Pelvis
EPIDEMIOLOGY
The incidence of pelvic fractures in the United States has been estimated to be 37 cases per 100,000 population per year.
In persons younger than 35 years, males sustain more pelvic fractures than females; in persons older than 35 years, women sustain more pelvic fractures than men.
Most pelvic fractures that occur in younger patients result from highenergy mechanisms, whereas pelvic fractures sustained in the elderly population occur from minimal trauma, such as a low fall.
ANATOMY
The pelvic ring is composed of the sacrum and two innominate bones joined anteriorly at the symphysis and posteriorly at the paired sacroiliac joints (Fig. 25.1A,B).
The innominate bone is formed at maturity by the fusion of three ossification centers: the ilium, the ischium, and the pubis through the triradiate cartilage at the dome of the acetabulum.
The pelvic brim is formed by the arcuate lines that join the sacral promontory posteriorly and the superior pubis anteriorly. Below this is the true or lesser pelvis in which are contained the pelvic viscera. Above this is the false or greater pelvis that represents the inferior aspect of the abdominal cavity.
Inherent stability of the pelvis is conferred by ligamentous structures. These may be divided into two groups according to the ligamentous attachments:
1. Sacrum to ilium: The strongest and most important ligamentous structures occur in the posterior aspect of the pelvis connecting the sacrum to the innominate bones.
The sacroiliac ligamentous complex is divided into posterior (short and long) and anterior ligaments. Posterior ligaments provide most of the stability.
The sacrotuberous ligament runs from the posterolateral aspect of the sacrum and the dorsal aspect of the posterior iliac spine to the ischial tuberosity. This ligament, in association with the posterior sacroiliac ligaments, is especially important in helping maintain vertical stability of the pelvis.
The sacrospinous ligament is triangular, running from the lateral margins of the sacrum and coccyx and inserting on the ischial spine. It is more important in maintaining rotational control of the pelvis if the posterior sacroiliac ligaments are intact.
2. Pubis to pubis: Symphyseal ligaments
Additional stability is conferred by ligamentous attachments between the lumbar spine and the pelvic ring:
1. The iliolumbar ligaments originate from the L4 and L5 transverse processes and insert on the posterior iliac crest.
2. The lumbosacral ligaments originate from the transverse process of L5 to the ala of the sacrum.
The transversely placed ligaments resist rotational forces and include the short posterior sacroiliac, anterior sacroiliac, iliolumbar, and sacrospinous ligaments.
The vertically placed ligaments resist shear forces (vertical shear, VS) and include the long posterior sacroiliac, sacrotuberous, and lateral lumbosacral ligaments.
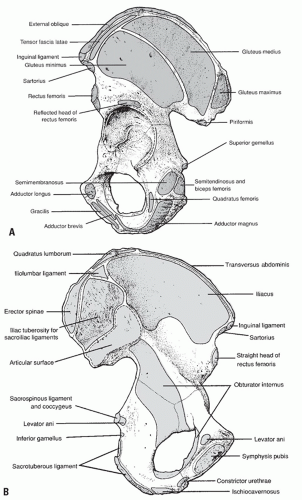 FIGURE 25.1 (A) Lateral projection of the left innominate bone. Note the muscular attachments to the ilium, ischium, and pubis. (B) Medial projection of the left innominate bone with muscle attachments and outline of the sacroiliac joint surface. (From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.) |
PELVIC STABILITY
A mechanically stable injury is defined as one that can withstand normal physiologic forces without abnormal deformation.
Penetrating trauma infrequently results in pelvic ring destabilization.
An unstable injury may be characterized by the type of displacement as:
Rotationally unstable (open and externally rotated, or compressed and internally rotated)
Vertically unstable
Sectioned ligaments of the pelvis determine relative contributions to pelvic stability (these included bony equivalents to ligamentous disruptions):
Symphysis alone: pubic diastasis <2.5 cm
Symphysis and sacrospinous ligaments: >2.5 cm of pubic diastasis (note that these are rotational movements and not vertical or posterior displacements)
Symphysis, sacrospinous, sacrotuberous, and posterior sacroiliac: unstable vertically, posteriorly, and rotationally
MECHANISM OF INJURY
These may be divided into low-energy injuries, which typically result in fractures of individual bones, or high-energy fractures, which may result in pelvic ring disruption.
Low-energy injuries may result from sudden muscular contractions in young athletes that cause an avulsion injury, a low energy fall, or a straddle-type injury (motorcycle or horse).
High-energy injuries typically result from a motor vehicle accident, pedestrian-struck mechanism, motorcycle accident, fall from heights, or crush mechanism.
Impact injuries result when a moving victim strikes a stationary object or vice versa. Direction, magnitude, and nature of the force all contribute to the type of fracture.
