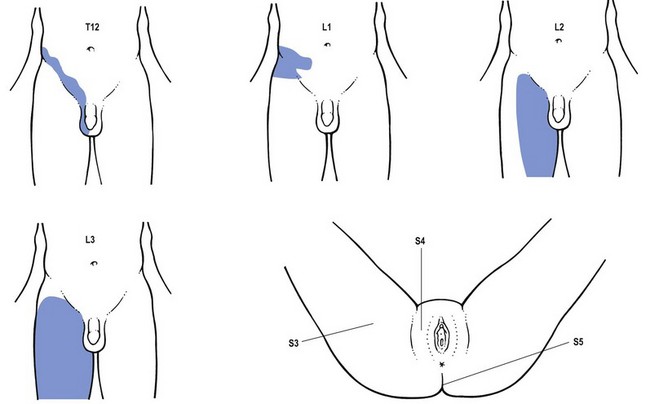
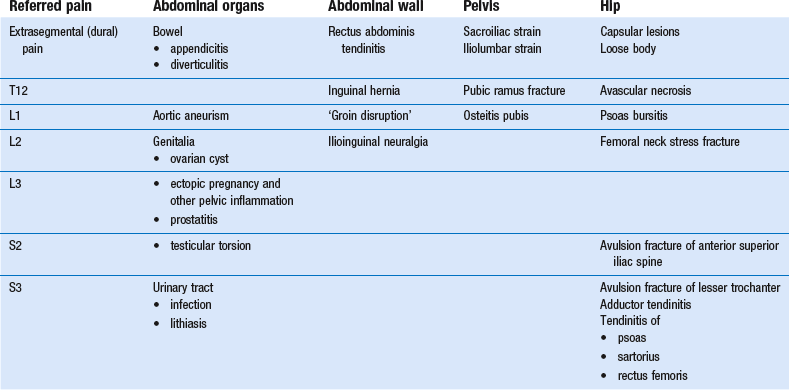
Groin injuries tax the diagnostic and therapeutic abilities of the clinician.1,2 Although they are considered to be common and the most frequent overuse syndromes in some athletic activities such as soccer,3 they are difficult to manage correctly. The clinician confronted with the prospect of evaluating a patient who complains of groin pain should first of all ask the patient to point to the pain and also establish whether it is localized or diffuse. The groin area is not only the crossing site of trunk and lower extremity muscles but is also a region of considerable dermatomical overlap which includes T11, T12, L1, L2, L3 and S4 (Fig. 1). Pain in the groin can also be of extrasegmental origin. Once the localization and any radiation of the pain have been clarified, the examiner continues with the routine history which relates to problems in the back, sacroiliac region and the hip (see Ch. 36, 45, 61). Finally questions related to possible intra-abdominal disorders may be indicated. For example: The causes that can result in groin pain are numerous and are summarized in Table 1. Differential diagnosis is not difficult if the guidelines and principles for a good functional examination of the lumbar spine and hip are followed. However, occasionally the results may be confusing. This is usually caused by the fact that resisted movements in and around the groin not only stress the activated contractile structures, but often also induce transmitted stress on inert structures (bones, ligaments). For example, resisted ad- and abduction movements of the hip may indirectly put stress on the sacroiliac or iliolumbar ligaments or on the pubic symphysis. Examination reveals an antalgic gait. There is usually a discrepancy between the obvious gait and the rather subtle signs on clinical examination: a full range of motion with pain produced at the extremes of hip rotation and on axial compression.4,5 Early radiographs may be negative and absence of a fracture line does not rule out a stress fracture. A bone scan should be positive 2–8 days after symptoms appear. Further imaging studies such as computed tomography (CT) or magnetic resonance imaging (MRI) should be undertaken early if clinical suspicion warrants it.6 Treatment is based on the type of fracture. If the bone scan is positive but there is no visible fracture on plain film, initial treatment will consist of modified bed rest. This leads on to non-weight bearing with crutches and then pain-free weight bearing.3 If there is visible fracture on the plain film, open reduction and internal fixation is the treatment of choice because of the high risk of displacement. An already displaced fracture is considered an orthopaedic emergency and requires open reduction and internal fixation. Recent arthroscopic studies suggest that most internal derangement in the hip may be the result of impingement of acetabular labral tears.7 The history is that of internal derangement: a feeling of giving way or a sharp ‘twinge’ in the groin that radiates into the anterior thigh, especially with a rotation of the hip while rising from a seated position. On examination, a non-capsular pattern of limitation is found, with limitation of lateral rotation (see p. 642). Some authors report successful diagnosis of impingement lesions with the so-called Thomas test.3 This involves flexion and external rotation of the hip and then allowing the extremity to abduct. The hip is then moved into extension, internal rotation and adduction. A positive test result is indicated by a palpable or audible click and the production of typical pain. Arthrography, MRI and arthroscopy can be used to confirm the diagnosis. Treatment consists of manipulation (p. 642), although arthroscopic or open operative excision may be necessary in recalcitrant cases.
Groin pain

Introduction
History
Interpretation
Femoral neck stress fracture
Acetabular labral tears
pain