CHAPTER 19 Wrist Arthroscopy: Setup, Anatomy, and Portals
Wrist arthroscopy has been used since it was first described by Chen in 1979.1 In the early stages of development, it provided only partial evaluation of the articular surfaces, and it was not used therapeutically. Few investigators routinely used arthroscopic techniques.2 It was not until 1986, when Whipple advocated distraction techniques and precise portal placement, that the exposure necessary to perform an extensive evaluation of the wrist joint became an option.3 Even then, diagnosis was the primary function, and therapeutic indications were minimal. Since that time, innovations in wrist arthroscopy have expanded treatment indications and promoted widespread acceptance.
Diagnostic and operative forms of arthroscopy have advanced our understanding of wrist anatomy and function, and arthroscopic techniques have facilitated the repair of previously unrecognized pathology. Continued advances in instrumentation and technology will improve the ability to perform challenging and innovative procedures as the principles of open surgical procedures become adapted to arthroscopy.4
Wrist arthroscopy allows close visual examination of the carpal articular surfaces and wrist ligaments, which is often inadequate with open procedures and which can be performed in a less invasive manner than traditional arthrotomy.5 The extremely close evaluation of details provides many benefits and increases appreciation of the subtle differences between normal and pathologic anatomy.6 This fact alone underscores the importance of a thorough understanding of arthroscopic anatomy.
ANATOMY
The wrist is made up of the eight carpal bones, each with multiple articular surfaces and the intrinsic and extrinsic ligaments, and a triangular fibrocartilage complex (TFCC) that is surrounded by tendons and neurovascular structures (Fig. 19-1).7,8 A thorough understanding of the relationship between the surface anatomy of the wrist and these underlying structures is essential to perform accurate arthroscopic portal placement and adequate arthroscopy. Understanding these relationships helps to prevent injury to the cutaneous nerves, tendons, and vascular structures and can minimize the risk to the articular surfaces in the wrist. It also facilitates the use of instruments during procedures, enabling the completion of increasingly complicated arthroscopic wrist procedures.
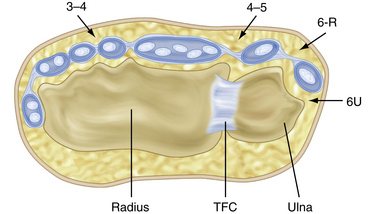
FIGURE 19-1 Cross-sectional anatomy of the dorsal compartments.
(Modified from Geissler WB, Freeland AE, Weiss AP, Chow JC. Techniques of wrist arthroscopy. Instr Course Lect. 2000:49:225-237.)
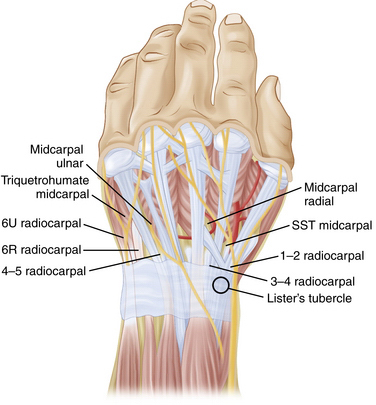
The extensor retinaculum is an obliquely oriented structure that spans the dorsal distal radius and ulna. It overlies the 12 extensor tendons, which are partitioned into six compartments to prevent bowstringing of the extensor tendons.4 The extensor pollicis longus (EPL) is the only tendon in the third compartment, and it is easily palpated, especially after application of traction. This structure passes just ulnar to Lister’s tubercle and should be appropriately marked. The area bordered by the EPL and extensor pollicis brevis together and the extensor carpi radialis longus (ECRL) define the margins of the anatomic snuffbox. The extensor digitorum communis (EDC) is just ulnar to the EPL. The extensor carpi ulnaris (ECU) and the ECRL and ECRB tendons are easily palpated and should be marked. The intersection of these tendons and the bony structures allows accurate identification and precise placement arthroscopy portals (Fig. 19-2).
PATIENT EVALUATION
History and Physical Examination
A thorough history and physical examination are essential before proceeding with arthroscopic evaluation of the wrist. It has been said that if no diagnosis can be made after a thorough clinical assessment, little additional information can be obtained from arthoscopy.9 A meticulous history helps focus the examiner on the cause and directs the physical examination to the suspected pathology. The examiner must determine the activities that exacerbate or lessen the problem, the functional loss, and the ability of the patient to perform daily activities, including work and leisure activities. The mechanism of injury should be ascertained.
