CHAPTER 2 Diagnostic Elbow Arthroscopy and Loose Body Removal
Advances in elbow arthroscopy have enabled surgeons to treat a broad spectrum of disorders that were once thought to be unsafe using arthroscopic techniques.1 Although technically demanding, advances in surgical technique and arthroscopic equipment and an improved understanding of neurovascular and joint anatomy have made this procedure safer and more effective than its initial applications.
The indications for elbow arthroscopy continue to evolve. In previous years, elbow arthroscopy was mainly used for removal of loose bodies,2–8 synovectomy,9,10 lysis of adhesions,11,12 excision of osteophytes,13,14 débridement of osteochondritis dissecans lesions,6,15–17 radial head resection,18 plica excision,19,20 instability,21 septic arthritis,22 and diagnostic arthroscopy for complex elbow pain.6 These indications have been expanded to include débridement, drilling, and autograft replacement for osteochondritis dissecans; débridement and repair of lateral epicondylitis; and débridement of radiocapitellar arthritis, olecranon bursectomy, arthrofibrosis, and fractures of the radial head, capitellum, and distal humerus.6,8,9,23
Removal of loose bodies is perhaps the most common and rewarding arthroscopic procedure involving the elbow.4,24,25 Arthroscopic identification and removal of such impediments to joint motion has significant advantages. Scar formation is limited by the small portal site incisions needed to fully evaluate and perform loose body removal. All compartments of the elbow are readily accessible for a thorough evaluation of intra-articular pathology with the arthroscope.
PATIENT EVALUATION
History and Physical Examination
A careful history, physical examination, and appropriate imaging are imperative before arthroscopic excision of loose bodies and osteophytes within the elbow joint. On presentation, patients with loose bodies often complain of pain, stiffness, catching, clicking, and locking of the elbow joint. Physical examination findings often include sometimes subtle losses of flexion, extension, and a small effusion that can be detected most often in the posterolateral gutter.26
When preparing for arthroscopic loose body excision, a detailed history of past surgical ulnar nerve neurolysis or transposition, along with physical examination for subluxation of the ulnar nerve, cannot be overemphasized. A subluxated or dislocated ulnar nerve can be found in 16% of the normal population.26 Awareness of these variations in normal anatomy is essential to prevent iatrogenic neural injury.
Diagnostic Imaging
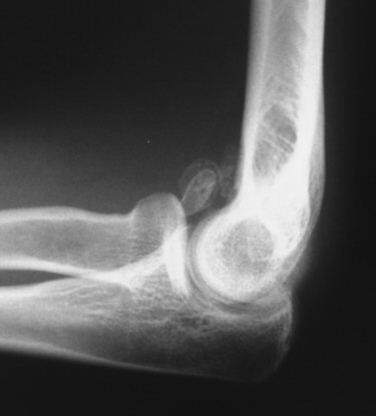
Anteroposterior and lateral radiographs of the elbow should be routinely obtained (Fig. 2-1). However, standard imaging fails to demonstrate almost 30% of loose bodies, and in such cases, further diagnostic testing, such as computed tomography or magnetic resonance imaging, may be warranted.4,5,26,27 In most cases, loose bodies are found in the coronoid fossa, olecranon fossa, and posterior aspect of the lateral gutter. Although careful attention must be paid to these areas, loose bodies often migrate and may be difficult to see on imaging. In some cases, arthroscopic evaluation may prove to be the gold standard for demonstrating loose bodies when classic presentations are encountered.26
TREATMENT
Indications and Contraindications
Patients who have failed conservative management for loose bodies within the elbow are candidates for elbow arthroscopy and loose body removal. However, before surgical intervention is undertaken, the treating surgeon must ascertain the cause of these impediments to normal joint motion. Loose bodies may be the result of osteochondritis dissecans, degenerative arthritis, synovial chondromatosis, or trauma.4,5,28 A carefully formulated plan to address the primary underlying pathology at the time of surgery can prevent the future formation of loose bodies.28
Absolute contraindications to elbow arthroscopy include any variation in the normal bony or soft tissue anatomy that precludes the safe insertion of the arthroscope into the elbow joint.28 Other contraindications include an ankylosed elbow joint that would preclude joint distention and local soft tissue infection in the area of portal sites. Prior ulnar nerve transposition is a relative contraindication if it interferes with portal positioning.28 However, elbow arthroscopy can be used if the ulnar nerve is identified with surgical dissection before portal creation.
