Proximal Procedures of the First Ray
PART 1 Osteotomies of the First Metatarsal Base
Robb A. Mothershed
Metatarsus primus adductus, or an increase of the first intermetatarsal angle, has long been recognized as a major contributing factor in the deformity of hallux abducto valgus. This component of hallux abducto valgus has been addressed by proximal osteotomies for decades. A transverse plane osteotomy of the first metatarsal base for the repair of hallux abducto valgus deformity was first described in 1901 by Loison (1), and it was performed in 1903 by Balacescu (2). However, not until the late 1960s and early 1970s did the base wedge osteotomy became popular and widely used. Over the intervening years, this particular procedure has been performed with less frequency because of several factors. First, certain complications were believed to be inherent to the procedure, including first metatarsal elevatus, shortening of the metatarsal, failure of the fixation, and delayed union (3, 4, 5, 6, 7). However, surgeons subsequently began to appreciate that most of these problems resulted from surgical technique, inadequate fixation, and insufficient postoperative protection, as opposed to a deficiency of the procedure itself. The perceived complications associated with the closing base wedge osteotomy also led surgeons to consider other forms of proximal osteotomies such as the crescentic and chevron configurations. In addition, other surgeons have employed more distal procedures for the correction of hallux abducto valgus deformity such as the Austin or Scarf osteotomies whenever possible. These latter procedures may prove technically easier to perform, and the patient can remain weight bearing during the postoperative period. However, the proximal osteotomies still are effective, particularly in patients with severe deformities and in patients with high intermetatarsal angles. The technical advances in surgical technique, rigid internal fixation, and the institution of a non-weight-bearing interval in the postoperative recovery have demonstrated that these procedures can provide consistently good results.
INDICATIONS
Large Intermetatarsal Angles
The traditional indication for a transverse plane base osteotomy of the first metatarsal was a hallux abducto valgus deformity with a high intermetatarsal angle, typically exceeding 15 degrees. This is still a reasonable criterion for employing this type of procedure, although in some instances adequate correction of severe deformities can be accomplished with other approaches as well.
The base wedge procedure may be more effective in reducing a high intermetatarsal angle than a distal procedure, particularly in rigid deformities, because of the geometric principles of placement of the osteotomy (8). The oblique orientation of the base wedge osteotomy is angled from proximal-medial to distal-lateral. This design allows the axis and hinge of the osteotomy to be placed in close proximity to the base of the first metatarsal. The effect creates the longest distance possible between the hinge and the distal end of the bone while keeping the osteotomy within the first metatarsal. This distance is the radius arm. A longer radius arm creates greater lateral movement at the end of the arm for each degree of rotation around the arc of the circle. Therefore, the base wedge osteotomy allows greater lateral movement of the head of the metatarsal for every degree of wedge resected and thereby provides a more effective procedure.
In addition, the more proximal the apex of the osteotomy,
the more lateral is the axis of rotation in relation to the position of the second metatarsal. Therefore, a more proximal hinge provides a more lateral overall position of the first metatarsal head once the distal segment has been reduced into a parallel relationship with the second metatarsal. In effect, the more proximal hinge allows the first metatarsal head to come closer to the second metatarsal without creating a negative intermetatarsal angle in the distal segment of the bone (8).
the more lateral is the axis of rotation in relation to the position of the second metatarsal. Therefore, a more proximal hinge provides a more lateral overall position of the first metatarsal head once the distal segment has been reduced into a parallel relationship with the second metatarsal. In effect, the more proximal hinge allows the first metatarsal head to come closer to the second metatarsal without creating a negative intermetatarsal angle in the distal segment of the bone (8).
The crescentic osteotomy also offers a more proximal location for rotation of the metatarsal. Although the proximal chevron procedure is typically transposed, it may also be rotated to enhance the reduction of the intermetatarsal angle. In each instance, more effective correction of large intermetatarsal angles may be obtained as compared with distal osteotomies.
Rigid First Ray
Flexibility of the first ray is an important factor to consider when evaluating the patient with hallux abducto valgus deformity. The success of a distal metatarsal osteotomy in the repair of hallux abducto valgus deformity associated with high intermetatarsal angles requires good transverse plane flexibility. This feature may be evaluated preoperatively by assessing the sagittal plane mobility of the first ray. If the first ray demonstrates good mobility in the sagittal plane, then it will almost always have good mobility in the transverse plane as well. In addition, one may assess the flexibility by applying medial to lateral compression to the first metatarsal head. However, if the sesamoids are significantly displaced within the first intermetatarsal space, then lateral shift of the metatarsal head may be difficult to accomplish.
