Principles of Muscle-Tendon Surgery and Tendon Transfers
Principles of Muscle-Tendon Surgery and Tendon Transfers
Stephen J. Miller
Mack Jay Groves IV
One of man’s greatest attributes is his ability to move. Purposeful active movement is dependent on many factors, but primarily on the ability of a myocyte to contract and thereby reduce its length. This motion is transmitted to the skeleton through a collection of longitudinally oriented collagen fibers: a tendon.
Enhanced understanding of the biomechanics of normal foot function and the pathomechanics of abnormal foot structure has led to the effective use of muscle-tendon transfers by the foot and leg surgeon. The goal of these procedures is to improve foot function through selective motor redistribution, with or without associated joint stabilization. As stated by Hackenbroch, “A tendon transplantation produces some benefits, redirects the powers, and is conservative in maintaining function as well as form. It does not create a new source of movement, but it utilizes efficiently the available power by eliminating less important motions and directing it to better advantage” (2). Tendon transfer is best applied in flexible deformities in which there is a dynamic muscular imbalance, such as in the conditions listed in Table 76.1.
The clinical foundations for various types of tendon transfers were developed largely in Germany and then further evolved in the United States (2,3 and 4). The first recorded tendon transfer was that of a peroneus longus muscle by Nicoladoni in Vienna on April 15, 1881. Ten years later, intense interest developed in this area, pioneered by the German authors Lange, Biesalski, Vulpius, and Stoffel. However, Mayer stands out as the anatomic, literary, and clinical father of the modern concepts of tendon transfer (3,5,6,7,8,9 and 10). Bernstein (11,12), Steindler (13,14), Ober (15), and Bunnell (16,17,18 and 19) in the United States added much to Mayer’s work.
The development of major tendon transfers in the podiatric community was first published by McGlamry (20) in 1973. They reported modifying the split tibialis anterior tendon transfer (21), Young tenosuspension (22,23) for weak foot, and Jones metatarsal suspension (24). Principles of tendon surgery were then incorporated into the treatment of the equinus foot (25,26). Sgarlato (27) presented the flexor tendon transfer for hammer toes in 1970.
The redistribution of the torque forces about the foot and ankle requires the application of specific principles based on a knowledge and understanding of the anatomy, physiology, and mechanics of the musculotendinous structures involved.
This includes a knowledge of tissue histology, support structures, circulation, healing processes, and biomechanics that affect tendon function.
DEFINITIONS
Terms crucial to understanding this chapter are defined here.
Tendon transfer: A tendon transfer is the detachment of a tendon of a functioning muscle at its insertion and then its relocation to a new insertion or attachment (28).
Tendon transposition: Tendon transposition is the rerouting of the course of a normal muscle tendon without detachment to assist other functions (29). It is sometimes known as a tendon translocation (28). However, translocation refers more to the rerouting of a tendon, whether it is detached or not detached.
Muscle—tendon transplantation: The detachment of a muscle tendon at both its origin and its insertion and moving it to a new location along with its neurovascular support structures constitute a muscle-tendon transplantation (28).
Tendon suspension: Also known as tenosuspension, tendon suspension refers to those tendon procedures designed to support a structure (e.g., Young tenosuspension, Jones tenosuspension).
TENDON ANATOMY
Muscles do not insert directly in the manner in which they originate. Tendons serve as a bridge between muscles and their insertions and thereby transmit the forces generated by the muscles to produce torque about joint axes. Tendons do not contract but are flexible and slightly extensible. Their fibers are able to resist tension so that muscle contractile energy is not lost during transmission of the force to the insertion.
In essence, tendons are smooth, cord-like, flat or round structures composed of parallel fibers flexible enough to be angulated around bone surfaces or deflected beneath retinacula. Yet, they have incredible strength, more per unit area than muscles. In fact, their tensile strength is as great as that of bone, with a breaking point similar to that of steel (30,31). Large, flattened tendon structures are known as aponeuroses.
Most importantly, these amazing tendons accommodate movement as they transmit force by having the ability to glide. Such gliding is assisted by a number of support structures. Naturally, tendons have a large excursion closer to their muscle connections, diminishing to virtually no gliding motion relative to background structures as they near their insertion.
In summary, with their unique structure and characteristics, tendons have a remarkable influence on foot functions, even though they are the passive component of the musculotendinous unit.
DEFINITION AND HISTOLOGY
A tendon is a cord-like, viscoelastic structure suitable for transferring large tensile forces produced by the contraction of muscle to bone so that distant movement can occur about joint axes. It requires smooth gliding along its course and flexibility of associated joints to function properly.
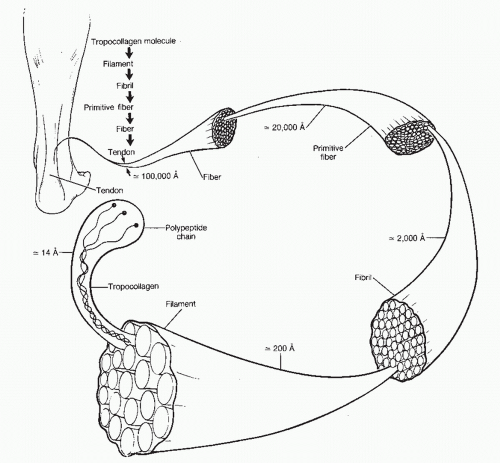
Histologically, tendons consist of about 30% collagen and 2% elastin within an extracellular matrix or ground substance containing 68% water. They also contain reticulin, which provides bulk. The majority of the collagen is type I, synthesized by fibroblasts and making up approximately 70% of the dry weight of a tendon. The structural unit of collagen is a long, thin protein molecule known as tropocollagen, which is formed outside the fibroblast from the procollagen that is formed inside the cell. Almost two-thirds of the procollagen molecule is made up of the amino acids glycine (33%), proline (15%), and hydroxyproline (15%). The tropocollagen molecules are laid down parallel to one another such that each molecule overlays the adjacent ones by 10% to 25% of its length. The molecules are polymerized via chemical bonds to form collagen filaments that have the characteristic banding seen in the light microscope at 640 angstroms (Aå). These filaments aggregate into fibrils of about 2,000 Aå in diameter, which, in turn, accumulate to make up the basic collagen fiber (Fig. 76.1).
TABLE 76.1 Some Applications for Tendon Transfer
Post poliomyelitis
Leprosy
Duchenne muscular dystrophy
Charcot-Marie-Tooth disease
Cerebral palsy
Multiple sclerosis
Discogenic disease
Sciatic nerve palsy
Common peroneal nerve palsy dropfoot
Dorsal bunions
Recurrent clubfoot
Flexible flatfoot
Forefoot equinus
Hallux valgus
Hallux varus
Flexible hammer toes
Ankle stabilizations
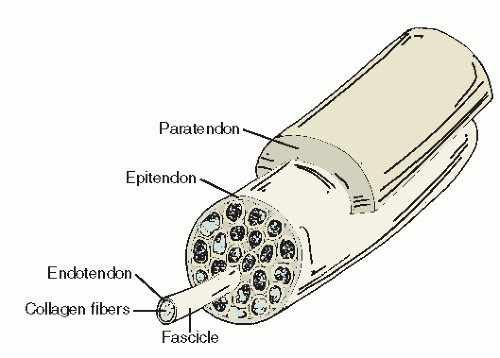
Collagen fibers are condensed into fascicles, and both units are surrounded by areolar connective tissue known as endotenon. It contains blood vessels, lymphatics, and nerves, as well as the fibroblasts that repair and replace the collagen fibrils. In fact, the fibroblasts replace all of the collagen in the tendon every 6 months. The fascicles are bound together to form the tendon, which is covered with the epitenon, a one- to two-cell fibroblastic and synovial layer continuous with the endotenon septa. The epitenon covering is sometimes referred to as the visceral layer, and it moves with the tendon (Fig. 76.2).
