Fig. 18.1
Intermediate paraglider from 1987

Fig. 18.2
High-performance paraglider from 2012
18.2 Incidents and Injuries
Epidemiological data on injuries in paragliding are mainly from retrospective case series or cross-sectional studies: calculation of injury rates is difficult, since the precise number of paragliders is usually unknown. No studies on degenerative changes as a result of overuse are reported in paragliding, and all the available series are related to traumatic events [1–5]. A survey from Germany analyzed over 400 incidents over a period of 3 years and calculated yearly incident rates of licensed pilots of 0.58–1.01 %, severe injury rates of 0.32–0.5 %, and mortality rates of 0.03–0.06 %, all decreasing over time [6]. In Switzerland, 129 incidents were reported over 3 years, 9 were fatal incidents and 60 of those classified caused major injuries [7].
Incidents in paragliding most commonly occur as a consequence of deflation of the glider (32.5 %), oversteering (13.9 %), landing errors (13.7 %), collision with obstacles (12.0 %), and takeoff errors (10.3 %) [6]. Any disturbance of the chute’s profile results in a loss of height: if there is an adequate distance to the ground, such disturbances can be corrected by the pilot, and a stable forward motion can be obtained. A large unilateral collapse of the airframe results in a spin and helical flight path, a spiral dive where the vertical speed can easily reach 20 m/s (72 km/h). Due to the large pendulum of the pilot suspended 8 m below the wing, the centrifugal forces may accelerate the pilot to speeds of over 100 km/h. By vector addition, this results in velocities of over 120 km/h for the pilot relative to the land surface. An aerodynamic stall over the whole wingspread (e.g., abrupt braking maneuver) results in a nearly vertical plunge downward, with speeds of around 10 m/s. A unilateral aerodynamic stall leads to uncontrolled rotation around the vertical axis and downward velocities of around 6 m/s.
18.3 Acute Traumatic Injuries
Due to the sitting or semi-recumbent position in the harness (Figs. 18.3 and 18.4), the crashing pilot first impacts with his feet or buttocks.


Fig. 18.3
Recreational harness
Fig. 18.4
Competition harness with streamlined leg cover
Accordingly, most injuries are observed in the lower extremities and the trunk (pelvis and spine): fractures, dislocations, distortions, and strains of the lower extremities account for 27–46 % of these injuries, with injuries to the spine and trunk representing 31–60 % of all reported paragliding injuries [2–5, 8, 9].
In the spine, the most common injuries (50–91 %) are severe compression-type fractures, requiring surgical treatment in two-thirds of patients, while one-third of patients present neurological impairment [2, 5, 7]. In a Swiss study, in 12 out of 37 patients with spinal cord injury, the level of the neurological damage and that of the vertebral fracture differed by two segments: the authors assume that the particular injury mechanism responsible for these injuries, involving mainly axial forces compressing or stretching multiple segments at once, explains this difference to the non-paraglider paraplegic patients [2]. There is a typical peak at the thoracolumbar junction, with L1 as the most affected vertebra (30–35 %), as compared to the fracture distribution in general trauma where another similar peak at the lower cervical spine and a third smaller peak at the mid-thoracic spine are described [2, 5, 8].
In paragliding incidents, injuries to the cervical spine (6–8 %) and head (5–16 %) are relatively rare, but the total frequency of spinal and pelvic injuries is far higher as compared to general and sports trauma and highlights the danger of the massive impact forces at deceleration [2–5, 9]. The spinopelvic junction has been identified as being at special risk in paragliding incidents: in a retrospective series, 8 of 144 severely injured paragliders sustained a spinopelvic dissociation, an injury also known as a “suicidal jumper’s fracture” [5] (Fig. 18.5). Compared to the normal trauma population, the injured paraglider has a 19-fold increased risk of sustaining such an otherwise rare fracture. One possible explanation may be the additional horizontal force vectors that occur during the paraglider’s landing, as the inertia of the axial and horizontal moved mass of the torso forces the lumbar spine into lordosis, resulting in flexion-type jumper’s fractures [5, 10].