 FIG. 1. A: Preoperative radiograph of a patient with severe hallux abducto valgus and a rigid first ray secondary to the articular relationship of the first and second metatarsal bases. B: Postoperative appearance 15 months after a closing base wedge osteotomy and fibular sesamoidectomy. |
Radiographic evaluation may also render helpful information. Some patients may actually have an enlarged articular facet between the metatarsal bases and a rudimentary os intermetatarsia, both of which are typically associated with less mobility of the first ray (Fig. 1). When distal osteotomies are employed for the correction of greater degrees of hallux abducto valgus deformity, the correction is accomplished by a combination of the release of soft tissue tension about the first metatarsal phalangeal joint and the translocation of the metatarsal head. If a distal osteotomy is performed in a rigid deformity, then the release of the soft tissues at the first metatarsophalangeal joint will generally result in little if any ability to reduce the intermetatarsal splay significantly. As such, it becomes more difficult to achieve a desirable permanent correction with a distal procedure. Therefore, a proximal osteotomy may be appropriate for correction of the hallux abducto valgus deformity in patients with reduced mobility of the first ray with only moderate amounts of intermetatarsal splay.
Sagittal Plane Abnormalities of the First Ray
Proximal osteotomies may also be helpful in addressing significant sagittal plane deformity or disease in patients with hallux abducto valgus deformity. The presence of a callus or pain plantar to the second metatarsal head generally indicates a hypermobile first ray, and patients may benefit from simultaneous plantarflexion of the metatarsal with reduction of the intermetatarsal angle. Proximal osteotomies are well suited to correction of this type of combined deformity.
An abnormally large sagittal plane deviation of the metatarsal can be more effectively corrected with an osteotomy of the first metatarsal base. An elevated first metatarsal may be effectively addressed at the base of the metatarsal because there will be more effective plantarflexion of the metatarsal as the resection of a small amount of bone wedge at the base translates into a larger amount of plantar deflection of the metatarsal when compared with resection of a distal wedge of bone. If a similar amount of plantarflexion could be achieved with a distal metatarsal osteotomy, it would more abruptly change the vectors of the flexor and extensor tendons crossing the joint. This change in vectors would potentially have a greater disruption of the muscular balance of the first metatarsal phalangeal joint, which could lead to a nonpurchasing or cock-up hallux.
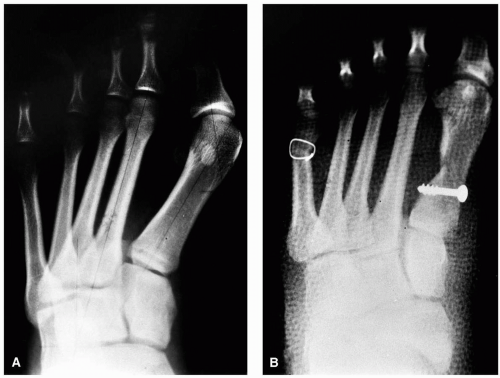 FIG. 2. A: A preoperative radiograph of a patient with hallux valgus deformity with concomitant metatarsus adductus. B: A closing base wedge osteotomy was performed to reduce the first intermetatarsal space. |
Hallux Abducto Valgus with Metatarsus Adductus
Some investigators have described the association of hallux abducto valgus with metatarsus adductus. LaReaux and Lee found that 35% of their patients with hallux abducto valgus had a metatarsus adductus deformity, compared with only 13% in a control group (9). Measurements of radiographs in 115 feet without evidence of hallux abducto valgus demonstrated a statistically significant and direct relationship between an increasing metatarsus adductus angle and an increasing hallux abductus angle (10). Banks et al. noted, in their series of patients with juvenile hallux abducto valgus, that 48 of the 72 cases had a metatarsus adductus angle greater than 15 degrees (11). Furthermore, an association was noted between an increasing metatarsus adductus angle and increasing amounts of hallux abductus.
The initial radiographic evaluation of hallux abducto valgus in patients with a concomitant metatarsus adductus is often misleading. Significant abduction of the hallux may be noted, yet with little intermetatarsal splay (Fig. 2). However, one must consider that the generalized adductus of the forefoot results in a greater functional value of the intermetatarsal angle. In this situation, the true intermetatarsal angle may best be estimated by the following formula (12):
True intermetatarsal angle = (Metatarsus adductus angle − 15 degrees) + Intermetatarsal angle
This formula provides a better determination of the actual intermetatarsal angle being treated.