STRESS AND STRAIN CURVE
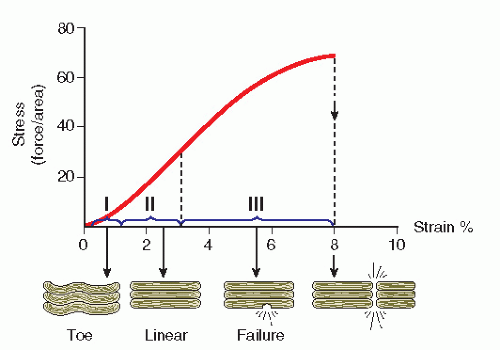
In the resting state of a tendon, the collagen fibers have a zigzag or wavy configuration that straightens as the tendon is stretched by 2%. Up to 4% stretch, even though the collagen fibers deform, they will return to their original length. When the tendon is stretched between 4% and 8%, the cross-links start to fail as the fibers begin to slide past one another, with the weaker fibers starting to rupture microscopically. Physiologic loading, therefore, is less than 4% stress, which is the safe zone. Past 8% stretch, the tendon will rupture (Fig. 76.3). The maximum load capacity and tear resistance both decrease with age, with peak values occurring in the third decade (31). In contrast, the elastin, which contributes to the flexibility of a tendon, can elongate up to 70% of its length without rupture and breaks at 150% of its length.
SUPPORT STRUCTURES AND ANATOMY
Straight Course—Paratenon
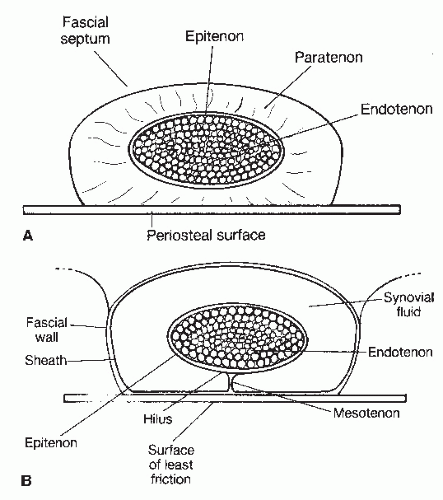
The supporting or surrounding tissue of a tendon varies, depending on whether the tendon has a straight pull or must travel around a corner. Along its straight course, a tendon is surrounded by a loose elastic areolar tissue known as the paratenon. This areolar tissue is continuous with the epitenon and perimysium, as well as the coverings of the nerves and blood vessels that it carries to the tendon. The supporting tissue fills the fascial space in which the tendon passes, and its elasticity enables the paratenon to stretch safely several centimeters with tendon movement. A good example of paratenon is found around the Achilles tendon. Together, the epitenon and paratenon are called the mesotenon (Fig. 76.4).
Angled Course—Tendon or Synovial Sheath
Where a tendon rounds a corner, changes direction, or passes under ligamentous structures, it is surrounded by a tendon sheath, through which the tendon is prevented from bowstringing across a joint. In other words, the sheath acts like a pulley. The tendon sheath is a tubular structure lined for the most part with synovial cells and within which the tendon glides back and forth, much like a piston within a cylinder. Similar to the peritoneum, the sheath consists of two layers: the epitenon corresponding to the visceral layer and the inner side of the sheath corresponding to the parietal layer. Just as the intestinal mesentery is formed, these two layers reflect on themselves to form the mesotenon, a thin, delicate elastic membrane that will stretch several centimeters and that carries the tortuous blood, nerves, and lymphatic vessels to the tendon. The point at which it is attached to the epitenon of the tendon is termed the hilus. The mesotenon is always located on the longitudinally convex side of the tendon where there is the least friction, and it is continuous with the areolar tissue surrounding the tendon proximal and distal to the sheath (Fig. 76.5). At those locations on either end of the sheath, the connective tissue covering is doubled on itself to form invaginating folds known as plicae. These plicae provide for free pistoning motion of the tendon, stretching or folding in accordance with the tendon pull, and thereby protect the vital mesotenon from excessive tension.
Gliding Mechanism
Therefore, the gliding mechanism of the tendon is dependent on these delicate tissues that also contain life support structures. In a straight course, the paratenon assumes such responsibility, whereas around corners, the mesotenon assisted by the plicae will allow liberal to-and-fro motion. The width of the mesotenon determines the degree of motion allowable between tendon and bone. These fine stretchable tissue coverings must be carefully preserved and repaired as necessary during surgery if one is to avoid tendon adhesions.
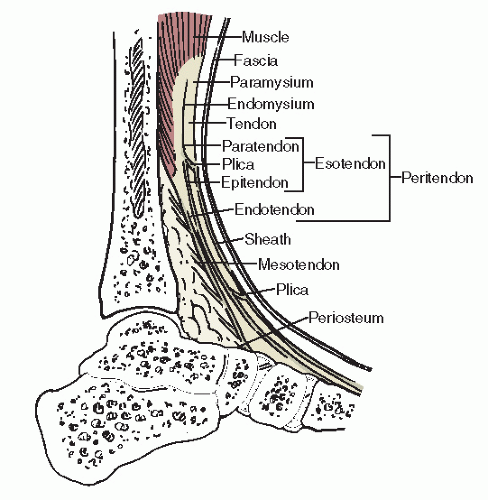
When the tendon sheath is absent, the tendon and overlying paratenon are enveloped in fatty areolar tissue. On the other hand, in some situations, there is no mesotenon accompanying the tendon within the tendon sheath. Mayer (4) found this to be the case with the tendon of the tibialis posterior 100% of the time; the flexor digitorum longus is 50% of the specimens. To avoid confusion, the term peritenon refers to all the connective tissue structures associated with the tendon, including the paratenon, mesotenon, epitenon, and endotenon (Fig. 76.6).
Figure 76.1 Schematic diagram showing the organization of the components of a collagen fiber, many of which make up a tendon.
Tendon Circulation
A tendon receives its blood supply via three sources:
A small part comes from the central blood vessels originating in the muscle belly.
Some is derived from vessels of the bone and periosteum near the point of insertion of the tendon.
Most of the blood supply, however, comes from the small vessels running in the paratenon or through the mesotenon, entering by way of the hilus.
These vessels then travel longitudinally in the epitenon and branch out, anastomosing freely, and also penetrate the endotenon, where they supply the fasciculi of the tendon (Fig. 76.7). Where the mesotenon is absent within a tendon sheath, the blood is carried to the tendon through the elastic membranous tissue called vincula, another term for plicae, at each pole of the sheath (4,12). Tendons also receive nutrition from local lymphatic and synovial fluid because between these major sources of blood supply are zones of apparent avascularity (1). Studies suggest that the synovial fluid diffusion can provide nutrition at least equal to that of the vincula vessels (32).
Avascular zones have particular clinical significance in the Achilles and posterior tibial tendons (33,34), where there is further compromise due to cyclical loading or friction. The reduced area of circulation 2 to 6 cm proximal to the insertion of the Achilles tendon probably explains why a tendo Achillis lengthening heals more slowly than a recession of an aponeurosis.
Figure 76.2 Tendon anatomy showing various bundles and their coverings.
Preservation of blood supply is an important principle of tendon surgery. It not only provides for the metabolic and healing production of amino acids and collagen but also minimizes the formation of adhesions.
Tendon Nerve Supply
The innervation of a tendon is entirely afferent and is derived from two sources: the muscle in the musculotendinous junction and fibers from the external local nerves, both subcutaneous and deep. The afferent receptors are the mechanoreceptor Golgi tendon organs (GTOs), which monitor increases in tension rather than length, and the lamellated corpuscles, which respond to pressure-type stimuli from the surrounding tissues. The GTOs provide feedback to reduce muscle tension during excessive muscular contraction (35,36). There are also afferent fibers that transmit pain, but their anatomy and distribution have not been studied in detail.
Figure 76.3 A stress-strain curve for tendon. (Adapted from Curwin S, Stanish WK. Tendinitis: its etiology and treatment. Lexington, MA: DC Heath and Company, 1984.)
