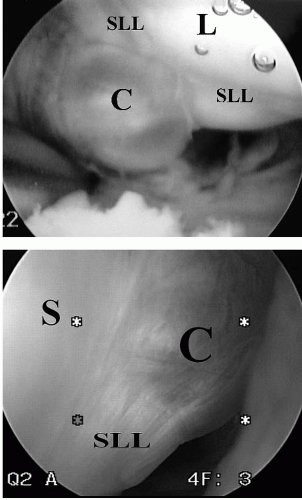
 FIGURE 41.1. Intra-articular cystic stalk as viewed from the radiocarpal joint compartment. Cysts may be (A) pedunculated or (B) sessile in appearance. C, cyst; S, scaphoid; L, lunate; SLL, scapholunate ligament. |
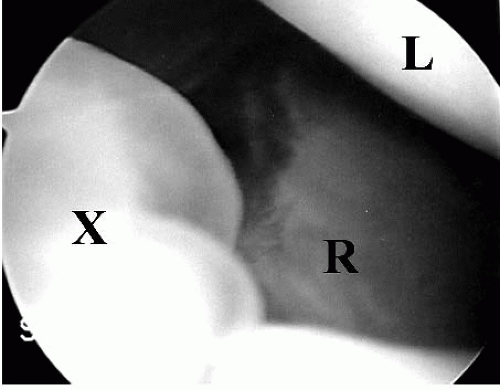 FIGURE 41.2. Diffuse cystic material and redundant capsule often occur more commonly than a discreet cystic stalk. X, cystic material and redundant capsule; R, radius; L, lunate. |
|
cyst. Palpation of the dorsal portion of the scapholunate ligament, a positive Watson scaphoid shift test, or positive straight finger resistance test may be suggestive of scapholunate ligament pathology. Cysts may resemble other pathologies such as gouty tophus, tenosynovitis, and rheumatoid pannus. A careful history and physical should be able to differentiate these conditions.
can be seen in the area where the extrinsic capsule joins the distal portion of the dorsal scapholunate ligament. This capsular reflection serves as part of the barrier between the radiocarpal and the midcarpal joints, and the protrusion located here has been termed the cystic stalk (Fig. 41.1). More often, however, one may be impressed with the amount of synovitis and redundant capsule in this area instead of an actual cystic stalk (Fig. 41.2).
Related posts:
 Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Multidirectional and Posterior Shoulder Instability
The Stiff Shoulder: Planning and Treatment Options
Arthroscopic Suprascapular Nerve Release
Endoscopic Carpal Tunnel Release: Chow Technique
Wrist Arthroscopy Basics: Anatomy, Portals, and Diagnostic Arthroscopy
Acromioclavicular Separations: Arthroscopic Reconstruction of The Acromioclavicular Joint
Multidirectional and Posterior Shoulder Instability
The Stiff Shoulder: Planning and Treatment Options
Arthroscopic Suprascapular Nerve Release
Endoscopic Carpal Tunnel Release: Chow Technique
Wrist Arthroscopy Basics: Anatomy, Portals, and Diagnostic Arthroscopy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