When repairing a hallux abducto valgus deformity in a patient with metatarsus adductus, the surgeon should reduce the intermetatarsal angle to 0 degrees or a slightly negative value to minimize the chance of recurrence of hallux abducto valgus (12). Despite excellent correction, the hallux may not remain perfectly rectus, but it may resume a slightly abducted alignment postoperatively. The longer radius for correction with a proximal osteotomy is well suited to achieve the degree of correction that is desirable.
Juvenile Hallux Abducto Valgus Deformity
The development of a hallux abducto valgus deformity in young patients represents significant deforming forces acting on the foot. Patients with juvenile hallux abducto valgus often present with other significant deformities. Banks et al. found that 66.7% of their patients with juvenile hallux abducto valgus deformity possessed a metatarsus adductus angle greater than 15 degrees (11). Pes valgus deformity and ankle equinus have also been associated with juvenile hallux abducto valgus (12, 13, 14, 15).
In the younger patient, correction of hallux abducto valgus deformity must be maintained over decades. Studies have shown that the incidence of recurrence of the deformity is higher in young patients undergoing a soft tissue procedure or distal osteotomy (16, 17, 18). The intermetatarsal angle in juvenile and adolescent patients is best reduced to 0 degrees or closely approximating that value to minimize the possibility of recurrence. In most patients, this goal can be more effectively accomplished with a proximal osteotomy.
 FIG. 3. A: Preoperative radiograph of a patient after a simple Silver bunionectomy with narrowing of the metatarsal head. This may preclude the use of a capital osteotomy for subsequent repair. B: Radiograph after a closing base wedge osteotomy. |
Iatrogenic Deformities
Correction of a recurrent hallux abducto valgus deformity often represents a difficult challenge. The metatarsal head is typically narrowed from the previous surgical procedure, and this configuration may make the use of a capital osteotomy difficult for the degree of correction required (Fig. 3). Furthermore, the presence of any retained fixation devices may compromise the integrity of the bone, so additional osteotomies at this level may pose more of a risk relative to fixation. In these instances, a proximal osteotomy may prove the best alternative, even if the intermetatarsal angle is low.
ANATOMIC CONSIDERATIONS
The choice of incisions for proximal osteotomies has been debated, but an effective incision may be placed dorsally
along the first ray slightly medial to the extensor hallucis longus tendon. The incision commences proximal to the first metatarsocuneiform joint and extends distally to the proximal phalanx. Typically, the distal segment of the incision is initiated and the metatarsophalangeal joint is released, and then the incision is extended proximally to provide access for the osteotomy (Fig. 4). The single-incision approach has been employed for decades without deleterious sequelae (8).
along the first ray slightly medial to the extensor hallucis longus tendon. The incision commences proximal to the first metatarsocuneiform joint and extends distally to the proximal phalanx. Typically, the distal segment of the incision is initiated and the metatarsophalangeal joint is released, and then the incision is extended proximally to provide access for the osteotomy (Fig. 4). The single-incision approach has been employed for decades without deleterious sequelae (8).
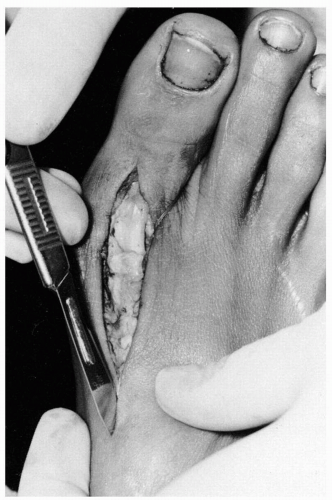 FIG. 4. Once the first metatarsophalangeal joint dissection has been accomplished, the skin incision is extended proximally for execution of the base osteotomy. |
Once the skin incision is completed, dissection is carried through the relatively thin subcutaneous tissues. The previously defined tissue planes may be followed from the more distal aspect of the wound into the proximal metatarsal area. At the proximal aspect of the incision, one typically encounters a branch of the medial dorsal cutaneous nerve. This nerve is easily retracted into the medial subcutaneous tissues. Once the superficial fascia has been cleared from the deeper structures, the deep fascia is incised along the medial aspect of the extensor hallucis longus tendon. This provides for effective retraction of the tendon and better exposure of the base and shaft of the metatarsal. The periosteum is then incised and reflected from the base of the metatarsal. Additional dissection of this layer may be required both medially and laterally to allow satisfactory clearance for the saw blade during the performance of the osteotomy as well as the insertion of internal fixation.
