CHAPTER 35 Wrist Arthroscopy: The Future
Wrist arthroscopy, first described by Chen in 1979,1 was popularized by Roth and colleagues in an instructional course lecture of the American Academy of Orthopaedic Surgeons almost a decade later.2 Since then, it has undergone substantial developments and has become an essential diagnostic and therapeutic tool for surgeons addressing a multitude of conditions affecting the wrist.
With improved techniques and equipment, procedures that were once performed as open surgery can be undertaken arthroscopically. Although initial therapeutic wrist arthroscopy focused on basic reparative procedures, some of the more complex reconstructive and salvage procedures are being performed with this procedure (Table 35-1), and the indications for wrist arthroscopy continue to expand. This chapter reviews some of the latest advances and discusses future directions for wrist arthroscopy.
TABLE 35-1 Expanding Indications for Wrist Arthroscopy
| Procedures | Soft Tissue | Bone |
|---|---|---|
| Diagnostic | ||
| Removal (“ectomy”) | ||
| Stabilization | ||
| Reconstructive | ||
| Salvage |
DRUJ, distal radioulnar joint; STT, scaphotrapeziotrapezoid; TFCC, triangular fibrocartilage complex.
ASSESSMENT
Arthroscopic examination of the wrist should include the radiocarpal and midcarpal joints and, if indicated, the distal radioulnar joint (DRUJ). Visualization of the pisotriquetral joint can be achieved through a fenestration communicating with the radiocarpal joint (which is present in approximately 50% of the population).3 Traditionally, dorsal 3-4, 4-5, 6-R, and midcarpal portals have been used as diagnostic and working portals (Table 35-2). These portals limit access to the dorsal wrist capsule and impose restrictions on the surgeon’s ability to treat dorsal pathology. The development of volar portals4–6 has provided freedom to explore newer arthroscopic techniques to address certain pathologic conditions such as dorsal wrist ganglion7 or capsular restriction.8
TABLE 35-2 Arthroscopic Wrist Portals: Technique and Comment
| Portals | Technique | Comment |
|---|---|---|
| Dorsal Portals | ||
| 1-2 | Inserted in the extreme dorsum of the snuffbox just radial to the EPL tendon to avoid the radial artery48,49 | Gives access to the radial styloid, scaphoid, lunate, and articular surface of the distal radius |
| 3-4 | Portal is 1 cm distal to Lister’s tubercle between the tendons of the third and fourth compartment | Main working portal; gives a wide range of movement and view |
| 4-5 | Between the common extensor fourth compartment and the EI in the fifth compartment | Usually, the 6-R portal is preferred |
| 6-R | Located distal to the ulnar head and radial to the ECU tendon; portal is established under direct vision through the arthroscope with a needle and avoids damage to the TFCC | Main working portal |
| 6-U | Established under direct vision, similar to the 6-R portal; always use blunt dissection to avoid the dorsal branches of the ulnar nerve | 6-U and 6-R portals allow visualization back toward the radial side and access to the ulna-sided structures |
| DRUJ | Forearm supinated to relax the dorsal capsule; arthroscope is introduced into the axilla between radius and ulna underneath the TFCC | Gives a view of the DRUJ articulation |
| Midcarpal Portals | ||
| MCR | Soft depression palpated between proximal and distal carpal rows, 1 cm distal to the 3-4 portal along a line bordering the radial edge of the third metacarpal | Can be used to get across to the STT joint, scapholunate articulation, and distal pole of scaphoid |
| MCU | Soft depression palpated between proximal and distal carpal rows 1 cm distal to 4-5 portal and in line with the fourth metacarpal | Allows visualization of the distal lunate, lunotriquetral, and triquetral hamate articulation |
| STT | Between EPL and ECRB in the midcarpal row; on the ulnar margin of the EPL tendon; terminal branches of the radial sensory nerve are at risk | Used with the MCR portal for STT débridement |
| Volar Portals | ||
| VR | A 2-cm longitudinal incision is made over the FCR on radial side of volar proximal wrist crease, and the FCR is retracted ulnarly. Radiocarpal joint is identified with a needle, and the port is expanded with artery forceps.3 An inside-out technique also can be used. Work between the RSC and LR ligaments, staying to the radial side of the FCR tendon to avoid the median nerve.2 | Safe zone of 3 mm in all directions with respect to the palmar cutaneous branch of the median nerve (ulnarly) and radial artery (radially)2,3 |
| VU | A 2-cm longitudinal incision is made; the FCU is identified and retracted ulnarly with the ulnar nerve. Working in the interval between the FCU and common flexor tendons, inserting needle into the joint and then expanding the area with an artery forceps4 | Both volar portals are used to assist in reduction of distal radius fracture and to view the dorsal articular surface and dorsal ligaments |
| DRUJ | Use the same mini-open approach as for a VU portal; take care to stay below the TFCC | Gives a view of the DRUJ and deep-sided TFCC tears |
DRUJ, distal radioulnar joint; ECRB, extensor carpi radialis brevis; ECRL, extensor carpi radialis longus; ECU, extensor carpi ulnaris; EDC, extensor digitorum communis; EI, extensor indicis; EPB, extensor pollicis brevis; EPL, extensor pollicis longus; FCR, flexor carpi radialis; FCU, flexor carpi ulnaris; LR, long radiolunate; MCR, midcarpal radial; MCU, midcarpal ulnar; RSC, radioscaphocapitate ligament; STT, scaphotrapeziotrapezoid; TFCC, triangular fibrocartilage complex; VR, volar radial; VU, volar ulnar.
From Bain GI, Munt J, Turner PC. New advances in wrist arthroscopy. Arthroscopy. 2008;24:355-367.