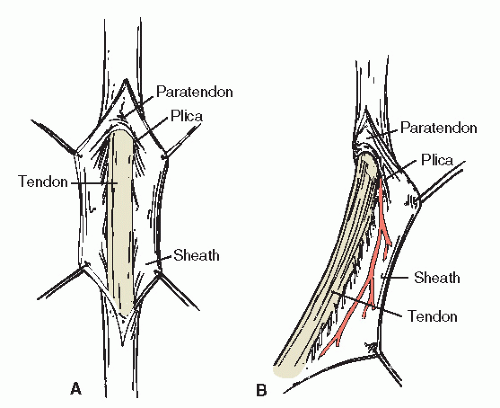
Figure 76.4 A: Tendon with paratenon shown in cross section. B: Tendon with sheath shown in cross section.
Tendon Torsion
Several tendons that insert in the foot yet originate extrinsically demonstrate various degrees of longitudinal torsion along the courses toward their attachments. The functional and surgical significance of the torsion varies for each tendon. Twisting of the Achilles tendon is well documented and begins proximal to the point at which the soleus fibers tend to merge (37,38). The degree of rotation varies from 11 to 65 degrees and has been classified into three groups of torsion: least, moderate, and extreme (39). Therefore, the relationship of the fibers of the gastrocnemius and soleus portions of the tendo Achillis varies. The obvious surgical implication is in how the fibers should best be cut to exact a tendon lengthening.
Figure 76.5 Drawing of an extensor hallucis longus tendon to show the relationship of the paratenon, mesotenon, and the sheath to the tendon itself. A: AP view. B: Lateral view.
Figure 76.6 Longitudinal section through the tibialis anterior tendon and surrounding structures.
As for functional implications, one theory is that torsion is nature’s way of increasing the strength of the Achilles tendon during weight-bearing and preventing rupture (39). Another theory is that torsion allows elongation and elastic recoil and stores energy that can be released during the propulsive phase of gait (40). It has also been suggested that the evolution of tendo Achillis torsion occurs during postnatal development and functions to facilitate combined movement about the oblique axes of the ankle and subtalar joints (41,42). Even though the hypovascularity of the Achilles tendon 2 to 6 cm above its insertion has been shown to not directly cause rupture (43), it has been noted that the twist in the tendon is most pronounced in this area and may affect the internal vascularity (44).
Figure 76.7 Blood supply as depicted to tendon in a digital sheath.
The tendon of the tibialis posterior muscle has been shown to exhibit a mean torsion of 47.5 degrees, counterclockwise on the right and clockwise on the left, proximal to distal (45). This torsion has been shown to equalize excursion of the tendon and eliminate the need for any longitudinal slippage between individual tendon fibers (46). The surgical implications generally apply to reconstruction of local tendinopathy.
Torsion has also been measured in the peroneus brevis tendon with a mean of 38.5 degrees, twisting clockwise on the right and counterclockwise on the left, proximal to distal (47). The functional and surgical significance of the phenomenon in this tendon remains to be investigated. Surgeons should be aware of the twist when harvesting tendon grafts from the peroneus brevis tendon for procedures such as ankle stabilizations.
The fibers of the tibialis anterior tendon have demonstrated a 90-degree medial rotation from proximal to distal. Like the Achilles tendon, this observation is consistent with our understanding of embryologic development of the limb (48). The surgical implication of this torsion is that the lateral fibers are attached to the medial cuneiform and are perhaps preferably severed for transfer in the split tibialis anterior tendon transfer procedure. This allows for improved alignment and line of force of the tendon. Detaching and transferring the fibers from the first metatarsal insertion may create an unwanted rotation of the proximal muscle belly.
Attachment to Bone
Tendons must both transmit and disperse enormous stresses that are applied through the corresponding muscle. The force is primarily dispersed by the relatively expansive nature of the tendon at its insertion. The deep fibers enter the bone at 90 degrees and attach by means of a gradual transition through four layers. This transition proceeds from tendon collagen fibers to fibrocartilage, which becomes calcified and then organized into bone (49,50,51 and 52). Indirect insertions consist mostly of superficial fibers that insert at acute angles into the periosteum. Sharpey fibers, which are collagen fibers originating in bone and terminating in the periosteum, may also be involved in securing the indirect insertions (31,52). However, these are not the fibers primarily responsible for the direct attachment of tendon to bone (50,53).
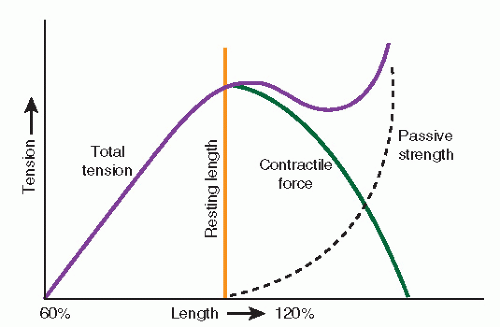
Figure 76.8 Contractile force curve as devised by Blix. The actual contractile force of a muscle is greatest at about 120% of its resting length. Tension falls off markedly in both directions, indicating that muscle must have optimum length for function and that deviations from this length in either direction will reduce the contractile force of a muscle. (Adapted from Bechtol CO. Muscle physiology. Instr Course Lect 1948;5:181.)
TENDON HEALING
Process
The goal of tendon healing is to produce an anastomosis of great tensile strength while providing unrestricted gliding function (54). Research has shown that the epitenon is the most proliferative structure in the tendon repair process. It produces the majority of type I collagen at the repair site in the first 2 weeks (55). Epitenon cells are also thought to be the primary source of differentiated fibroblasts (56). After a short delay period, the epitenon is augmented by the endotenon and interfascicular vessels. However, the tendon sheath contributes little, if anything, to tendon repair. Even with complete sheath excision, tendon function remains intact as a new sheath develops and adhesion formation is minimal (57,58).
The origin of the fibroblast necessary for repair remains controversial. Lindsay and Thomson (57) and Lindsay and Birch (59) refined the peripheral healing theory of extrinsic processes. They believed that all connective tissue cells supporting a tendon are capable of producing the fibroblasts that will migrate into the tendon callus. Those in the less specialized tissues, the epitenon and endotenon, tend to react earlier. This theory was also advocated by Potenza (60) and Matthews and Richards (61), who concluded that tendon healing also requires the development of scars as a source of vascularity and fibroblasts necessary for collagen synthesis.
Using radioactive labeling and other techniques, researchers have been able to show that the tendon cells, or tenocytes, have the capability of producing cells and collagen for intrinsic tendon repair (32,39,40 and 41,61,62 and 63). It is evident that both intrinsic and extrinsic processes have important roles in tendon healing. The degree of contribution from each is dependent on the extent of local damage and the quality of the repair (64).
In summary, the integrity of the peritendinous structures is of paramount importance for healing success. Proliferative reparative processes are much more efficient when healing occurs within paratenon as opposed to within a synovial sheath. Whenever possible, tendon procedures should be performed in areas where paratenon is present because the resultant scar will be able to glide with the areolar tissue of the paratenon, as well as the tendon itself.
When a tendon is separated from its normal surrounding structures, disturbances in nutrition and adhesion formation may lead to surgical failure. A tendon should not be stripped of paratenon in the process of transposition. For optimal healing, all the necessary peritendinous tissues should accompany the tendon with a minimal amount of trauma during the transfer procedure for optimal healing (12).
Chronology
When severed tendons are reapproximated end to end and maintained with suture, the healing process is one of progressive fibrosis and reconstitution of the tendon (cicatrization and tendonization) (65). The changes in tensile strength conform to the histologic phases during the process of repair. The stages of tendon healing are (a) the initial inflammatory (exudative) phase, (b) the fibroblastic (formative) phase, and (c) the remodeling (organizational) phase of maturation and differentiation. The first phase takes about 48 to 72 hours, whereas the second phase begins at approximately 5 days, inasmuch as collagen fibers are formed in a random disorganized pattern. Fibroplasia predominates by the 10th day as the increased collagen and fibroblasts are oriented perpendicular to the long axis of the tendon. The third phase begins gradually from 15 to 28 days as the new collagen begins to align itself with the tendon (61,64,66,67).