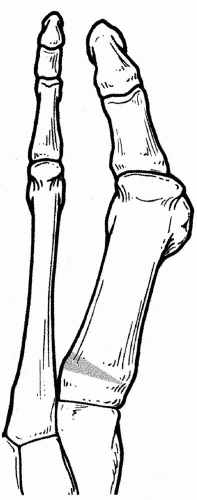 FIG. 5. The transverse closing base wedge osteotomy. |
TECHNIQUES
Closing Base Wedge Osteotomy
The closing wedge osteotomy has been the standard technique for base procedures for many years. Traditionally, the procedure was performed in a transverse orientation, and fixation was provided by Kirschner wires (K-wires), intraosseous wire loops, or other methods (Fig. 5). The transverse wedge osteotomy was modified to an oblique orientation to accommodate screw fixation (8) (Fig. 6). In addition, the oblique orientation allows the surgeon to place the apex of the osteotomy further proximally, thus providing a longer radius arm for correction. More freedom was obtained in
maneuvering the oscillating saw for performance of the procedure. With this technique, the handle of the saw is directed medially away from the foot and is free from the interference and contact of the foot itself. Therefore, the surgeon need not worry that the saw may be misdirected during the osteotomy.
maneuvering the oscillating saw for performance of the procedure. With this technique, the handle of the saw is directed medially away from the foot and is free from the interference and contact of the foot itself. Therefore, the surgeon need not worry that the saw may be misdirected during the osteotomy.
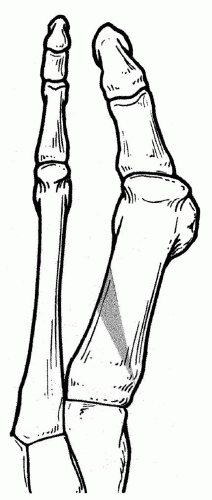 FIG. 6. The oblique closing base wedge osteotomy. |
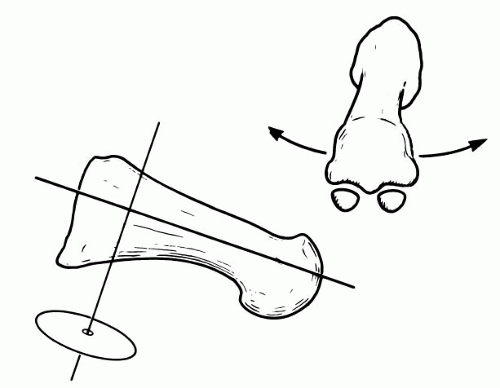 FIG. 7. Traditional axis of the base wedge osteotomy. If the osteotomy is made perpendicular to the metatarsal, subsequent lateral displacement of the distal metatarsal will result in sagittal plane dorsiflexion as well. Such may be the cause of a short first metatarsal. |
Regardless of which orientation is employed, the use of an axis guide may facilitate the performance of the osteotomy. The axis guide also provides an accurate means of assessing and implementing concomitant dorsiflexion or plantarflexion of the distal metatarsal with closure of the osteotomy. During the base wedge osteotomy of the first metatarsal, an intact cortical hinge acts as an axis of rotation (8). The traditionally perceived axis for a hinged osteotomy of the first metatarsal was perpendicular to the long axis of the bone. Because of the anatomic declination of the first metatarsal in the human foot, rotation of the distal segment of the first metatarsal around this axis after a closing base wedge osteotomy would tend to create elevation of the metatarsal head from the weight-bearing surface (Fig. 7). However, designing the osteotomy so the axis is perpendicular to the weight-bearing surface allows for full rotation of the distal segment of the metatarsal without elevating or plantarflexing the metatarsal head in relation to the weight-bearing plane (Fig. 8).
The previous description of the sagittal plane orientation of the axis is based on the given relationship that the axis is perpendicular to the transverse plane when viewed in the frontal projection. Logically, manipulation of the axis in the frontal plane may influence the ultimate position of the metatarsal head in relation to the weight-bearing surface. Manipulation of the axis in the frontal plane is based on the presumption that the axis remains perpendicular to the weight-bearing surface in the sagittal plane.
