Posterior Interosseous Artery Island Flap for Dorsal Hand Coverage
Eduardo A. Zancolli
The posterior interosseous flap is an island pedicled fasciocutaneous flap from the dorsal aspect of the forearm supplied by the cutaneous branches of the posterior interosseous artery. The posterior interosseous artery is located in the septum between the extensor carpi ulnaris and the extensor indicis propius. This flap has proven to be an excellent coverage option for the dorsum of the hand and the first interdigital web. The dorsal cutaneous area of the forearm supplied by the posterior interosseous artery was initially described by Manchot in 1889 (8) and later by Salmon in 1936 (12).
The vascular anatomy of the flap was described along with 20 initial cases (17 cases to cover the first web and three cases to cover the dorsum of the hand). The dorsal cutaneous area of the forearm irrigated by the posterior interosseous artery was initially described by Manchot in 1889 (8) and later by Salmon in 1936 (12).
This island flap was presented for the first time by the author at the VIth European Hand Surgery Course in Ümea (Sweden) (13). In this opportunity the vascular anatomy of the flap and an experience on 20 initial cases were presented (17 cases to cover the first web and three cases to cover the dorsum of the hand). Hand outs distributed during the course were published by the author in 1993 (18). The procedure was also presented in the same year in the XI Congress of the Argentine Society for Surgery of the Hand (awarded with the “J. Goyena Prize”), in November 1985, Buenos Aires, Argentina (14). Other papers on the procedure were published by us in 1986 (15,16), 1988 (17) and 1993 (1,18). The vascular anatomy of the posterior interosseous island flap was presented by Penteado et al in 1986 (11), and other studies on the posterior interosseous flap have been published by Masquelet et al (9), Costa et al (3,4), Gilbert et al (7), Buchler et al (2), Dap et al (5), Mazzer et al (10), and Goubier et al (6). These studies have further supported the efficacy of the this flap.
Indications/Contraindications
The posterior interosseous artery island flap is capable of transporting the skin of the distal two-thirds of the forearm. The flap’s pedicle length determines its coverage possibilities.
It is particularly useful for covering extensive defects on the back of the hand as far distally as the dorsal aspect of the proximal phalanges of the fingers and for obtaining a complete coverage of the first web after the release of severe adduction contractures of the thumb. Buchler et al (2) noted that the flap could reach the dorsum of the proximal interphalangeal joints. It can be indicated in different
types of pathologies such as burn sequelae, wounds on the dorsum of the hand, tumors, and congenital deformities.
types of pathologies such as burn sequelae, wounds on the dorsum of the hand, tumors, and congenital deformities.
Contraindications for flap use include any injury to the posterior interosseous artery or deep laceration or crush wounds to the posterior forearm in the area of the flap pedicle. The flap is not recommended in patients with diabetes, in whom small vessels may be diseased. The flap has been used successfully in smokers, but smoking certainly carries a higher risk of flap complications.
Preoperative Planning
Successful flap harvest is predicated on a thorough knowledge of the flap anatomy. Normally the anterior and posterior interosseous arteries in their course through the forearm are united through two main anastomoses, one proximal, at the level of the distal border of the supinator muscle, and one distal at the most distal part of the interosseous space (2 cm proximally of the distal radioulnar joint) (Fig. 16-1). The island posterior interosseous island flap is supplied by the reverse arterial blood flow through the distal anastomosis once the proximal anastomosis has been ligated. Venous drainage is produced by the venae comitantes of the posterior interosseous artery.
The angiosomal territory of the posterior interosseous artery was studied in a series of 80 cadaveric forearms in 1993 (1). Ink injections performed through catheter placed in the distal part of the anterior interosseous artery stained the distal two-thirds of the posterior forearm skin through the reverse flow through the distal anastomosis. The proximal third of the forearm skin remained unstained even when larger amounts of ink were injected (see Fig. 16-5). Ink injections through the catheter placed in the proximal part of the posterior interosseous artery stained the proximal two-thirds of the posterior forearm through the direct flow through the proximal cutaneous branch (1).
Other anatomic conclusions from this study can be summarized as follows: the posterior interosseous artery usually branches from the common interosseous artery in the proximal third of the forearm in 90% of cases, it can however be a direct branch of the ulnar artery in 10% of cases (1). It pierces the interosseous membrane about 6 cm distal to the lateral epicondyle of the humerus (14,15,16,17,18) forming its origin or proximal anastomosis between the anterior and posterior interosseous arteries. It enters into the posterior compartment of the forearm below the distal edge of the supinator muscle, located at the union of the proximal with the distal two-thirds of the dorsal aspect of the forearm (60 mm distal to the lateral epicondyle). At its entrance into the posterior compartment of the forearm, the posterior interosseous artery gives off branches to the recurrent interosseous artery that anastomoses at the elbow with a descending branch from the superior profunda, with the posterior ulnar recurrent and the anastomotica magna. In its ascending course the artery runs between the lateral condyle and the olecranon (Figs. 16-1 and 16-2).
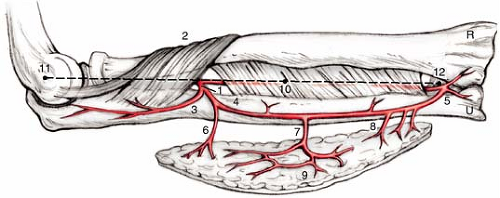 FIGURE 16-1 Anatomy of the posterior interosseous artery. (1) Proximal end of the posterior interosseous artery at the distal border of the supinator muscle. (2) The artery is emerging as a division of the common interosseous artery. (3) Recurrent interosseous artery. (4) Posterior interosseous artery following the longitudinal line X-X’, between the lateral epycondile (11) and the distal radio-ulnar joint (12). (5) Distal anastomosis between both interosseous arteries (2 cm proximal to the distal radio-ulnar joint). Cutaneous branches from the posterior intererosseous artery that irrigte the two distal thirds of the posterior skin of the forearm. Proximal (9
Get Clinical Tree app for offline access
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|