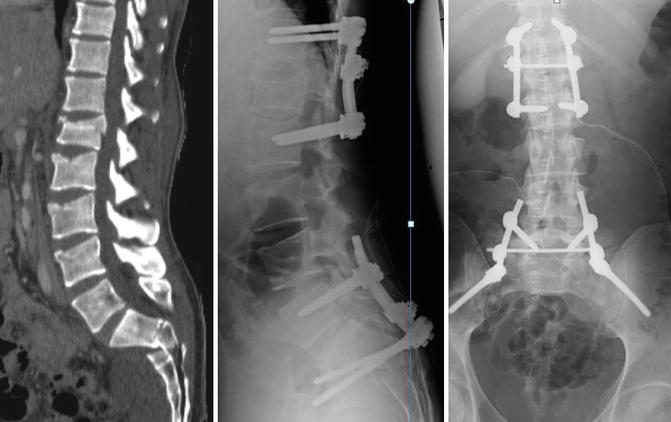
Fig. 18.5
Typical fracture pattern of a 30-year-old paraglider with lumbar compression-type fractures, superior burst-split fracture of L1, flexion type 2 spinopelvic dissociation with impaired S2 and S3 root function
Non-skeletal injuries are less frequent: severe thoracic, visceral, and vascular trauma are reported, often concomitant to injuries of the spine [9, 11]. Three cases of traumatic rupture of the descending aorta, associated with multiple injuries following a paragliding blunt trauma, have been attributed to the chest being crushed and the sudden brusque deceleration [12]. Cases of myocardial contusion, hematothorax, pneumothorax, and gut and urinary bladder rupture, as well as liver contusion with bleeding, have also been reported [13].
18.3.1 Medical Considerations with Regard to the Dynamic of Injuries
One-third of the incidents occur during the launch phase. Launching with a paraglider requires a fast run downhill from a slope until the sail inflates and provides sufficient lift. Most of the injuries during takeoff involve the ankle, as a consequence of a fall while the pilot is running on the ground. Launch injuries are usually minor. However, major spinal injuries can occur if the pilot overestimates the lifting airstream and sits back too early, landing on his buttocks [3].
Although in-flight incidents as a consequence of a sail collapse or turbulence are rare (16 %), crashes from a great height can lead to multiple injuries involving fractures of the talus, pelvis, and spine [3]. In these cases, plain radiographs or computed tomography (CT), particularly of the lower spine and pelvis, is essential in order to exclude fractures. Neurological observation is necessary in the short term. In the case of such incidents, ultrasound imaging should also be performed to exclude closed abdominal injuries [3].
The most dangerous phase of the paragliding flight is landing [1, 3, 14, 15]. During landing, the legs can bend and absorb part of the impact. Injuries of various degrees may happen as a consequence of poor technique, such as landing with the legs straight. Large axial compression forces act on the spine and lower limbs at the time of contact with the ground, which predisposes the paraglider to compression fractures of the spine and calcaneus [4]. Uncontrolled landings can occur if the descent is too rapid, due to misjudgment or turbulence: since these may result in high-energy trauma, major injuries should be excluded in all of these cases. In victims of severe paragliding incidents, contrast-enhanced CT should be included in the routine emergency radiologic evaluation, in order to exclude severe injuries, including traumatic aortic rupture [12].
18.3.2 Treatment and Outcome of Paragliding Acute Traumatic Injuries
Initial treatment should strictly follow the ATLS guidelines; the relatively frequent and possibly life-threatening pelvic fractures and deceleration injuries to abdominal organs and vessels need to be ruled out. The same applies to thoracic trauma cases, which are seen in over 20 % of all cases [2, 4, 5, 9]. Careful assessment and documentation of neurological status is mandatory. Selective bladder or bowel dysfunction may be present in spinopelvic dissociation. Spinal fractures are seen mostly at the thoracolumbar junction, but multiple spinal fractures are also common (17–26 %) and need to be considered in the examination, as well as non-spinal fractures that concomitantly occur in more than half of the patients with severe spinal trauma [2, 5]. Most of these fractures are unstable and require surgical treatment. Indications and technical preferences vary greatly among regions [4, 5].