With the axis perpendicular to the weight-bearing surface in the frontal plane, lateral rotation of the distal metatarsal segment maintains the metatarsal head on the weight-bearing surface (Fig. 9). When the superior pole of the axis is tilted laterally, a dorsomedial hinge is created, and plantarflexion of the distal segment of the metatarsal occurs with lateral rotation or closing of the wedge osteotomy (Fig. 10). Conversely, when the superior pole of the axis is tilted medially, a plantar medial hinge is created, and dorsiflexion of the distal segment occurs with closing of the wedge osteotomy (Fig. 11).
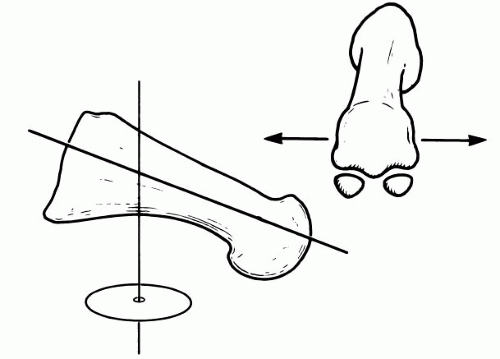 FIG. 8. If the osteotomy is made perpendicular to the weight-bearing surface, then lateral displacement of the distal metatarsal will not dorsiflex or plantarflex the metatarsal head, and it should remain parallel with the weight-bearing surface. |
The concept of the axis relationship just described may be directly applied to the actual execution of the closing base wedge osteotomy of the first metatarsal. A 0.045-inch K-wire
can be drilled through the base of the first metatarsal to represent the functional hinge of the intended osteotomy. The K-wire should penetrate the dorsal cortex just short of the apex of the intended osteotomy, to allow for additional feathering of the hinge. The wire is then drilled to penetrate the metatarsal at the appropriate angle, which affects manipulation of the distal metatarsal as required for each individual case.
can be drilled through the base of the first metatarsal to represent the functional hinge of the intended osteotomy. The K-wire should penetrate the dorsal cortex just short of the apex of the intended osteotomy, to allow for additional feathering of the hinge. The wire is then drilled to penetrate the metatarsal at the appropriate angle, which affects manipulation of the distal metatarsal as required for each individual case.
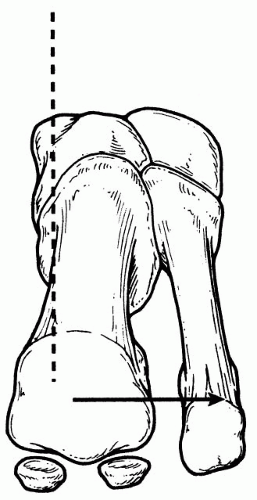 FIG. 9. Proper frontal plane orientation must be observed as well. Same perpendicular relationship of the axis is essential if the distal segment is to remain on the weight-bearing surface after closure of the osteotomy. |
 FIG. 10. Altering the position of the axis may be used to the surgeon’s advantage. If the axis is tilted laterally, then a dorsomedial hinge is created. When the osteotomy is closed, plantarflexion of distal segment occurs. |
With the K-wire in place, the relationship of the axis with the weight-bearing surface is evaluated from a medial and frontal perspective. The position of the axis may easily be changed before the osteotomy by simply removing and reinserting the K-wire.
The wedge osteotomy is then cut by keeping the plane of the saw blade in line with the axis guide so the planes of the two cuts converge at the K-wire. The medial cortex of the metatarsal remains intact as a physical hinge that coincides with the axis and planes of the intersecting wedge osteotomies. The osteotomy may be feathered to create a flexible yet intact hinge that bends but does not fracture with manual reduction. Christensen et al. showed that the intact medial hinge provides stability to the osteotomy and functions as another point of fixation (19). If the hinge fractures, the stability of the osteotomy will be reduced, and fixation may prove more difficult.