Elbow Arthroscopy
Anesthesia
General anesthesia or regional blocks are the most common methods used in elbow arthroscopy. General anesthesia is more commonly used because of the flexibility it permits with respect to patient positioning and postoperative examination. The prone and lateral decubitus positions are poorly tolerated in awake patients, and these positioning methods are most amenable to general anesthesia.12 Use of general anesthesia in the absence of a neurologic block enables immediate postoperative neurologic examination.
Patient Positioning
Supine Position.
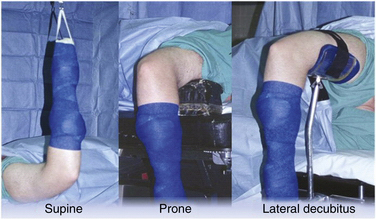
Supine positioning for elbow arthroscopy was first described in 1985.9 After supine positioning of the patient on the operating table, the operative extremity is lateralized on the operating table so that the shoulder is placed at the edge of the bed. The patient is secured, and all pertinent prominences are appropriately padded. The operative extremity is placed in 90 degrees of shoulder abduction, 90 degrees of elbow flexion, and neutral forearm rotation, and a nonsterile arm tourniquet is applied (Fig. 2-2). Traction is facilitated with the use of a traction device.
The supine position offers several advantages to the elbow arthroscopist.2 A three-dimensional understanding and application of elbow anatomy is facilitated by the anatomic and familiar position of the elbow. This also benefits the surgeon if open procedures follow. This position enables quick access to the patient’s airway and the choice of multiple effective anesthetic regimens. Drawbacks of the supine position include the necessity of a traction setup, which makes manipulating the elbow cumbersome, and the inability to easily visualize and work in the posterior compartment.
Prone Position.
The prone position was first described in 1989 as an alternative method for positioning.29 The aims of this method were to improve access to the posterior compartment of the elbow and eliminate the need for a traction device for intraoperative elbow manipulation.
The patient is initially intubated on a gurney and rolled to the prone position on the operating table. The face and chest are padded and supported by a foam airway and head positioner and by padded chest rolls. The nonoperative extremity is brought into 90 degrees of shoulder abduction and neutral rotation with the elbow in 90 degrees of flexion. The elbow and wrist are supported by a padded arm board. On the operative side, an arm board is placed parallel to the operating table centered at the shoulder level. A nonsterile arm tourniquet is applied, and the arm is placed in 90 degrees of shoulder abduction and neutral rotation. The arm is supported at the middle humeral level by a padded bolster attached the operating table or by a rolled towel bump that is positioned on top of the arm board, which suspends the elbow in 90 degrees of flexion (see Fig. 2-2).
The prone position has several advantages. With the arm freely hanging, the elbow is easily manipulated from flexion to full extension. This can be done without the use of a traction setup or arm positioner and without an assistant. The posterior compartment of the elbow is easily accessible. Flexion of the elbow allows the neurovascular structures to sag anteriorly, providing a greater margin of error when establishing anterior portal sites. As with the supine position, open procedures are easily conducted on the medial and lateral sides of the elbow if necessary.30
Lateral Decubitus Position.
The lateral decubitus position was described by O’Driscoll and Morrey in 1993.30 The aim of this position was to exploit the benefits of the supine and prone positions while avoiding the major pitfalls inherent to each setup. The patient is initially placed in the lateral decubitus position with the aid of a bean bag or sand bag kidney rests and secure taping or strapping. An axillary roll is appropriately placed. The operative extremity is positioned over an arm holder or over a padded bolster, with the shoulder internally rotated and flexed to 90 degrees. The elbow is maintained in 90 degrees of flexion (see Fig. 2-2).
Arthroscopic Portals
At the outset of any elbow arthroscopic procedure, various landmarks must be localized and marked. The ulnar nerve, radial head, olecranon, lateral epicondyle, and medial epicondyle should be traced with a marking pen. Palpating and outlining the course of the ulnar nerve cannot be overemphasized to ensure that it is not subluxated or subluxatable. An 18-gauge spinal needle is used to insufflate the elbow joint with approximately 20 to 30 mL of sterile saline. This can be accomplished through a posterior injection into the olecranon fossa or through the lateral soft spot portal site, which is bounded by the radial head, lateral epicondyle, and olecranon (Fig. 2-3). The intra-articular injection can be confirmed by resistance to further inflow and often by the slight extension of the elbow seen as fluid is introduced. Distention of the joint capsule further protects the anterior neurovascular structures by displacing them anteriorly and farther away from planned portal sites.32,33





