Radial Longitudinal Deficiency
CASE PRESENTATION
A 3-month-old female infant presents with bilateral radial longitudinal deficiency (Figure 13-1). She has absent thumbs with a simple skin tag on the left and complete aplasia on the right. Both upper limbs are foreshortened, the left more so than the right. There are no associated malformations. Her father has less severe bilateral wrist and thumb involvement, treated surgically as a preschool and adolescent child.
CLINICAL QUESTIONS
What is the incidence of radial longitudinal deficiency?
What syndromes and malformations are associated with radial deficiency?
How is radial deficiency classified?
What is the initial treatment?
What are the surgical options?
How does one choose the appropriate treatment for the patient?
What are the long-term results?
THE FUNDAMENTALS
A stable wrist is necessary for power grip. Normal digital motion and strength are necessary for sophisticated pinch function. Normal elbow motion is necessary for full hand-to-mouth and hand-to-groin activities. Normal limb length allows for full placement of the hand in space. Children with severe radial deficiency are lacking in all these areas. If bilateral, activities of daily living are compromised and require marked adaptive behavior. As Flatt pointed out, “Radial club hand … is a profoundly abnormal hand joined to a poor limb by a bad wrist.”1
When you add in the significant aesthetic differences from unaffected limbs and hands, severe radial deficiency tests the resiliency of the human mind and spirit.
Etiology and Epidemiology
Also known as radial club hand or radial dysplasia, radial longitudinal deficiency occurs in approximately 1:30,000 live births.2 It is associated with many other malformations as the timing of in utero preaxial upper limb development coincides with cardiac, hematopoietic, musculoskeletal, renal, gastrointestinal, and craniofacial, among others, organ system development.
These associated conditions include VACTERRL (V = vertebral, A = anal atresis, C = cardiac, TE = tracheoesophageal fistula, R = renal, radial, L = limb), Fanconi anemia, thrombocytopenia absent radius (TAR), chromosomal abnormalities (trisomy 13, 18), and craniofacial syndromes such as Nager acrofacial dysostosis. Some of these conditions are genetic. Fanconi anemia (1:350,000 live births, but genetic carriers may be 1:600) and TAR (1:240,000 live births) are autosomal recessive, and Holt-Oram (cardiac septal defects and radial deficiency) is autosomal dominant. Mutations in the TBX5 gene have been identified as the causal factor for Holt-Oram syndrome. Most are sporadic including all the VACTERRL-syndrome children.
Clinical Evaluation
Any infant with a radial longitudinal deficiency needs a thorough physical exam, laboratory screening, and radiologic evaluation. Subspecialty consultation with genetics, cardiology, orthopaedics, hematology, general surgery, and craniofacial surgery may be necessary. There are now times where the diagnosis is made during pregnancy3 (Figure 13-2), and initial consultations occur prenatally rather than in the neonate. A thorough physical exam in the nursery is performed looking for a cardiac murmur, obvious scoliosis, lower limb deficiencies, and breathing or feeding issues indicative of a tracheoesophageal fistula. A complete blood count to assess for thrombocytopenia or pancytopenia is obtained. With TAR, the platelet count is at its lowest in the neonate, usually <100,000 (normal range 150,000 to 300,000) at birth, and improves over the first year of life. The risk for these children is hemorrhage. Fanconi anemia and pancytopenia usually do not present
until preschool or school age. Therefore specific testing for chromosomal fragility and breakage needs to occur in infancy. The testing is done with either diepoxybutane or mitomycin C. These tests can also be performed prenatally with chorionic villi or amniotic fluid cells. Fanconi anemia is a potentially lethal disease if recognized late and may be curable with bone marrow transplantation if performed early before pancytopenia, myelodysplasia, or acute myelogenous leukemia develops. This is one of the few situations where a pediatric hand surgeon can save a life with proper referral and testing. Renal and cardiac ultrasounds are generally performed for identifying malformations. A chest x-ray as a part of cardiac workup will also provide a screening test for congenital scoliosis or other vertebral abnormalities.