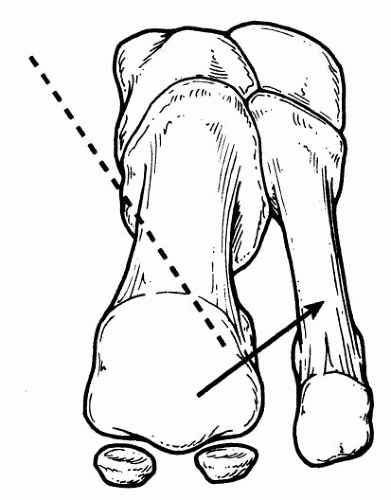 FIG. 11. Should dorsiflexion of the distal segment be necessary, then the axis should be tilted medially. |
Various forms of fixation have been employed with the closing base wedge osteotomy, and studies have been conducted in an attempt to determine which form of fixation is more stable (20,21). An important factor for a successful closing base wedge osteotomy is the presence of two points of fixation. An intact medial cortical hinge may be considered one point of fixation. The transverse wedge osteotomy is more commonly stabilized with crossed K-wires or cerclage wire. Evidence seems to indicate that when a K-wire is used, the osteotomy is more stable if the wire crosses the metatarsal-cuneiform joint (21). Cerclage wire appears to provide the most stability when it is applied at the plantar aspect of the metatarsal, such that it prevents disruption by the weight-bearing forces (20).
Although K-wires and cerclage wire are commonly used for fixation, the technique I favor is the use of two 4.0-mm partially threaded cancellous screws to secure the osteotomy. This has provided effective fixation and a high rate of success. The first screw is placed distal to the medial hinge and is oriented perpendicular to the metatarsal. The second screw is positioned distal to the first and is oriented perpendicular to the osteotomy (Fig. 12). Alternatively, crossed-screw fixation of the base wedge has been described, with favorable results (22). The cancellous screws are employed more often because they provide rigid fixation of the osteotomy, regardless of the integrity of the bone. However, provided non-weight-bearing is instituted after surgery, both crossed 0.062 K-wires and a single screw may provide good results that are comparable (23). Cortical bone screws also provide good stabilization.
The closing base wedge osteotomy has always been an effective means of reducing the intermetatarsal angle, although early reviews noted that shortening of the first metatarsal was a common occurrence after a transverse base wedge osteotomy (3, 4, 5, 6, 7). As a consequence, metatarsalgia, painful plantar callosities, and stress fractures of the lesser metatarsals developed in some patients. However, the base wedge osteotomy was not totally abandoned because it provided a much needed alternative in patients with severe deformities with high intermetatarsal angles. A few workers persisted in the investigation of the procedure (24), and the technical aspects were further advanced by the application of rigid internal fixation across angulated osteotomies. However, elevation of the first metatarsal continued to develop even with the use of the new fixation
techniques. Although some authors proposed that the change in metatarsal declination was related to the removal of excessive amounts of bone from the dorsal aspect of the osteotomy (6), Schuberth et al. attributed this phenomenon to weight bearing in the postoperative period before osseous healing had occurred, as opposed to its being a primary complication of the procedure itself (7). Furthermore, the radiographic appearance of a shortened metatarsal could largely be explained by the elevation of the distal fragment, which could be overcome by geometrically correct osteotomy and an appropriate interval of non-weight-bearing during the healing process (8). Later investigators proved that the shortening associated with the oblique base wedge osteotomy was less than actually perceived. Using both mathematic and bone models, investigators determined that the average oblique base wedge osteotomy would result in less than 2 mm of shortening, comparable to most other osteotomies (25). Therefore, elevation of the first metatarsal would be a primary means of creating the appearance of a “shortened” metatarsal on dorsoplantar radiographs. Other investigators noted that early weight bearing in the postoperative period either contributed to or directly caused failure of the fixation (26).
techniques. Although some authors proposed that the change in metatarsal declination was related to the removal of excessive amounts of bone from the dorsal aspect of the osteotomy (6), Schuberth et al. attributed this phenomenon to weight bearing in the postoperative period before osseous healing had occurred, as opposed to its being a primary complication of the procedure itself (7). Furthermore, the radiographic appearance of a shortened metatarsal could largely be explained by the elevation of the distal fragment, which could be overcome by geometrically correct osteotomy and an appropriate interval of non-weight-bearing during the healing process (8). Later investigators proved that the shortening associated with the oblique base wedge osteotomy was less than actually perceived. Using both mathematic and bone models, investigators determined that the average oblique base wedge osteotomy would result in less than 2 mm of shortening, comparable to most other osteotomies (25). Therefore, elevation of the first metatarsal would be a primary means of creating the appearance of a “shortened” metatarsal on dorsoplantar radiographs. Other investigators noted that early weight bearing in the postoperative period either contributed to or directly caused failure of the fixation (26).
