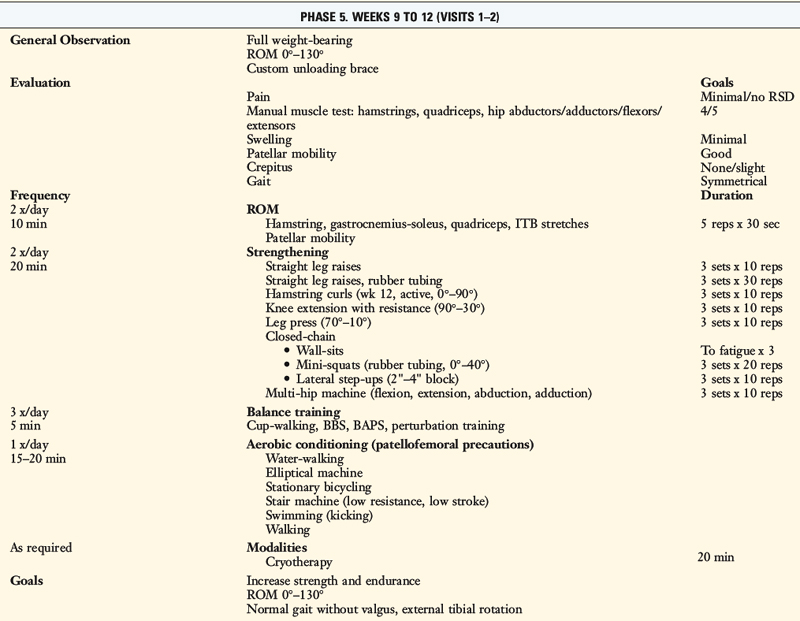
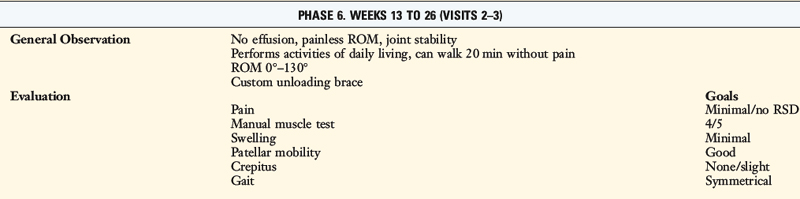
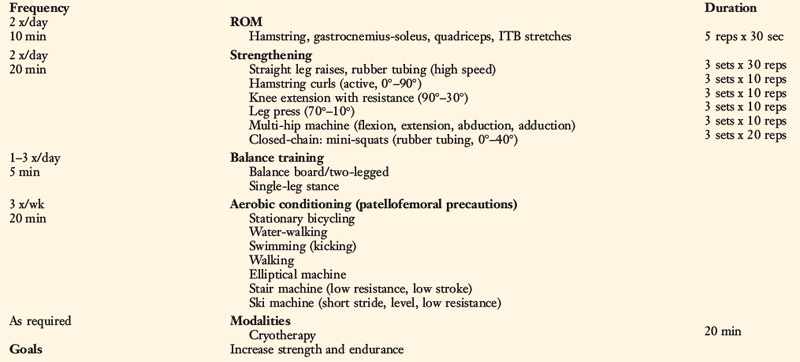
Table 25-3 Cincinnati Sportsmedicine and Orthopaedic Center Rehabilitation Protocol for Medial Ligament Repair or Reconstruction

Related posts:
 Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
Aquatic Therapy for the Arthritic Knee
The Cincinnati Knee Rating System
Medial and Posteromedial Ligament Injuries: Diagnosis, Operative Techniques, and Clinical Outcomes
Primary, Double, and Triple Varus Knee Syndromes: Diagnosis, Osteotomy Techniques, and Clinical Outcomes
Allografts: Graft Sterilization and Tissue Banking Safety Issues
Differences in Neuromuscular Characteristics between Male and Female Athletes
Aquatic Therapy for the Arthritic Knee
The Cincinnati Knee Rating System
Medial and Posteromedial Ligament Injuries: Diagnosis, Operative Techniques, and Clinical Outcomes
Primary, Double, and Triple Varus Knee Syndromes: Diagnosis, Osteotomy Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