It takes about 4 weeks before healing is sufficient after tendon repair to allow a gradual return to activity, although passive motion may be started after the 3rd week. The histologic stages tend to overlap and vary with the individual’s physiologic response and ability to generate collagen, but generally, patients progress through the chronology presented in the following sections (1,3,57,61,66,68).
Week One.
During the 1st week, there is a reactive process whereby the tendon ends retract and become red and swollen with increased vascularity. An inflammatory cell exudate accumulates in the perisheath tissue and gap zone to form a jellylike bridge of serous and granulation tissue called a fibroblastic splint or tendon callus. Indeed, in 48 hours, there is a vigorous fibroblastic proliferation and migration from the epitenon, mesotenon, and paratenon. Two days later, the cells of the endotenon, followed by the tenocytes themselves, contribute to this proliferative cellular response. Initially, the cells have a phagocytic function to clean up debris. At this stage, sutures have reduced holding power in the softened tendon and may easily pull out.
Week Two.
During this week, the vascularity of the paratenon increases, as does the redness and edema of the tendon ends. Fibroblastic cells continue to proliferate into the amorphous mass to bridge the gap zone within 10 to 14 days. Still, there is no tensile strength and rupture may occur easily, although muscle tone is probably helping to stimulate repair. Active function of the tendon during the first 15 days will cause further irritation and swelling of the tendon, resulting in more adhesions, not a stronger union.
Week Three.
Now there is a vigorous production of collagen fibers that coalesce and begin to align themselves longitudinally to form new tendon fibers across the gap. The juncture is firmer, and cleavage begins between the tendon and surrounding tissue in preparation for movement. A moderate degree of bone strength is now present. Gentle mobilization after the 3rd week increases the strength of the union and discourages adhesion formation.
Week Four.
During the phase of resolution, the swelling and vascularity are reduced. The tendon continues to be loosened from surrounding tissues to increase gliding function. Applied force through passive motion and muscle contraction will stimulate the collagen fibers into parallel formation so as to give optimum strength to the union. There should be only a progressive or gradual return to maximum contracture at this stage because complete strength has not yet been fully restored.
Gradually, the amount of collagen in the healing area diminishes as the remaining fibers establish a longitudinal orientation, maturing by about 8 weeks. Tissue strength increases with the development of multiple cross-linkages, and as the tendon is stressed, tensile strength increases (69,70). After 20 weeks, there is minimal histologic difference compared with normal tendon (58). Adhesions are either weakened or lysed as the gliding mechanism is restored or, if they are fixed, they contract and restrict motion.
Progressive Strength of the Healing Tendon
This chronology will help in judging how long to immobilize a tendon after repair. Immediately after the surgery, the strength of the union is no greater than that of the suture material. After 2 weeks, the suture can withstand little strain. Limited isometric or passive range-of-motion exercises can be initiated after the 3rd week as the union increases in strength. When 4 weeks have passed, the need for further immobilization is reduced because the danger of rupture is greatly lessened. A gradual return to full function is advised (Table 76.2) (71).
Augmenting Tendon Healing
Tendon healing and strength recovery can be augmented through several methods including early mobilization, ultrasound, electrical stimulation, and growth factors. Early tendon motion is probably the most effective adjunct for enhancing tendon repair. Early controlled tendon loading and mobilization helps align repair cells and collagen matrix parallel to the line of tension, thereby increasing strength (72,73). Conversely, repair tissue of immobilized tendon is arranged randomly, creating a weaker union. One study demonstrated that 3 weeks after surgical repair, immobilized tendon is only half as strong as mobilized tendon (74). Often, the concern is not whether to mobilize tendon but rather determining the optimal amount of motion.
TABLE 76.2 Summary of Chronology of Tendon Healing
Time
Histologic Process
Strength
Treatment
Week 1
Softening. Production of jelly-like “fibroblastic splint”
Suture
Immobilize
Week 2
Increased vascularity and proliferation of fibroblasts
Suture
Immobilize
Week 3
Vigorous production of collagen fibers
Moderate bond strength
Gentle motion or isometric exercises
Week 4
Collagen fiber alignment; cleavage from local tissues
Gradual return to not quite full strength
Progressive muscular force
Undoubtedly, too much tendon motion or loading is detrimental and may disrupt healing tendon. The careful application of early tendon motion considers the type of injury, the strength of repair, and type of patient (72). Generally, when the suture repair is considered sufficient, passive motion may be initiated between 1 and 2 weeks postoperatively. Otherwise, passive motion may be started by 3 weeks (75).
Therapeutic ultrasound and electrical stimulation also have been shown to augment tendon healing (76). Ultrasound treatment of healing tendon has generated significant increases in tensile strength (77), with one study reporting an increased tensile strength up to 65% when compared with the control tendon (78).
Electrical stimulation induces new collagen production in tendon by mechanically loading the limb (76). Animal studies and in vitro studies of cultured tenocytes support the use of electrical stimulation in tendon healing; however, human clinical studies are needed (56,79).
Another developing area of tendon healing involves growth factors. Several growth factors have been identified in healing tendon, of which insulin-like growth factor-I (ILGF-I) appears to be the most important (80,81 and 82). ILGF-I stimulates collagen synthesis in tendon; however, human clinical applications have not yet been developed.
Factors Affecting Adhesion Formation
It would greatly simplify clinical practice if tendons could heal in isolation, but they do not. The healing process was placed in perspective by the “one wound—one scar” concept advocated by Peacock who, with Van Winkle (83,84), showed that each structure in the wound is connected with all others during healing, permeated by a single viscous gel. Thus, the surrounding tissue heals in conjunction with tendon healing, and connections are necessary to revascularize the tendon repair. Initially, by the 6th to 8th day, the normal vascular anatomy is replaced by a haphazard arrangement of multiple small vessels with frequent anastomoses (12). During the resolution stage of healing, the vascular pattern resumes a more normal configuration, and by 8 weeks, the longitudinal supply has been reestablished (85).
Thus, adhesions are not necessarily a complication of surgery in themselves. They are indeed an integral part of the healing process (86). However, additional factors have been shown to influence proliferation of excess adhesions that impede tendon function.
Matthews and Richards (87) studied the effects of immobilization, suture, and sheath excision during tendon healing and monitored for adhesion formation. The results indicated that all three factors work in concert to contribute to adhesion formation rather than just one factor being solely responsible. Sutures produced the most adhesions, although at times none formed. The constriction and trauma created by sutures tends to devitalize the enclosed tendon, with fibrous proliferation occurring throughout the sutured area and not just the stump region. Immobilization alone does not evoke the development of adhesions. Excision of the sheath results in repair through the formation of granulation tissue, but this tissue does not contribute to, nor interfere with, the healing of tendon. The synovial layers are subsequently regenerated. Other authors have shown that adhesions will form at every point of trauma to the tendon (12,88,89). Scar tissue will also form wherever blood is left to clot and organize (90).
As described previously, healing is most satisfactory when it occurs within the paratenon. Here, the possibility of adhesion formation is diminished. When transferred, the paratenon should accompany the tendon only in small amounts. A thin film will allow the scar tissue to remodel so that it has the same characteristics as normal paratenon (54). If large amounts of paratenon are transferred, dense restrictive scar tissue may be produced. When scar conditions are already present, autogenous paratenon or thin Silastic sheets (0.13 mm) can be interposed between the tendon and skin to prevent adhesion formation (91,92).
Finally, the epitenon should never be stripped from the tendon unless scar tissue formation is desired, as in side-to-side anastomosis. Ober (15) showed that the best way to restore and maintain gliding function is to pass the transferred tendon down the compartment of the paralyzed tendon. If necessary, the paralyzed tendon can be withdrawn. Early, protected motion will help diminish the formation of restrictive adhesions during tendon healing (64).