Over 60 % of injured paragliders are admitted to a hospital. Length of hospital stay varies from 22 to 26 days on average, and the duration of disablement ranges from 80 to 98 days on average. About 43–70 % of patients resumed paragliding [7, 9].
Even patients with severe neurological impairment from spinal cord injury showed a high potential for neurological recovery. In particular, patients with a bony occlusion of the spinal canal of less than 70 % improved substantially, with 13 out of 14 patients ambulatory after the rehabilitation phase of 3–4 months on average (compared to 13 of 19 patients with occlusion >70 %). As expected, patients with type A (vertebral body compression) lesions, according to Magerl et al. [16], recovered better than those with type C fractures (anterior and posterior element injury with rotation) [2]. Nearly all patients with spinopelvic dissociations will present neurological impairment with the nerve roots below the level L5 being incompletely affected: incomplete recovery and persisting bladder and bowel dysfunction are expected [5].
18.3.3 Crashed Pilot Rescue
Especially in remote areas difficult to access with ground vehicles, evacuation of crashed paragliding pilots is very often possible by helicopter only [9]. The use of a helicopter may be also justified by the need for immediate medical support. When approaching a victim of a paragliding incident near a slope crowded with paragliders, the risk of collision of the helicopter with other gliders may be high. Landing the helicopter at the incident site is often impracticable due to the tight spaces, and rescue operations are sometimes possible only by means of a cable winch or a long rope fixed to the helicopter [17]. Since the downwash of the rotor blades could blow the paraglider upward, resulting in a secondary lethal crash if the stranded athlete is still attached to his wing, a direct approach of a helicopter is advisable only if the pilot has secured the scene by detaching and folding his wing.
When a direct approach is appropriate, a long-line rescue with extension of the rope up to 200 m may reduce the risk of downwash, even if this maneuver remains extremely risky for the rescue team. Unfortunately, rescue situations such as these are unusual: generally the rescue team is lowered to the ground as close as possible to the incident scene and walks or climbs to reach the stranded pilot.
There are cases of crashed pilots stranded on the cables of a cable car [9], and specific evacuation techniques are required in these situations. The emergency physician should perform a careful examination of the pilot, despite the challenging environmental conditions. Knowledge of the injury pattern typically sustained by crashed paraglider pilots is a valuable aid when formulating the primary diagnosis, important when deciding the most appropriate care facility for the victim, based on the specific injuries sustained [9]. It is vital to stabilize the patient before starting transportation: this should include securing the airways, immobilizing the spine, stabilizing fractures with the aid of a vacuum mattress, and beginning infusion and analgesics [9].
18.4 Musculoskeletal Injuries Due to Specific Patterns of Movements
Musculoskeletal, ligament, and tendon injuries related to functional overload and to the specific patterns of movements required in paragliding are rarely reported, probably because more attention has been paid to injuries resulting from high-energy trauma injuries up to now; however they are probably underestimated. Shoulder dislocation, for example, is a common paragliding injury and may be a consequence of the particular movement required when pulling up the sail [18]. Schulze Bertelsbeck et al. [19] also reported the case of a pilot who sustained a bilateral partial rupture of the rectus femoris muscle during a paragliding landing maneuver. Rupture of the rectus femoris muscle is a rather uncommon condition: the rectus femoris is the only biarticular muscle in the quadriceps, making it prone to muscle strain injuries when undergoing eccentric contractions [20–23]. During a paragliding landing, the pilot absorbs energy through his legs [3], and the quadriceps exerts an eccentric contraction to counteract the impact: accordingly, the rectus may be subject to strains and ruptures during landings with a paraglider. Effective strategies to prevent such injuries, therefore, may include an appropriate flight technique (including a proper reduction of the speed during the approach phase), together with a workout focused on the specific types of efforts required.
18.5 Environmental Illnesses
Various non-traumatic, yet potentially life-threatening conditions are reported in literature: they are characteristic of this extreme sport and are associated with exposure to environmental agents. Although the data in question consists of isolated reports, it takes on greater importance in the absence of systematic sets of data. Physicians should be aware of the potential for these health problems and take them into consideration, both when formulating the primary diagnosis, which often needs to be done rapidly, and when considering suitable strategies for the prevention of these conditions.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