Physical examination is the most accurate method for diagnosing pathology.2 A systematic approach to the wrist examination is essential. All joints must be carefully inspected, palpated, and appropriately stressed with the use of provocative tests. Areas of swelling, tenderness, or pain can focus attention on the specific pathology. Examination includes palpation of the tendons and evaluation of the patient’s neurologic and vascular status.
Diagnostic Imaging
Occasionally, the diagnosis remains unclear after an adequate history, physical examination, and routine radiographic studies have been completed. Further diagnostic studies may be indicated. Computed tomography (CT) is useful for evaluating osseous and articular morphology. Magnetic resonance imaging (MRI) provides important information about the soft tissues of the wrist and the vascularity of bones. The most definitive study is magnetic resonance arthrography, which begins with a radiocarpal injection followed by a distal radioulnar joint injection.10
TREATMENT
Indications and Contraindications
Wrist arthroscopy provides an accurate complement to the probable diagnosis obtained from the physical examination. Arthroscopy is useful for evaluation of patients with wrist pain and motion loss when noninvasive studies have failed to provide a diagnosis, and it is more sensitive than arthrography for evaluating pathology.8 Diagnosis of interosseous ligaments tears and the degree of carpal instability can be accurately determined using arthroscopy. It is also useful in patients with well-defined pathology, such as nonunions, Kienbock’s disease, and scapholunate or lunotriquetral dissociations, for which evaluation of the articular surfaces is of prognostic and therapeutic importance.
Although once used almost exclusively for diagnostic purposes, the therapeutic indications for wrist arthroscopy continue to expand. Arthroscopic treatment is indicated for loose body removal, synovectomy, intra-articular adhesion release, lavage of a septic wrist, débridement of chondral lesions, hypertrophic or torn ligaments, and tears of the TFCC. It has also been used for dorsal ganglion excision and provides a useful adjunct in the reduction of distal radius and scaphoid fractures. Bone excision procedures, such as radial styloidectomy and partial resection of the distal ulna (i.e., wafer procedures), have been performed arthroscopically. Arthroscopy has been described for advanced procedures, such as proximal row carpectomy, excision of the proximal pole of the scaphoid, lunate excision in Kienbock’s disease, and capitolunate arthrodesis.7,8
Conservative Management
Before arthroscopy, nonoperative measures should usually be exhausted. Temporary immobilization and anti-inflammatory medication may be helpful. Diagnostic and therapeutic injections frequently provide some benefit. A physical therapy regimen for wrist range of motion and strengthening may prove definitive for some wrist pathology.
Arthroscopic Technique
Setup
A significant improvement in wrist arthroscopy came with the innovation of wrist distraction. This key element enhanced the surgeon’s ability to perform arthroscopic procedures in the confined wrist joint. Distraction is essential to improve visualization and provide adequate space for maneuverability during wrist arthroscopy, because distention of the joint alone does not provide adequate room for instrumentation.2 Several options exist to provide the necessary distraction. A dedicated sterile or nonsterile traction tower is a popular choice. Alternatives include the use of horizontal traction with a pulley and weight system and a nonsterile traction boom device (Figs. 19-3 to 19-5).



We prefer a sterile traction tower with nylon finger traps. It provides convenient application of wrist distraction in flexion, extension, and radial and ulnar deviation. This system allows adjustability to the distraction force and the position of the wrist, and it permits easy conversion to open procedures if necessary. The traction tower system maintains the wrist in a stable position for portal preservation during the exchange of instruments.2
The arm is placed in an abducted position, and the upper arm is secured to the traction tower. A nonsterile tourniquet is applied, and the arm and hand are prepared and draped with the forearm in a vertical position (Fig. 19-6). We use sterile soft nylon finger traps to secure the index and long finger to the tower for most procedures. Soft traps increase the surface area and distribute the force better than wire devices. For patients with poor or fragile skin, additional fingers in the traps can decrease the force to the skin.2 To improve visualization for ulnar-sided pathology, we frequently use the index and ring fingers (Fig. 19-7). Most procedures require 5 to 10 pounds of traction.


Equipment
Other small joint arthroscopy equipment is available and necessary for mastery of wrist arthroscopy. Equipment includes a small joint shaver (2.7 or 2.9 mm) with multiple tips, a wrist probe (1.7 or 2.0 mm), and many of the smaller versions of large joint arthroscopic instruments.5,7 As arthroscopy has advanced, more specialized equipment has become available, including TFCC repair kits, retrograde retrievers, ablation shrinkage devices, and fracture fixation devices. Spinal needles and passing sutures are helpful tools that have been adapted from other arthroscopic repair techniques.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