MUSCLE-TENDON PHYSIOLOGY
TENDON FUNCTION
Definition and Function
A tendon is a nonelastic structure suitable for transferring large tensile forces produced by the contraction of muscle so that distant movement can occur about joint axes. It requires smooth gliding along its course and flexibility of associated joints to function properly.
Duchenne made the cogent observation early in his studies that the isolated action of any muscle is not physiologic. Instead, each muscle works in concert with and is affected by other muscles or groups of muscles either synergistically or antagonistically. For example, muscle tone is required to maintain an extremity in its normal position at rest using these same subtle forces. Therefore, just as paralysis or loss of any single muscle must adversely affect others, similarly the selection of a muscle for transfer must be weighed for benefits with an understanding of the potential effects of the loss.
Concept of Tension
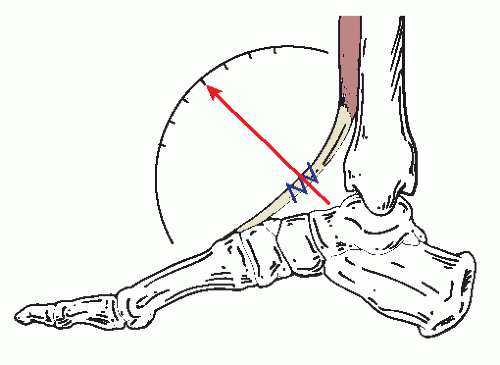
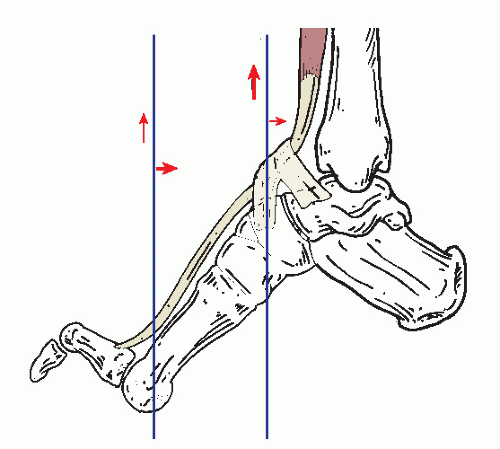
Blix (94) established that there exists a muscular length at which its contractile force is the strongest and most efficient. Thus, the degree of tension developed by the muscle is directly related to the length of the muscle at the time of contraction (Fig. 76.8) (4,93,94 and 95). Muscles tend to produce their greatest force at about 120% of their resting length (see the section on tension curve). Therefore, it is important to reestablish normal muscle tension in the transfer of a musculotendinous unit, which is accomplished by maintaining the physiologic length, a term coined by Stoffel (93,94 and 95). As Mayer (4) pointed out, based on his findings, this is done surgically by approximating the origin and insertion of a muscle—placing the foot in the position produced by maximal contraction of the transfer—and then removing all the slack from the tendon. By definition, zero tension is achieved when the patient is relaxed through general anesthesia. In other words, if the tendon were severed while in this position, the two ends would not separate. Using the tibialis anterior as an example, when the foot is placed in maximum dorsiflexion and moderate inversion, the tension on the tendon would be zero (Fig. 76.9).
Figure 76.9 Determining zero tension for transferred tendons. Essentially, the foot is placed in the desired position for correction (usually by dorsiflexing the foot to a right angle on the leg). Then all slack is removed from tendon, and it is fixed in place with 0 pounds of tension. (Adapted from McGlamry ED, Butlin WE, Ruch JA. Treatment of forefoot equinus by tendon transpositions. J Am Podiatr Med Assoc 1975;65:872-888.)
Muscle tension decreases as the muscle cells shorten, from the maximum achieved at 120% of their resting length to zero tension when they reach 60% of their resting length.
Levers, fulcrums, and axes.
Fulcrums are available to increase the angle of application and to improve the efficiency of tendon function. The sesamoids are fulcrums for the flexor hallucis brevis, whereas the cuboid has the same function for the peroneus longus tendon.
The ratio of torque produced by the anterior and posterior leg muscles in controlling foot function is roughly 1:4, respectively. This discrepancy is offset by the long lever arm of the forefoot, which increases the force of the anterior leg muscles. Comparatively, the powerful triceps possesses a short lever arm through the posterior calcaneus.
The proximity of a tendon to a joint axis will determine whether its force is primarily stabilizing or rotary (Fig. 76.10). The cross-sectional mass will determine the strength of the force (96,97 and 98).
PHASE FUNCTION AND CONVERSION
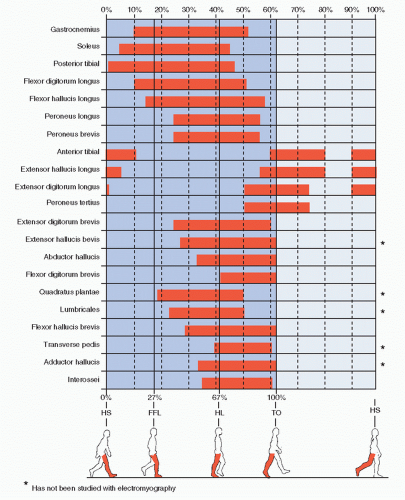
Muscles with insertions in the foot can be generally divided into swing-phase or stance-phase structures, depending on their function. For the most part, the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius are swing-phase muscles. The remainder are active during stance (Fig. 76.11).
In 1959, Close and Todd (99) evaluated the ability of transferred muscles to maintain or change phase, using electromyography (EMG) and cinematographic techniques. They found that muscles transferred to function in the same phase would rapidly regain their activity in as little as 7 or 8 weeks. Muscles transferred to function out of phase were generally unable to fire in their new position. However, such change in function was not entirely impossible. When transferred posteriorly into the calcaneus, the tibialis anterior showed activity in four of 13 patients. When the peroneus longus and brevis were studied after transfer to the dorsum of the foot, the brevis was shown to convert its function readily as early as 3 months after surgery, whereas the longus only rarely demonstrated complete functional conversion. When transferred to the dorsum of the foot, the tibialis posterior tendon for the most part retained its stance-phase activity (99). Other authors have also reported difficulty in educating the posterior tibial muscle to change phase (100). These authors also noted that when muscles were transferred to another phase, they were more likely to adapt than if they were transferred with additional muscles of the same phase.
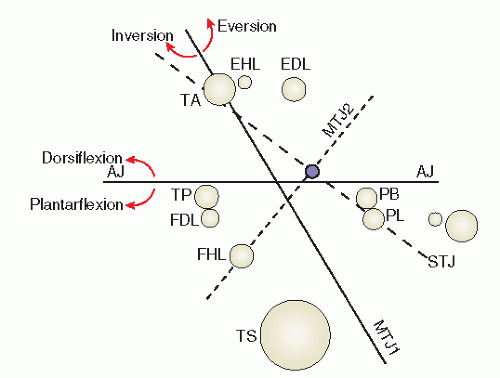
Figure 76.10 Cross section in the transverse plane through the ankle joint showing the relationship of various tendons with axes of ankle (AJ), subtalar (STJ), and midtarsal joints (MTJ). Tendons are identified by letters representing their corresponding muscles. EDL, extensor digitorum longus; EHL, extensor hallucis longus; FHL, flexor hallucis longus; PB, peroneus brevis; PL, peroneus longus; TA, tibialis anterior; TS, triceps surae; TP, tibialis posterior. (Adapted from Elftman H. Dynamic structure of the human foot. Artif Limbs 1969;13:49-58.)
Clinical experience has shown that it is more important to obtain a functional conversion than a phase conversion of a muscle, particularly when treating dropfoot. For example, even though the transferred tibialis posterior muscle might not fully convert in gait, it can still be trained to fire voluntarily at its new location in all but the most resistant patients. Even without functional conversion, such a tendon transfer can eliminate the need for a dropfoot brace because of the resting tone of the muscle will still provide a stabilizing effect. Active tenodesis can work as a rein or sling to hold the foot and ankle in a neutral position, somewhat like a bridle.