The wrist can be visualized as a box with access through four sides (Fig. 35-1). The arthroscope can be introduced to provide the optimal view of pathology, and any number of portals can be used for instrumentation. The use of multiple portals does not increase the surgical insult significantly as long as standard precautions are taken to protect soft tissue structures, but it can ensure that the surgeon has optimal placement of instruments and the arthroscope.
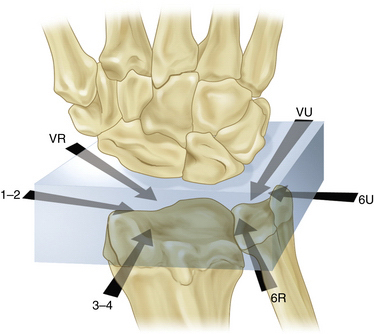
FIGURE 35-1 The box concept of wrist arthroscopy.
(Modified from Bain GI, Munt J, Turner PC. New advances in wrist arthroscopy. Arthroscopy. 2008; 24:355-367.)
Most investigators describe arthroscopy of the wrist in a manner similar to large joint arthroscopy, with infiltration of the joint with fluid (i.e., lactated Ringer’s solution). Dry arthroscopy of the wrist has not been associated with undue procedural difficulty.9 It provides a different perspective of tissue and chondral surfaces. Other benefits of the dry technique include a decreased risk of compartment syndrome and the availability of dry tissue planes in the event of conversion to open surgery. The main role of dry wrist arthroscopy is in the management of intra-articular distal radial fractures,10 but indications may broaden to include carpal fracture management and other reconstructive procedures.
The value of arthroscopy can be augmented by the use of fluoroscopy, which enables accurate intraosseous placement of drills and implants. It also can be used to confirm reduction of fractures or joint diastasis.11
SPECIFIC AREAS OF ADVANCEMENT
Carpal Instability
Assessment of Instability
Numerous radiologic investigations are used to assess carpal instability, including plain radiographs, fluoroscopy, arthrography, computed tomography (CT), and magnetic resonance imaging (MRI). Although three-compartment arthrography can identify intercarpal ligament perforations, it is inadequate for localizing these lesions.12 CT is less sensitive than MRI for detecting intercarpal ligament tears and triangular fibrocartilage complex (TFCC) injuries.13
Arthroscopy is the gold standard for the diagnosis of carpal instability. It has the benefit of giving surgeons direct visualization of the scapholunate and lunotriquetral ligaments and allows them to assess the state of the ligament, the extent of the ligament injury, and whether it is reparable. Associated problems such as hemorrhage, synovitis, chondral damage, and degenerative changes can be assessed at the time of arthroscopy.
Repair Procedures
Arthroscopic débridement alone has been used in the management of scapholunate interosseous ligament (SLIL) and lunotriquetral interosseous ligament (LTIL) injuries. Good results have been achieved from arthroscopic débridement of partial tears of the SLIL and LTIL.14,15 Weiss and colleagues described arthroscopic débridement as sole treatment for complete tears of the SLIL and LTIL.15
There has been interest in the use of ligament and capsular thermal shrinkage in the treatment of interosseous ligament injuries, and early results are promising. Good results have been achieved with arthroscopic débridement and thermal shrinkage of Geissler grade I or II injuries (Table 35-3).16–18 Battistella and coworkers compared outcomes of débridement alone and thermal shrinkage as a sole treatment of Geissler I SLIL injuries.19 They also compared the results of débridement and pinning with those of thermal shrinkage and pinning for Geissler II and III injuries. In both comparisons, superior outcomes were achieved with thermal shrinkage.19 However, the use of thermal shrinkage techniques remains controversial, and no long-term studies have been published to confirm its safety and efficacy.
TABLE 35-3 Geissler Arthroscopic Classification of Carpal Instability
| Grade | Description |
|---|---|
| I | Attenuation or hemorrhage of interosseous ligament as seen from the radiocarpal joint. No incongruence of carpal alignment in the midcarpal space. |
| II | Attenuation or hemorrhage of interosseous ligament as seen from the radiocarpal joint. Incongruence or step-off as seen from midcarpal space. A slight gap (less than width of a probe) between the carpal bones may be present. |
| III | Incongruence or step-off of carpal alignment is seen in the radiocarpal and midcarpal space. The probe may be passed through the gap between the carpal bones. |
| IV | Incongruence or step-off of carpal alignment is seen in the radiocarpal and midcarpal space. There is gross instability with manipulation. A 2.7-mm arthroscope may be passed through the gap between the carpal bones. |
From Geissler WB. Intra-articular distal radius fractures: The role of arthroscopy. Hand Clin. 2005;21:407-416.
In patients with significant instability (Geissler grades II through IV), arthroscopic débridement and percutaneous pinning have produced mixed results.20–22 Whipple’s series supported the concept that the chronicity of the lesion and the degree of instability affect the eventual outcomes.20 In that study, SLIL tears were treated with arthroscopically assisted reduction and percutaneous pinning, and outcomes were compared for patients with less than 3 months’ history and less than 3 mm of scapholunate displacement and for those with symptoms of more than 3 months’ duration and more than 3 mm of displacement. Eighty-five percent of patients in the first group maintained comfort and stability at 2 to 7 years, and 53% of patients in the second group remained symptom free at 1 to 3 years.
The reduction-association scapholunate (RASL) procedure is often performed as an open procedure for chronic scapholunate instability. An arthroscopically assisted method of RASL has been described, with arthroscopy facilitating anatomic reduction and precise placement of the cannulated screw, with the advantage of a three-portal rather than a two-incision approach.23
The future role of arthroscopy in treating carpal instability is likely to include arthroscopically assisted tendon graft reconstruction procedures, such as the modified Brunelli procedure.24




