in the coronal plane due to advanced medial plateau concavity. This finding indicates that it will not be possible to significantly unload the medial compartment, and a majority of the weight-bearing loads will be confined to the medial compartment. Marked patellofemoral symptoms contraindicate an HTO. Medical contraindications include diabetes, rheumatoid arthritis, autoimmune diseases, and malnutrition states.
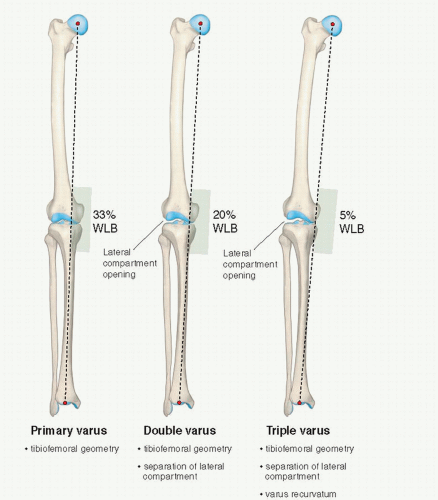 FIGURE 76.1. Schematic illustration of primary, double, and triple varus knee angulation. WBL, weight-bearing line. (Reprinted from Noyes FR, Barber-Westin SD. Primary, double, and triple varus knee syndromes: diagnosis, osteotomy techniques, and clinical outcomes. In: Noyes FR, ed. Noyes Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. Philadelphia, PA: Saunders; 2009:821-895.) |
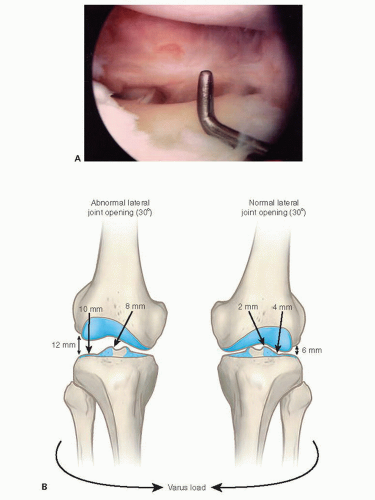 FIGURE 76.2. Arthroscopic gap test for determining the amount of lateral joint opening. (Reprinted from Noyes FR, Barber-Westin SD. Primary, double, and triple varus knee syndromes: diagnosis, osteotomy techniques, and clinical outcomes. In: Noyes FR, ed. Noyes Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. Philadelphia, PA: Saunders; 2009:821-895.) |
If separation of the lateral tibiofemoral joint is observed, it is necessary to subtract the lateral compartment opening so that the true tibiofemoral osseous alignment is determined and a valgus overcorrection is avoided. Other radiographs include a lateral at 30° knee flexion, weight-bearing posteroanterior at 45° knee flexion, and patellofemoral axial views. Telos medial or lateral stress radiographs may also be required of both knees. The height of the right and left patella is measured on lateral radiographs to determine if an abnormal patella infera or alta position exists (1).
Table 76.1 Preoperative planning | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
slope is required before cruciate ligament surgery or other conditions discussed. Empirically, a tibial slope greater than two standard deviations above normal (e.g., a tibial slope of 15° or greater) usually requires correction.
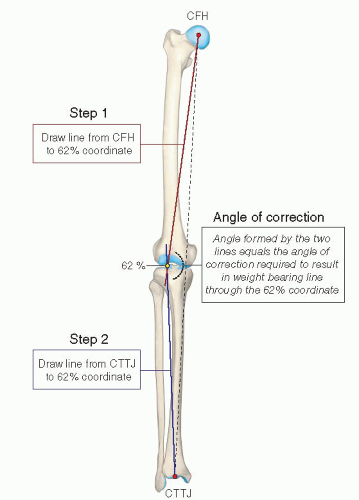 FIGURE 76.3. Graphic depiction of the method used to calculate the correction angle of an HTO using a full-length anteroposterior radiograph of the lower extremity. The lines from the centers of the femoral head (CFH) and tibiotalar joint (CTTJ) converge in this example at the 62% coordinate. (Reprinted from Noyes FR, Barber-Westin SD. Primary, double, and triple varus knee syndromes: diagnosis, osteotomy techniques, and clinical outcomes. In: Noyes FR, ed. Noyes Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. Philadelphia, PA: Saunders; 2009:821-895.) |
between the tibial tubercle and the posteromedial tibial cortex, starting 1-cm inferior to the joint line. Once the dissection is complete, a Keith needle is placed in the anteromedial joint just above the tibia, and the distance is marked on the desired point of the osteotomy along the anteromedial cortex. A second Keith needle is placed at the posteromedial tibial joint space, and the same millimeters are marked to provide a measurement of the tibial slope. The two marks are connected to provide the osteotomy line perpendicular to the tibial slope.
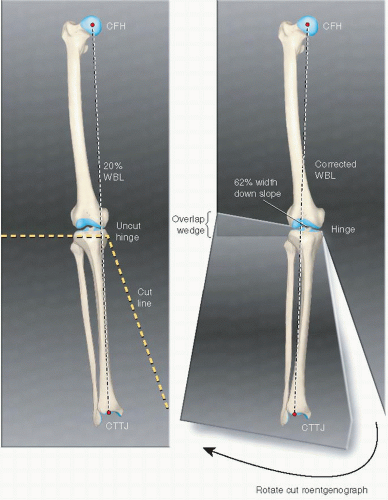 FIGURE 76.4. Graphic depiction of an alternative method used to calculate the correction angle of an HTO using a full-length anteroposterior radiograph of the lower extremity. The roentgenograph is cut to allow the center of the femoral head (CFH), the 62% coordinate, and the center of the tibiotalar joint (CTTJ) to become colinear. The angle of the resulting wedge of roentgenograph overlap equals the desired angle of correction. The example is provided for a closing wedge osteotomy. The same technique is used for an opening wedge osteotomy where the medial tibial opening wedge is made to obtain the desired correction. (Reprinted from Noyes FR, Barber-Westin SD. Primary, double, and triple varus knee syndromes: diagnosis, osteotomy techniques, and clinical outcomes. In: Noyes FR, ed. Noyes Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. Philadelphia, PA: Saunders; 2009:821-895.) |
Related posts:
 Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Multidirectional and Posterior Shoulder Instability
The Stiff Shoulder: Planning and Treatment Options
Arthroscopic Suprascapular Nerve Release
Arthroscopic Management of Lateral Epicondylitis
Clinical Approach to Articular Cartilage Pathology
Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Multidirectional and Posterior Shoulder Instability
The Stiff Shoulder: Planning and Treatment Options
Arthroscopic Suprascapular Nerve Release
Arthroscopic Management of Lateral Epicondylitis
Clinical Approach to Articular Cartilage Pathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