With the development and refining of techniques in biofeedback and EMG, the retraining of muscles has improved dramatically (94,95). Even changing phases can be more readily accomplished. However, it requires close cooperation with rehabilitation specialists for intensive conversion training. By teaching the patient how to isolate the desired motor activity before surgery, less difficulty may be encountered in learning how to control and use the motor unit voluntarily postoperatively.
OBJECTIVES OF TENDON TRANSFERS
The goals of tendon transfers about the foot and ankle are primarily to provide active motor power where it has been lost and thereby restore function or balance, or both. To provide such motion, surgery must be performed in an environment of flexible joints, unimpeded by contractures or osseous deformities. The goals are as follows:
To improve motor function where weakness and imbalance exist and thereby prevent contractures and further deformity
To eliminate deforming forces
To provide active motor power for restoration of a lost essential motor function
To produce better stability by establishing better muscle balance
To eliminate the need for bracing
To improve cosmetic appearance
MUSCULAR DYNAMICS OF THE FOOT
To appreciate deformity and tendon imbalance, it is necessary to understand muscle function as it affects the foot, whether intrinsic or extrinsic in its origin. The biomechanics of each individual muscle must of course be a part of that basic knowledge. However, as shown with such vivid insight by Duchenne in his 1867 monumental study entitled Physiology of Motion, the isolated action of muscles is not physiologic. Using faradic stimulation, coupled with his own astute clinical observations, Duchenne accurately demonstrated the concept of synergistic function of muscle groups. In addition, he described the concept of multiple muscle tone maintaining an extremity in a normal position at rest as “so many springs which act to maintain the position of an extremity.” When one spring is weakened or paralyzed, the stage is set for imbalance and abnormal position because of the pull or the tone of those remaining (101).
It is not the purpose of this chapter to describe in detail the function of each muscle. Although this detailed knowledge is important when clinical decisions are being made, this chapter will focus on a more general appreciation of the muscles used in the gross motions of the foot and specific knowledge of the major agonists or antagonists of each group. From this perspective, deformities may be understood and appropriate muscle and tendon units selected for transfer.
A highly useful tool in the biomechanical and neurologic evaluation of the patient is the standardized manual muscle testing described by Daniels and Worthingham (102), which uses a grading system for strength. Each muscle, placed at its end range of motion, is tested by applying manual force against it. The patient will best comprehend the test if the foot is placed with the desired muscle under maximum contraction and the patient is asked to hold it against the examiner’s resistance. If considerable force is required to break the muscle, it is graded at five or normal. Grades then descend with appropriate reductions in strength (Table 76.3). On the basis of the examiner’s experience, plus or minus may be used when the muscle test falls slightly above or below any one grade.
Figure 76.11 Phasic activity of muscles controlling the foot during normal gait. FFL, forefoot loading; HL, heel lift; HS, heel strike; TO, toe off. (Adapted from Root ML, Orien WP, Weed JH. Normal and abnormal function of the foot. Clinical biomechanics, vol II. Los Angeles, CA: Clinical Biomechanics Corp., 1977.)
Cinematographic gait studies, particularly when obtained with a high-speed camera that will allow detailed slow motion, may be valuable in appreciating muscle imbalance and functional deficits or compensation. Instant videotape systems may also be used with some sacrifice of detail.
Finally, EMG studies can provide detailed information about a muscle. An experienced examiner can determine roughly what percentage of the motor units are still functional. Also, the nature and often the stage of degeneration through which a muscle is passing may be assessed by analyzing the electrical activity within its fibers (102,103,104,105,106 and 107). Kinetic or dynamic EMG may be used to determine phase function activity (108,109).
TABLE 76.3 Grading System for Manual Muscle
Testing
Grade Description
5, Normal
Full resistance at end range of motion
4, Good
Some resistance at end range of motion
4+
Moderate resistance at end range of motion
4-
Mild resistance at end range of motion
3, Fair
Able to move against gravity alone
2, Poor
Able to move with gravity eliminated
1, Trace
Can palpate or visualize muscle contraction
0, Zero
No evidence of muscle contraction
PRINCIPLES OF TENDON TRANSFER SURGERY
As tendon surgery has been refined over the last century, specific principles have evolved, the goal of which is to obtain optimum function. Several authors have clarified these principles so they may be applied universally, whatever the nature of the particular tendon surgery proposed (3,6,8,13,15,110,111 and 112).
SELECTING SUITABLE PATIENTS
A necessary consideration in selecting a patient for a tendon transfer is the potential for rehabilitation. The nature of the disease, the mental capacity of the patient, and the attitude toward the proposed operation all enter into the decisionmaking process, even for children and parents. The cause of the patient’s disability must be analyzed in terms of its progressive nature, spasticity, flaccidity, and flexibility, as well as the remaining strength of the muscle. The transfer must be considered in relation to the total plan for rehabilitation of the patient.
In reviewing these factors, it is also important for the surgeon and the patient to be realistic in determining and understanding the goal of the proposed muscle-tendon transfer. A loss of one grade of muscle strength may be associated with many tendon transfers, and the patient or parents should be made aware of this factor in advance. However, most often, it is impossible to detect any loss, and often there appears to be a gain in strength. This occurs because of the change in leverage made possible with many transfers.
UNDERSTANDING ANATOMY AND PHYSIOLOGY INVOLVED
Paramount to preoperative planning is a thorough knowledge of the anatomy, pathology, and altered function of the involved area. The anatomy should be reviewed, and the examination should include manual muscle testing and a neurologic evaluation. Gait analysis will help one to appreciate the pathomechanics involved. The examiner may need to reevaluate the patient on several different occasions if he or she is unsure of the accuracy of findings. Cinematographic studies are an asset, particularly when slow motion is used for visual analysis. This is becoming more universally available with the affordability of more sophisticated modern video systems.
EVALUATING THE LOCAL TISSUES FOR SUPPLENESS
The tissues in the area of the transfer must be healthy. Severe scarring or scarring with concomitant tissue loss from previous trauma will not allow free tendon movement and may even result in further scar formation if surgery is attempted. Partialand full-thickness burns tend to damage tendons in the area, leaving them indurated and often bound to the surrounding tissues.
CORRECTING FIXED OR STRUCTURAL DEFORMITIES FIRST
Tendon transfer cannot be expected to overcome a fixed deformity. For a transferred tendon to be effective, the functional defect or deformity must be entirely flexible. In other words, the associated joint should demonstrate a reasonable range of passive motion. If a concurrent deformity is fixed, whether structural or as a contracture, it must be corrected at a prior surgery or at the same operation, provided it is done before the tendon is transplanted. Such fixed deformities can be altered by joint releases, tendon lengthenings, osteotomies, and arthrodeses.
SELECTING PROPER TIME FOR TRANSFER
Timing refers to the age of the patient and the course of the disease. Age is important if osseous stabilizing operations, which require adequate mature bone stock, are considered. However, it is not necessarily wise to delay tendon transfers several years if there exists a dynamic muscular imbalance, especially in younger patients who require or who resist brace protection. Early tendon surgery will prevent further deformity, thus facilitating the performance of future operations.
Although it is preferable for a pediatric patient to be old enough to cooperate in the retraining process, this is not always necessary. For example, in the dynamic and progressive talipes calcaneus deformity, early transfer can often arrest the progress of the deformity, even though the patient may not fully understand the new function of the muscle (113,114 and 115).
Timing during the disease process is most important when the condition is of a progressive nature. When there is brain damage, surgery should be delayed until the most intense stage of spasm has passed. Other disorders have individual times suitable for tendon transfer that vary according to their nature (Table 76.4).