until preschool or school age. Therefore specific testing for chromosomal fragility and breakage needs to occur in infancy. The testing is done with either diepoxybutane or mitomycin C. These tests can also be performed prenatally with chorionic villi or amniotic fluid cells. Fanconi anemia is a potentially lethal disease if recognized late and may be curable with bone marrow transplantation if performed early before pancytopenia, myelodysplasia, or acute myelogenous leukemia develops. This is one of the few situations where a pediatric hand surgeon can save a life with proper referral and testing. Renal and cardiac ultrasounds are generally performed for identifying malformations. A chest x-ray as a part of cardiac workup will also provide a screening test for congenital scoliosis or other vertebral abnormalities.
 FIGURE 13-1 Clinical photograph of radial longitudinal deficiency with a rudimentary pouce flottant. |
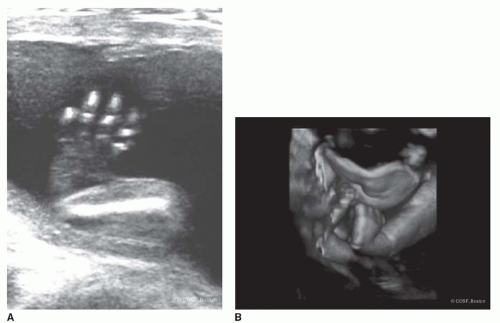 FIGURE 13-2 A: Prenatal ultrasound of severe radial longitudinal deficiency. B: A 3-D ultrasound of same patient. Clinical photograph of same patient shortly after birth is seen in Figure 13-1. |
Evaluation of the radial deficiency starts at the chest wall and shoulder. Entire upper limb involvement does occur with both obvious and subtle differences.
Phocomelia with preaxial deficiency is the most involved case. Elbow range of motion is critical to treatment decisions. In the presence of a stiff extended elbow, extreme wrist radial deviation functionally substitutes for elbow flexion. In the absence of at least 90 degrees of elbow flexion, definitive correction of the wrist deformity is contraindicated.
The obvious deficiencies are in the wrist and hand. This condition can have profound limitations of (1) forearm length, (2) wrist stability and motion, (3) thumb development and function, and (4) digital motion and strength. Anatomic variations abound, and the degree of soft tissue anatomic abnormalities tends to parallel the degree of osseous deficiency. Muscle deficiencies throughout the entire upper limb, but in particular in the forearm, wrist, and hand, include partial or complete absence, hypoplasia, abnormal origins and/or insertions, and/or fusion to adjacent muscles and accessory muscles. Brachial plexus, radial, ulnar, and median nerve anomalies have been well described.4 The median nerve is usually present
but with aberrant anatomic course through the forearm and wrist. Vascular anomalies also are frequently present, and, again, the more deficient the radius, the more likely an abnormal radial artery and palmar arch.5 The spectrum of thumb deficiency ranges from mild hypoplasia to complete absence (Blauth classification). Digital involvement spreads from the radial side to the middle of the hand depending on the degree of preaxial osseous and muscle deficiency. Digital lack of motion is common and greatly affects function. The ulnar digits tend to have more developed joints, as well as intrinsic and extrinsic muscles, than the middle or radial side of the hand. Ulnar prehension is common. Very few of the more involved children can perform power grip and normal pinch activities. Spherical grip is most often used for functional grasp. The hand tends to be assistive rather than independent. Since 50% to 60% have bilateral involvement, this can be debilitating.
but with aberrant anatomic course through the forearm and wrist. Vascular anomalies also are frequently present, and, again, the more deficient the radius, the more likely an abnormal radial artery and palmar arch.5 The spectrum of thumb deficiency ranges from mild hypoplasia to complete absence (Blauth classification). Digital involvement spreads from the radial side to the middle of the hand depending on the degree of preaxial osseous and muscle deficiency. Digital lack of motion is common and greatly affects function. The ulnar digits tend to have more developed joints, as well as intrinsic and extrinsic muscles, than the middle or radial side of the hand. Ulnar prehension is common. Very few of the more involved children can perform power grip and normal pinch activities. Spherical grip is most often used for functional grasp. The hand tends to be assistive rather than independent. Since 50% to 60% have bilateral involvement, this can be debilitating.
