CHAPTER 9 Osteocapsular Arthroplasty of the Elbow
Arthroscopic osteocapsular arthroplasty is a procedure involving three-dimensional reshaping of the bones (i.e., removal of osteophytes), removal of any loose bodies, and capsulectomy to restore motion and function and to eliminate pain.1
Arthroscopic release is effective for soft tissue contractures of the elbow.2–5 When arthritic changes are present, bone work is also necessary.1,6–12
ANATOMY
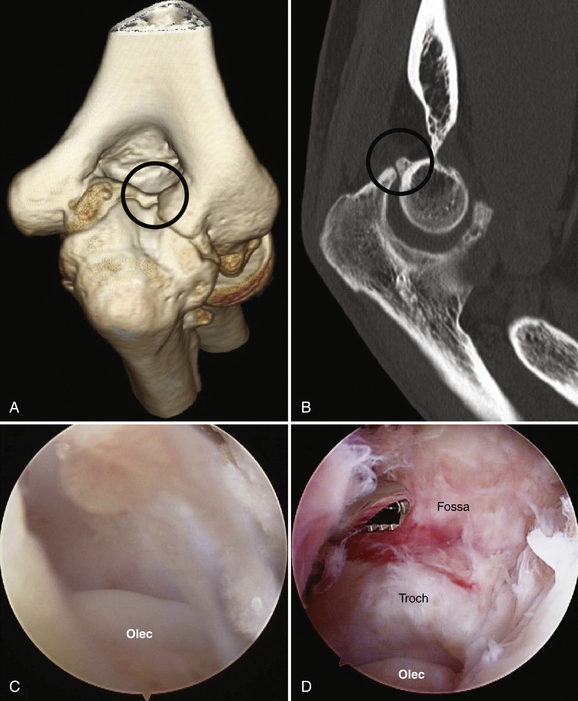
Osteophytes build up in typical locations along the margins of the joint and in the fossae. Although the patient may have osteophytes on the posteromedial olecranon, osteophytes alone do not always cause impingement pain. The relationship between bony osteophytes and impingement pain poses an apparent dilemma. It is not unusual to see osteophytes that impinge at the limit of motion in patients who have no pain. The question is why some osteophytes are painful and others are not. Based on experience and unpublished research in progress, I think the usual cause for impingement pain in such circumstances is a fractured olecranon osteophyte that has typically progressed to nonunion by the time of referral to the orthopedic surgeon.13 Nonunion fractures are best visualized (Fig. 9-1) on sagittal and coronal computed tomography (CT) reconstructions. The loose fragment is easily missed during arthroscopy because it is very small or covered with cartilage and not obviously loose. In some patients, the loose fragment is removed during osteophyte excision without ever being recognized. Other causes for the pain include loose bodies or buildup of inflamed soft tissue posteriorly.

PATIENT EVALUATION
History and Physical Examination
I have found that the diagnosis of posterior impingement due to fractured nonunited osteophytes can be confirmed with confidence on physical examination using the extension impingement test and the arm bar test.13 The extension impingement test is performed by starting with elbow near full extension and then quickly (but gently to prevent injury) snapping it into terminal extension. This maneuver reproduces the posterior or posteromedial pain experienced during provocative activities such as throwing. A simultaneous valgus load normally enhances the pain if the pathology is primarily posteromedial.
A similar test is the arm bar test, which is a variation of a martial arts maneuver. With the patient’s shoulder in full internal rotation, the examiner extends the elbow to its full limit and then (gently at first) hyperextends it. This is reproducibly performed with the patient’s shoulder in full internal rotation and 90 degrees of forward elevation. The patient’s hand is placed on the shoulder of the examiner, and the examiner pulls down on the olecranon, leveraging the elbow into extension. Reproduction of the patient’s pain is expected if impingement is present. I have found this test to be more sensitive than the extension impingement test if the patient’s symptoms are relatively minor or have diminished just before consultation.
Diagnostic Imaging
CT with three-dimensional surface rendering provides excellent imaging of the bony pathology (Fig. 9-2A). The individual bones can be isolated from each other and spun around in three dimensions, demonstrating the location and structure of each osteophyte and loose body. Two-dimensional sagittal and coronal reconstructions are also necessary, because they reveal the fine details not available in the three-dimensional images (see Fig. 9-2B), including nonunited fractures, the original floors of the fossae, and small loose bodies embedded in the cartilage surfaces. Axial two-dimensional reconstructions complete the imaging protocol.
TREATMENT
Alternative Surgical Treatments
Alternatives to arthroscopic osteocapsular arthroplasty include arthroscopic or open Outerbridge-Kashiwagi, open column, and open Tsuge procedures.6,8–12 In my experience, drilling a hole through the olecranon fossa does not adequately decompresses the coronoid fossa or the olecranon fossa, and it fails to address osteophytes in the radial fossa. It also eliminates the bony landmarks used to determine just how much bone should be removed from the fossa. The open column procedure does not permit as accurate and complete removal of osteophytes or contracted capsule (e.g., medial gutter) as the arthroscopic procedure. The Tsuge procedure has a high morbidity rate with no apparent advantages over arthroscopic osteocapsular arthroplasty.
Arthroscopic Technique
Arthroscopic osteocapsular arthroplasty is a complex procedure requiring a high level of experience in elbow arthroscopy for its safe and effective performance. I have learned by experience that it is best performed in a stepwise sequence, starting posteriorly and completing the work in the gutters before going anteriorly (Box 9-1).
Posterior Joint Compartment
Step 1: Get In and Establish a View.
The first step is to get in and establish a view. Place the scope in the posterolateral portal and the shaver in the posterior portal. Confirm by visualizing identifiable articular structures that you are inside the joint and that you have the correct anatomic orientation (see Fig. 9-2C). Touch the tips of the shaver and scope together by triangulation, and visualize the shaver blade. By using surface anatomic landmarks, it should be possible to verify the shaver is within the olecranon fossa. This can be confirmed by tactile feedback as the shaver is moved up and down the sides of the fossa and around its rim.