SELECTING THE SUITABLE TENDON OR TENDONS
An initial consideration is whether there is sufficient power in the remaining muscles to provide adequate function once the desired tendon is harvested. In other words, is the muscle to be transferred truly expendable? It is also important to be realistic about the muscle’s capability—its strength and adaptability—to perform its new function. Strength can be approximately assessed by estimating the cross-sectional mass of the muscle itself. Table 76.4 supplies helpful information for the selection of tendons of sufficient capability.
Choosing muscles that are functionally similar (i.e., stabilizers vs. accelerators) or within the same phase (i.e., stance or swing) is ideal but not absolute. In electing to use a muscle of the opposite phase, it is better to select one that has a high potential for conversion (e.g., the peroneus brevis).
TABLE 76.4 Timing of Tendon Transfers in Certain Diseases
Disease
Suggested timing
Author
CVA
6 mo
Edmonson and Crenshaw, 1980
Cerebral palsy
1 y old—tendon lengthenings
Goldner, 1971
4 y old—tendon transfers
Brain injury (children)
1 y old
Samilson, 1976
2 y old
Hoffer et al., 1974
Lower level
6 mo to 8 y old
Janda et al., 1984
Spinal dysplasia (e.g., myelomeningocele)
After 9 mo
Edmonson and Crenshaw, 1980
Poliomyelitis
2-3 y after acute onset (during the early residual stage)
Peabody, 1949
Edmonson and Crenshaw, 1980
Better over 10 y old
Charcot-Marie-Tooth disease
Variable because of different ages of onset
Leprosy
6 mo after onset of palsy (arm)
Brandsma and Lijftogt, 1983
1 y after onset of palsy (dropfoot)
Muscular dystrophy
Variable because different ages of onset
In regressive neuromuscular conditions such as Charcot-Marie-Tooth disease, the potential for future deterioration of the muscle to be transferred must be as accurately ascertained as possible. Even if only several years of function remain, it can still serve to delay disability.
PROVIDING DIRECT OR MECHANICALLY EFFICIENT LINE OF PULL
The individual fibers of a muscle are set and arranged according to the optimal line of function. When this line of application is altered, the muscle must undergo a certain amount of readjustment. The more the line of pull is changed, the greater the demand on the muscle for adaptability, of which there is a definite limit (116).
Maximum physiologic efficiency is obtained when a tendon pulls in a straight line. Therefore, changes in the direction of tendon contraction, that is, retinacula, reduce the maximal effectiveness of the muscle. When tendons are transferred, angulations should be avoided as much as possible because any degree of angulation will cause a loss of amplitude. Despite these considerations, it is usually preferable to transfer the tendon along an anatomic course. Transferring the tendon subcutaneously will enhance its power but will result in bowstringing against the skin and also introduces an unpredictable degree of torsion against the involved joints.
In addition, as the lever arm increases, the force vectors change in amplitude. Generally, the longer the lever arm, the more effective the muscular force. However, if the line of contracture is parallel to the lever, then additional length will have little effect. A good example is a tendon transfer to the dorsum of the foot beneath the extensor retinaculum (Fig. 76.12). Extensor tendons that are transferred to a more proximal location on the foot have a more effective force of ankle dorsiflexion compared with the distal metatarsophalangeal location.
PERFORMING STABILIZATION PROCEDURES IF NECESSARY
Tendon transfers require rigid lever arms on which to function, regardless of their distance from the joint axes. When such stability is not present, then it must be constructed by way of arthrodeses, regardless of whether in the toes or the tarsus. Stabilization procedures must be performed before the tendon transfer, either at a prior surgery or during the same operation.
Figure 76.12 Vector of force of the effective lever arm of tendon. Arrows indicate the relative direction and amount of force of tendons transposed at different levels. A more proximal transfer of the insertion enhances available dorsiflexory power. With a more distal insertion, the line of pull tends to parallel the lever arm, and the mechanical advantage of dorsiflexion is lost. (Adapted from McGlamry ED, Butlin WE, Ruch JA. Treatment of forefoot equinus by tendon transpositions. J Am Podiatr Med Assoc 1975;65:872-888.)
PRESERVING THE GLIDING MECHANISM
The most perplexing problem in tendon transfer surgery has been that of adhesions restricting function. All major tendon surgeons agree that the only satisfactory way to prevent adhesions is to preserve or reconstruct the physiologic gliding mechanism of the tendon. This is best accomplished through absolute atraumatic surgery, restoration of the tendon-sheath relationship, and use of existing sheaths or establishment of a subcutaneous tunnel. If possible, the peritendinous structures, especially small amounts of the paratenon, should be transferred with the tendon.
Retention of the physiologic relationship between the tendon and sheath can be obtained by passing the transferred tendon within the sheath of the paralyzed tendon. When this is not possible, a gliding channel can be fashioned within subcutaneous adipose tissue by establishing a channel with forceps or other blunt instruments. The channel will eventually be lined with smooth cells to permit gliding of the tendon. Early protective mobilization exercises will help restore the gliding mechanism (117). Ultimately, the transferred tendon should have similar excursion to the one it replaces.
USING ATRAUMATIC TECHNIQUE AT ALL TIMES
The principle of atraumatic technique was first proposed and the term coined by Bunnell (118) in 1918. Atraumatic technique is the central factor that contributes to preservation of the gliding function of the transferred tendon, reiterated time and again by many authors. Although it is a term heard often by the reconstructive surgeon, several aspects apply especially to tendon surgery.
Atraumatic technique begins with the incision. It should not be placed directly over the tendon itself and, when practical, should parallel local skin creases to minimize the development of thick, nonpliable cicatrix. Careful planning will allow the operation to be performed precisely yet as quickly as possible, exposing tissues to air for the shortest period possible. Absolute hemostasis is essential. An adhesion can often form at every place a small clot of blood is allowed to remain. Thus, the wound should be irrigated frequently and liberally, preferably with Ringer solution, not only to keep the tissues moist but also to remove blood clots and other tissue debris that might adversely affect the healing process. Tissues must not be torn or crushed, except for the tendon end that is to be fixated and where fibrous production is desired.
Any damage to the gliding surface of the tendon, covered with smooth delicate cells, will readily cause adhesions to form. The tendon to be moved should be left in place until its new course and insertion are made ready to receive it. It should be manipulated very gently, using toothless forceps, Penrose drains, or a wet gloved hand. Even a moistened sponge can be too rough. The paratenon and epitenon should be left intact and transferred with the tendon, which should be kept moist at all times. The tendon should never be allowed to lie on the local drapes. Mesotenon, when present, should be sharply and gently extricated.
PRESERVING BLOOD SUPPLY AND INNERVATION
Sometimes, considerable traction is required to harvest a tendon for transfer. If this is excessive, the nerve supply to the tendon can pull free. Similarly, rough handling or indiscriminate dissection may lacerate the main blood vessel of the tendon, usually found running in the lower muscle fibers. Smaller vessels running in the mesotenon can be divided with impunity.
PROVIDING ADEQUATE MUSCLE-TENDON TENSION ON FIXATION
The concept of zero tension has already been described. Whereas too little tension will cause the muscle to shorten, leaving a loss of power, the strain of excess tension will cause rapid degeneration of the muscle tissue over a period of only weeks (5,9). The goal is to establish tension that corresponds to the normal physiologic conditions under which the muscle and tendon work. In other words, the physiologic length of the muscle must be maintained. Yet, no matter how well the technique is described, fastening a tendon under zero tension is a skill that each surgeon develops with experience because it varies from one muscle to another.
Using Secure Fixation Techniques
A tendon transfer is only as good as the security of its point of fixation. The first recorded effort by Nicoladoni (3,5,6,7,8,9 and 10) failed because the tendon pulled free, leaving other surgeons skeptical of the procedure. Ideally, the tendon should be secured as close as possible to the insertion of the paralyzed tendon. If this is not feasible, then consideration must be given to a location in which leverage will provide sufficient power and balance. When a tendon is split to balance its pulling force, care must be taken to fixate each branch under equal tension. If unbalanced, the resulting motion will go to the tightest branch.