Osseous classification is by the amount of preaxial deficiency. Bayne and Klug classified this by types I through IV, from a minor deficiency in length to complete absence (I = short distal radius, II = hypoplastic radius, III = partial absence radius, IV = complete absence radius). James et al. added type O for radial carpal and thumb deficiency with a normal radius. We use a type V for elbow involvement and phocomelia. Unfortunately, type IV is the most common type, meaning those with this deformity have a lot of involvement. The osseous classification can be misleading because it focuses only on the radius and precludes thinking of the ulna, muscle, and soft tissue involvement. In types III and IV, the ulna is always foreshortened (at best 60% of normal length) and frequently bowed. The osseous classification can lead us to think simplistically. “If I only straighten the forearm, wrist, and hand, all will be well,” forgetting the profound degree of muscle and soft tissue impairment.
Treatment
Experience is that marvelous thing that enables you to recognize a mistake when you make it again.
—Franklin P. Jones
In all of congenital hand surgery care, at the present time there may be no greater variation and polarity of opinion than care of the severe radial club hand. A generation back, it appeared to be quite straightforward. Stretch the soft tissues with splints and/or casts early in infancy, surgically place the hand on the end of the ulna, and reconstruct the thumb. All in sequence during the first 1 to 2 years of life. Done deal. Unfortunately, as our partner Dr. John Emans says, “There is nothing that shakes your confidence as much as surgical follow-up.” Nowadays, there are the nihilists who almost believe in virtually no surgical intervention for type IV radial club hand and the optimists who believe that you use everything you have in your toolbox, including external fixation, lengthening, as well as microvascular bone and joint transfers. For the neophyte, even for the experienced surgeon, and especially for the parents, treatment selection can be confusing and daunting. The range of strong opinions makes for interesting debate but hard choices.
Nonsurgical
It is clear that the place to begin treatment is with stretching of the wrist from its malaligned position of radial deviation and flexion into extension and neutral to ulnar deviation. This can be by serial casting or by passive stretching many times a day and progressive forearm-based splinting of the wrist into a corrected position (Figure 13-3). With our skilled therapists, we tend to use progressive splinting and stretching followed by maintenance nighttime splinting in the first 6 to 12 months of life. For the mild type I or II radial deficiency, this is all the care that is needed for the wrist and forearm in infancy. They will correct and usually maintain their alignment throughout growth. If there is recurrent deformity, reinitiation of splinting and stretching is begun.
If the elbow is stiff in extension, a corrected wrist may impair hand-to-mouth, hand-to-head, and bimanual hand activities. Thus, most surgeons state that lack of elbow flexion is a contraindication to wrist surgery in radial longitudinal deficiency. We concur with that opinion.
Surgical Indications
Surgical intervention for radial club hand is for persistent wrist deformity that limits function. There is also the unspoken motivation to improve aesthetics. A welldesigned and executed surgical plan will address the deficiencies in (1) wrist stability, (2) wrist alignment, and (3) forearm length. These often are not achievable in a single-stage procedure. Surgery does not come without a cost. For example, creating a straight, stable wrist may come at the cost of future growth of the ulna or wrist mobility and function. The more you strive to maintain or improve wrist motion, the more risk there is of recurrence. Ultimately, the functional outcome of any radial dysplasia patient, regardless of treatment, will be determined more by the quality of the fingers and thumb than the position and stability of the wrist.
Most of the time with more marked deformity, the stretching and splinting/casting precedes open or external fixation definitive surgical correction. The more difficult decision is what to do with a wrist, usually a Bayne type III or more commonly type IV deformity, that is uncorrectable by therapy, casting, and/or splinting. If it is extreme, most surgeons now progress to external fixation for soft tissue stretching and joint alignment.6,




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