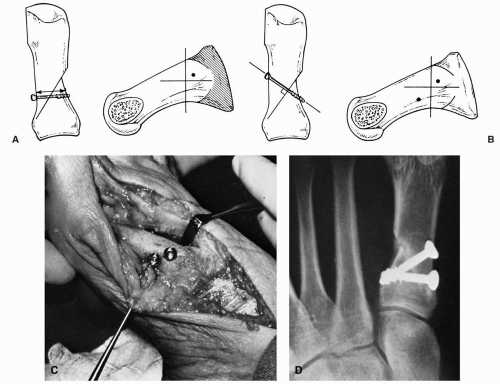 FIG. 12. Two-screw fixation for the oblique closing base wedge osteotomy. A: The anchor screw is oriented perpendicular to the medial cortex or long axis of first metatarsal. B: Compression screw perpendicular to the plane of the osteotomy. C: Medial orientation of the two-screw technique. D: Compression and anchor screws. |
However, later authors who instituted at least 6 weeks of non-weight bearing after the closing base wedge osteotomy continued to find evidence of first metatarsal elevatus, although of far less magnitude and with few associated problems (19,27,28). Nonetheless, patient satisfaction rates were high, and evaluations of the results by the investigators were similar. The problems of transfer lesions or other symptoms related to the alignment of the first ray were minimal. In one study, 44% of patients admitted to premature weight bearing on the extremity (28). Whether this is a consistent finding in other patient groups or whether this accounts for the small degree of metatarsal elevation is unknown. In addition, an inconsistency is noted in the means by which first metatarsal elevation has been measured on radiographs, and
at times the values could have been affected by the position of the foot. Therefore, it appears that at the current levels of elevation noted with non-weight bearing in the postoperative setting, this phenomenon is clinically inconsequential. Good correction can be achieved with restoration of function.
at times the values could have been affected by the position of the foot. Therefore, it appears that at the current levels of elevation noted with non-weight bearing in the postoperative setting, this phenomenon is clinically inconsequential. Good correction can be achieved with restoration of function.
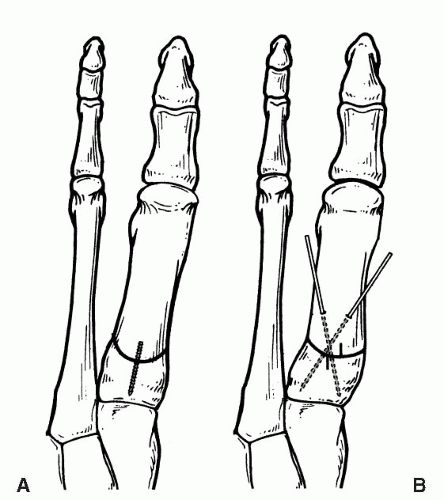 FIG. 13. A,B: The crescentic first metatarsal osteotomy. A notch may be made on each side of the osteotomy before rotation to help assess the amount of correction achieved. |
Crescentic Osteotomy
The crescentic osteotomy is another popular technique for achieving reduction of the intermetatarsal angle at the proximal aspect of the first metatarsal. This procedure may provide correction of deformity in all three planes (Fig. 13). Because no bone is resected, this procedure theoretically produces little shortening (29), so it may be a good alternative in the patient who has a significantly short first metatarsal. However, the performance of any osteotomy creates some amount of shortening, typically in the range of 1 to 2 mm. The osteotomy has been modified to include a plantar shelf in an attempt to provide more stability (30).
A special crescentic blade is necessary to perform the procedure. The saw blade is oriented with the concavity directed proximally, so there is more excursion of the bone segments to allow for correction of the intermetatarsal angle. This also allows for better bone contact once the osteotomy is rotated (31). Cohen et al. and Kay et al. demonstrated how the orientation of the blade directs the correction in each plane (29,30). As in the closing base wedge osteotomy, the cut should be oriented so the saw is perpendicular to the weight-bearing surface to prevent dorsiflexion of the distal metatarsal with lateral rotation. If the blade is oriented laterally, then plantarflexion of the distal segment will occur, with reduction of the intermetatarsal angle. If the blade is oriented medially, then dorsiflexion will occur with translation of the osteotomy.
The osteotomy is best performed distal to the plantar flare of the metatarsal; otherwise, the cut will be difficult to complete. A small notch may be made at the intended osteotomy site, to provide a better determination of the amount of correction that is achieved with rotation of the distal segment (Fig. 14). However, care must be taken not to produce significant plantarflexion and inversion during correction of more severe deformities. It appears that the best correction of the intermetatarsal angle may be achieved when the saw diameter is larger than the diameter of the osteotomy site (31).