Crush injuries occur when a victim is trapped between the injurious force, such as motor vehicle, and an unyielding environment, such as the ground or pavement. In addition to those factors mentioned previously, the position of the victim, the duration of the crush, and whether the force was direct or a “rollover” (resulting in a changing force vector) are important to understanding the fracture pattern.
Specific injury patterns vary by the direction of force application:
1. Anteroposterior (AP) force (motorcycle crash)
This results in external rotation of the hemipelvis.
The pelvis springs open, hinging on the intact posterior ligaments.
2. Lateral compression (LC) force (fall onto side, “T-bone” in motor vehicle crash): This is most common and results in impaction of cancellous bone through the sacroiliac joint and sacrum. The injury pattern depends on location of force application:
Posterior half of the ilium: This is classic LC with minimal soft tissue disruption. This is often a stable configuration.
Anterior half of the iliac wing: This rotates the hemipelvis inward. It may disrupt the posterior sacroiliac ligamentous complex. If this force continues to push the hemipelvis across to the contralateral side, it will push the contralateral hemipelvis out into external rotation, producing LC on the ipsilateral side and an external rotation injury on the contralateral side.
Greater trochanteric region: This may be associated with a transverse acetabular fracture.
External rotation abduction force: This is common in motorcycle accidents.
Force application occurs through the femoral shafts and head when the leg is externally rotated and abducted.
This tends to tear the hemipelvis from the sacrum.
Shear force
This leads to a completely unstable fracture with triplanar instability secondary to disruption of the sacrospinous, sacrotuberous, and sacroiliac ligaments.
In the elderly individual, bone strength will be less than ligamentous strength and will fail first.
In a young individual, bone strength is greater and, thus, ligamentous disruptions usually occur.
CLINICAL EVALUATION
Perform patient primary assessment (ABCDE): airway, breathing, circulation, disability, and exposure. This should include a full trauma evaluation (see Chapter 2).
Identify all injuries to extremities and pelvis, with careful assessment of distal neurovascular status.
Pelvic instability may result in a leg-length discrepancy involving shortening on the involved side or a markedly internally or externally rotated lower extremity.
The AP-LC test for pelvic instability should be performed once only and involves rotating the pelvis internally and externally.
“The first clot is the best clot.” Once disrupted, subsequent thrombus formation of a retroperitoneal hemorrhage is difficult because of hemodilution by administered intravenous fluid and exhaustion of the body’s coagulation factors by the original thrombus.
Massive flank or buttock contusions and swelling with hemorrhage are indicative of significant bleeding.
Palpation of the posterior aspect of the pelvis may reveal a large hematoma, a defect representing the fracture, or a dislocation of the sacroiliac joint. Palpation of the symphysis may also reveal a defect.
The perineum must be carefully inspected for the presence of a lesion representing an open fracture.
Digital rectal in all and a vaginal exam in women should be performed in all trauma patients who present with a pelvic ring disruption. A missed rectal or vaginal perforation in association with a pelvic ring injury has a poor prognosis.
HEMODYNAMIC STATUS
Retroperitoneal hemorrhage may be associated with massive intravascular volume loss. The usual cause of retroperitoneal hemorrhage secondary to pelvic fracture is a disruption of the venous plexus in the posterior pelvis. It may also be caused by a large-vessel injury, such as external or internal iliac disruption. Large-vessel injury causes rapid, massive hemorrhage with frequent loss of the distal pulse and marked hemodynamic
instability. This often necessitates immediate surgical exploration to gain proximal control of the vessel before repair. The superior gluteal artery is occasionally injured and can be managed with rapid fluid resuscitation, appropriate stabilization of the pelvic ring, and embolization.
instability. This often necessitates immediate surgical exploration to gain proximal control of the vessel before repair. The superior gluteal artery is occasionally injured and can be managed with rapid fluid resuscitation, appropriate stabilization of the pelvic ring, and embolization.
Options for immediate hemorrhage control include:
1. Application of military antishock trousers (MAST). This is typically performed in the field.
2. Wrapping of a pelvic binder circumferentially around the pelvis (or sheet if a binder is not available) (Fig. 25.2). This should be applied at the level of the trochanters to provide access to the abdomen.
3. Consider application of a bean bag.
4. Consider angiography or embolization if the hemorrhage continues despite closing of the pelvic volume.
5. Consider application of a pelvic C-clamp (posterior).
6. Consider an anterior external fixator.
7. Open reduction and internal fixation (ORIF): This may be undertaken if the patient is undergoing emergency laparotomy for other indications; it is frequently contraindicated by itself because loss of the tamponade effect may encourage further hemorrhage.









