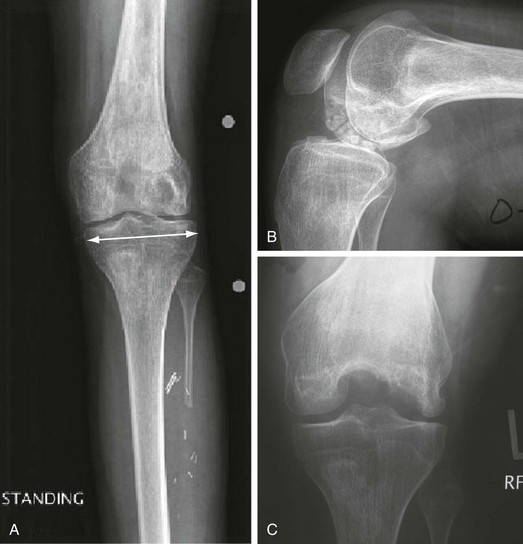
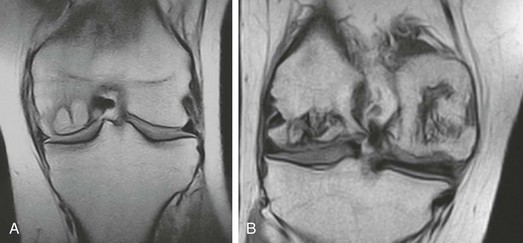
Chapter 66 • Range of motion: may be decreased secondary to pain, muscle spasm, or subchondral collapse • Swelling, effusion; may or may not be present • Weight-bearing anteroposterior (AP) radiograph of knee in full extension with a radiopaque magnification marker (Fig. 66-1A) • Non–weight-bearing 90-degree-flexion lateral view of knee (Fig. 66-1B) • Notch (Fig. 66-1C) or Rosenberg view of knee • Magnetic resonance imaging (MRI) can help to confirm the diagnosis and the extent of lesion(s) (Fig. 66-2). • Technetium-99m bone scanning is generally unreliable but may assist in diagnosis when radiographs are negative. Bipolar uptake is more indicative of osteoarthritis, except in the late stages of ON. Conversely, simultaneous atraumatic ON of the ipsilateral tibial plateau and femoral condyle is certainly possible during any stage and usually causes more intense uptake than osteoarthritis. The Aglietti classification for spontaneous ON of the knee (modified Koshino) and the Mont and Hungerford classification for secondary ON of the knee (modified Ficat and Arlet) are described in Boxes 66-1 and 66-2. Nonoperative Treatment (Only in Low-Grade, Low-Symptom, Precollapse Lesions) • Nonsteroidal antiinflammatory drugs (NSAIDs), if tolerated • Pharmacologic treatment based on underlying disease process • Activity modifications and protective weight bearing • Closed-chain quadriceps exercises
Osteonecrosis of the Knee
Preoperative Considerations
Physical Examination
Imaging
Other Modalities
Staging
Treatment
Related posts:
 Open Repair of Posterior Shoulder Instability
Open Repair of Posterior Shoulder Instability
 Autologous Chondrocyte Implantation in the Knee
Autologous Chondrocyte Implantation in the Knee
 Allografts for Anterior Cruciate Ligament Reconstruction
Allografts for Anterior Cruciate Ligament Reconstruction
 All-Inside Anterior Cruciate Ligament GraftLink Technique: Second-Generation, No-Incision Anterior Cruciate Ligament Reconstruction
All-Inside Anterior Cruciate Ligament GraftLink Technique: Second-Generation, No-Incision Anterior Cruciate Ligament Reconstruction
 Hamstring Tendon Autograft for Anterior Cruciate Ligament Reconstruction
Hamstring Tendon Autograft for Anterior Cruciate Ligament Reconstruction
 Arthroscopic Meniscus Repair: All-Inside Technique
Arthroscopic Meniscus Repair: All-Inside Technique
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Osteonecrosis of the Knee