Although the crescentic osteotomy does provide good correction, it has some disadvantages. Because there is no fixed hinge, the osteotomy is unstable, and this feature may make it difficult to achieve solid, reliable fixation across the osteotomy site. The cannulated screw system has facilitated this process (32). Fixation may consist of one screw (33,34), two screws (32), one screw and one K-wire (35), crossed K-wires, or Steinmann pins. The screws can become prominent at a later time and may require removal (33).
Cohen et al. described a modification of the crescentic procedure that incorporated a plantar shelf to enhance overall stability (30). A K-wire was introduced medially at the apex of the osteotomy, and the plantar shelf was created initially with a sagittal saw. The dorsal crescentic cut was then performed. Good results were noted without sagittal plane deviation of the first metatarsal. Later studies comparing the crescentic shelf and standard crescentic procedures indicated that, by using the shelf procedure, one could produce slightly greater reductions in the intermetatarsal angle and enhanced plantarflexion of the distal metatarsal, although the differences were not statistically significant. Overall, both procedures possessed similar mechanical properties, although investigators believed that the shelf osteotomy may be easier to fixate (36).
Favorable results have generally been reported with the procedure (30,32, 33, 34, 35,37). Although the crescentic osteotomy may tend to resist sagittal plane disruptive forces more effectively than a base wedge osteotomy (38), weight bearing cannot be recommended before osseous consolidation. Unrestricted weight bearing has been associated with metatarsal elevation (33, 34, 35), although most authors have apparently not altered their postoperative regimen to prevent this potential problem.
Chevron Osteotomy
The procedure was first described by Kotzenberg in 1929 as a horizontal “V” in Schotte’s article (39). The osteotomy is performed 1 to 1.5 cm from the metatarsal cuneiform joint. The apex of the osteotomy can be oriented either distally or proximally, although most surgeons appear to favor a distal apex. In either instance, care should be taken to avoid compromise of the first metatarsal cuneiform joint (Fig. 15). The same axis guide techniques described for osteotomies of the metatarsal head may be incorporated into the proximal procedure to shorten, lengthen, dorsiflex, or plantarflex the distal metatarsal with lateral transposition. However, because the osteotomy is primarily transpositional, it does not appear to provide any advantage over the more distally based Austin procedure. Regardless of the location of the osteotomy, similar amounts of lateral shift result in similar reductions in the intermetatarsal angle. Improved correction may be achieved with the proximal chevron procedure if the distal segment is swiveled laterally before fixation. The design of the osteotomy affords good stability in the sagittal plane.
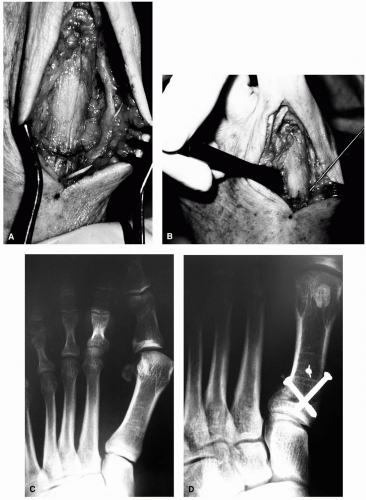 FIG. 14. A: The crescentic osteotomy is performed with the concavity directed proximally. B: A crescentic osteotomy is temporarily fixated with a guidewire for a cannulated screw. C: A preoperative radiograph of a patient with a high intermetatarsal angle. D: After the crescentic osteotomy and fixation with two cannulated screws. (Courtesy of Ira Fox, D.P.M.)
Related posts: Anatomic Dissection of the First Metatarsophalangeal Joint for Hallux Valgus Surgery Anatomic Dissection of the First Metatarsophalangeal Joint for Hallux Valgus Surgery
 Juvenile Hallux Abducto Valgus Deformity Juvenile Hallux Abducto Valgus Deformity
 Digital and Sesamoid Fractures Digital and Sesamoid Fractures
 Distal Metaphyseal Osteotomies in Hallux Abducto Valgus Surgery Distal Metaphyseal Osteotomies in Hallux Abducto Valgus Surgery
 Congenital Deformities Congenital Deformities
 Osteotomies of the First Metatarsal Shaft in Hallux Abducto Valgus Osteotomies of the First Metatarsal Shaft in Hallux Abducto Valgus
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|