Tendon may be attached in one of three ways: tendon to tendon, tendon to periosteum, or tendon to bone. The tendon-to-bone attachment provides the most secure fixation. Specific techniques will be described for each of these methods.
Providing Detailed Postoperative Management
Postoperative care is crucial to a successful outcome. It is vital that the patient and, when necessary, the parents understand the requirements of immobilization, convalescence, and rehabilitation following tendon transfer surgery. The cast should be applied at the time of surgery, if possible. Manipulation during dressing changes or cast applications early in the healing period may cause the tendon to pull free.
Motion may be started early, as soon as the surgeon is reasonably certain that healing has provided firm anchorage of the tendon. Gentle isometric exercises within the cast can be started as early as 3 weeks.
The rehabilitation program should begin with strengthening exercises immediately after removal of the cast. Then retraining the muscle to contract appropriately in its new location becomes the goal of therapy. If phasic conversion is required, intense training must be accompanied by rehabilitation techniques. These methods will be detailed later.
Fixation of Transferred Tendons
Tendon to Tendon.
Side-to-side anastomosis of a transferred tendon provides the most physiologic pull; the greatest danger in such attachment is that of slippage. The adjoining surfaces should be roughened and the epitenon scraped free. Scarring the tendons with light cross-hatching will also encourage fibrous union (Fig. 76.13). Polygalactic or polyglycolic acid sutures provide sufficient strength for sewing tendons, but they may be reinforced with a nonabsorbable polyester suture to increase strength over time as the former are absorbed.
Figure 76.13 Suture technique for side-to-side anastomosis.
Tendon to Bone.
Several techniques can be used to anchor tendon into bone. Regardless of the method, healing will occur similarly with the tendon actually being incorporated into the bone by ossification (119,120). The osseous healing process and strength of attachment is the same whether the tendon is placed in cortical or cancellous bone (121). The limb must be immobilized during the early phase but not for longer than necessary. Twenty-one days may be all that is required. Prolonged immobilization may retard the tensile strength of the union. The relative size of the tendon to drill hole has little effect on the rate of union of tendon to bone.
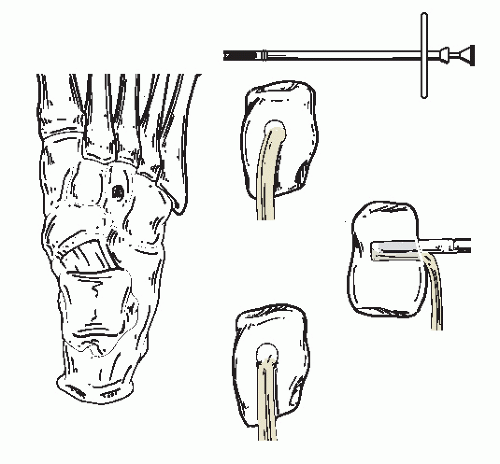
Trephine plug.
Michele vertebral trephines are ideal hand instruments. A hole is created, and the plug of bone preserved for future replacement (Fig. 76.14) (122). Power trephines can also be used. The tendon end is inserted into the hole, and the plug is tapped into place. Anchor sutures are then placed in the surrounding fascia and periosteum. In the absence of a trephine, a cortical window may be fashioned with use of osteotomes or a drill.
Chinese finger trap suture.
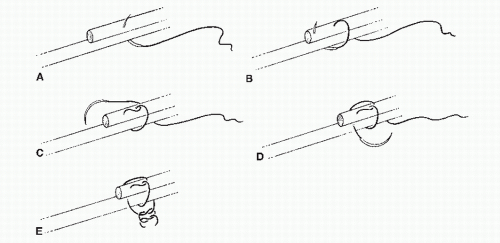
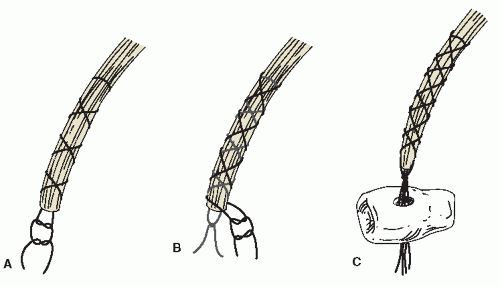
This technique facilitates the drawing of a tendon through a drill hole (123). A polyester suture (1-0 or 2-0) is wrapped around the tendon in a crisscross fashion proceeding from about 3 or 4 cm to the end. A knot is tied and the suture tails left long. A second suture is then wrapped in crisscross fashion around the tendon, out of phase with the first suture, and tied in a knot at the end. The ends of the suture are then passed through the drill hole to draw the tendon through. Finally, the sutures are cut to relieve tension around the tendon (Fig. 76.15).
Three-hole suture.
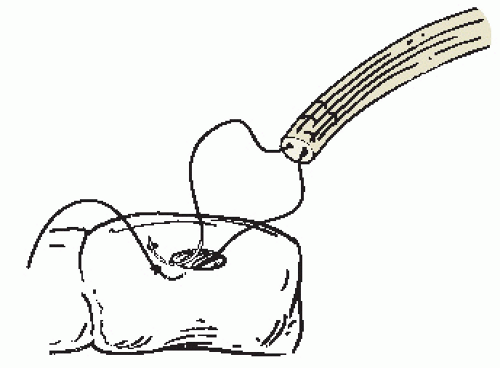
This technique consists of anchoring the transposed tendon end with a double-armed suture, then placing it into one large drill hole. It is secured by drawing the suture ends out through two small adjacent drill holes and tying them firmly. A nonabsorbable polyester suture is recommended (Fig. 76.16) (26).
Buttress and button anchor.
By this method, a bone hole is drilled for tenodesis at the desired site. The suture is anchored in the tendon, and one or two straight Keith needles are then passed through the drill hole and out the other side of the foot. A button provides the anchor on which to tie the suture ends, but a sterile buttress material, such as foam or gauze, must be interposed between the button and the skin to disperse the pressure and to avoid ischemic necrosis (Fig. 76.17).
Tunnel with sling.
Only when there is sufficient length of tendon available can this technique be used. It consists of drilling a hole completely through a bone and then passing the tendon all the way through so it can be sutured back on itself. In this manner, the tendon becomes something of a sling. It has its greatest application in the Jones first metatarsal tendon suspension (26,122) and in ankle stabilization procedures such as described by Watson-Jones (Fig. 76.18) (122).
Figure 76.14 Insertion of tendon into a trephined hole in bone. A Michele vertebral trephine or power trephine may be used.
Figure 76.15 Chinese finger trap suture. A: First crisscross suture. B: Second crisscross suture. C: The tendon is compressed as it is drawn through the drill hole in the bone.
Tendon with osseous insertion.
Instead of severing the tendon at its insertion, the portion of bone to which it is attached is carefully removed with an osteotome or power saw. The plug of bone is then inserted into the new site where a similarly sized piece of cortical bone has been removed. The main disadvantage is that adjustment of the tendon length for proper tension is extremely limited.
Screw and washer.
The use of a cleated polyacetyl washer and cancellous bone screw is a helpful method for securing a tendon at its new location. It is especially suited where there is little soft tissue to which the transferred tendon can be sutured or where other bone attachments are difficult. A good example is the anterior advancement of the posterior tibial tendon (Fig. 76.19).
Soft Tissue Anchors into Bone.
Bone anchors were first introduced in 1988 and have become valuable devices for reattaching soft tissue to bone. Prime indications in the foot and leg include rupture or reconstructive procedures involving tendons or ligaments. There are several anchors available that can be categorized as threaded, pronged, or absorbable-type anchors. Each allows attachment of a suture.
Figure 76.16 Three-hole suture technique for anchoring tendon to bone.
Threaded anchors are screwed into bone and then used to attach soft tissue to bone. Pronged anchors have laterally projecting tines that help prevent anchor pullout. Absorbable anchors vary in method of attachment to bone but generally are made of poly-L-lactide or polylactic acid.
Only gold members can continue reading. Log In or Register to continue