Open Reduction Internal Fixation of the Sacroiliac Joint and Sacrum
Open Reduction Internal Fixation of the Sacroiliac Joint and Sacrum
Henry Claude Sagi
DEFINITION
Pelvic fractures are serious injuries associated with a diverse assortment of morbidities and mortality rates ranging from 0% to 50%.
Fractures and dislocations of the pelvis involve, in broad terms, injuries to the anterior and posterior structures of the pelvic ring.
Injuries to the anterior pelvic ring include symphyseal disruption and pubic body or rami fractures.
Injuries to the posterior pelvic ring involve iliac wing fractures, sacroiliac (SI) joint dislocations and fracturedislocations, and sacral fractures.
The implications and treatment options vary widely depending on the spectrum of fracture patterns, the degree of displacement and potential instability, and associated injury patterns.
This chapter will focus specifically on the treatment of displaced sacral fractures and SI joint dislocations.
ANATOMY
The pelvis is a ring structure composed of the two hemipelves
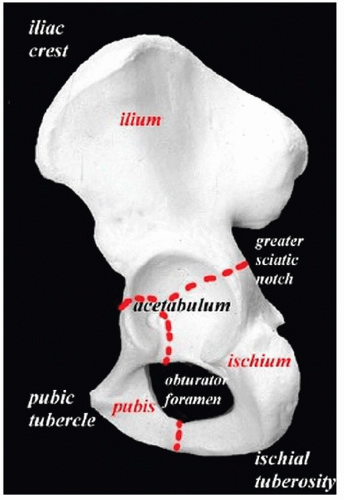
(innominate bones) and the sacrum. Each hemipelvis is the culmination and fusion of the three embryonic bony elements: the ilium, the pubis, and the ischium (FIG 1).
The two hemipelves are joined anteriorly at the pubic symphysis
(a symphyseal joint), whereas posteriorly, they articulate with the wings, or alae, of the sacrum via the SI joints to complete the pelvic ring (FIG 2A,B).
The sacrum represents the terminal structural segment of the spinal column that connects the pelvis and extremities to the trunk and spine.
The sacrum is the caudal segment of the axial skeleton. It is, therefore, a spinal element and subject to segmentation abnormalities and dysmorphism.
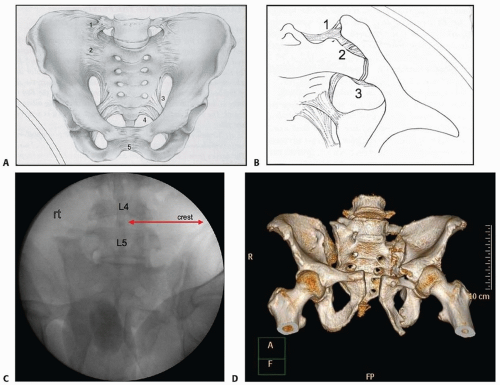
Most commonly, segmentation anomalies such as a lumbarized S1 or a sacralized L5 will be present (FIG 2C,D). The only way to be sure which defect, if any, is present, is to count down from the first thoracic vertebrae, which is the first vertebra to have transverse processes that are inclined cephalad.
As a general rule of thumb, however, the top of the iliac crest is usually at the same level as the L4 or L5 disc space. This rule can be used to judge the presence of dysmorphism (see FIG 2C).
These issues are pertinent to interpretation of the radiographic landmarks required to safely place iliosacral screws (see discussion later).
Being wedge-shaped, the sacrum forms a keystone articulation with the innominate bones.
By virtue of this shape and their orientation, the SI joints are inherently unstable with respect to the bony constraints, and the maintenance of posterior pelvic ring integrity is wholly dependent on the support provided by the ligamentous structures (see FIG 2A).
The pelvic ligaments are structured and positioned to resist these deformations as static stabilizers of the pelvis. There are no specific dynamic stabilizers of the pelvic ring.
With axial loading, the natural tendency is for each hemipelvis to externally rotate and translate in a cephalad and posterior direction. During two-legged stance, the symphysis is under tension and the SI joints experience compression superiorly and tension inferiorly. During single-leg stance, the symphysis is under compression and shear, whereas the SI joints are under tension superiorly and compression inferiorly.
The SI ligaments (anterior, posterior, and intra-articular ligaments) are the strongest ligaments in the body, with the posterior SI ligaments being the most important in resisting posterior and cephalad displacement (see FIG 2B).
The symphyseal ligaments (themselves contributing no more than 15% to pelvic ring stability), the sacrotuberous ligaments, and the sacrospinous ligaments resist external rotation.13,31
FIG 1 • The three embryonic bones (pubis, ischium, ilium) fusing to form the innominate bone or hemipelvis.
FIG 2 • A. The two innominate bones and sacrum forming the pelvic ring with supporting ligaments. 1, iliolumbar; 2, SI; 3, sacrospinous; 4, sacrotuberous; and 5, symphyseal ligaments. B. SI joint ligaments. 1, posterior; 2, intra-articular; 3, anterior SI ligaments. C. Intraoperative fluoroscopy showing unilateral segmentation anomaly with partial sacralization of L5 and the level of the crest still at L4-L5. D. Three-dimensional CT reconstruction showing segmentation anomaly.
The bladder is immediately posterior to the pubic bodies and symphysis, separated only by a thin layer of fat and the potential space of Retzius.
The relationship of the L5 nerve root to the superior aspect of the sacral ala as it courses to join the lumbosacral plexus is a key anatomic feature that must be kept in mind during reduction and stabilization of posterior pelvic ring injuries (FIG 3A,B).
FIG 3 • A,B. Neurovascular structures around the posterior pelvic ring. Note intimate relationship of L5 nerve root to sacral ala.
The sacral nerve roots course from posterior to anterior, medial to lateral, and proximal to distal as they traverse the upper sacral nerve root tunnels. As they exit the sacrum, the nerve roots lay on the inferior and lateral aspect of the foramina.
The superior gluteal artery is immediately lateral to the inferior aspect of the SI joint as it arises from the internal iliac artery to exit the greater sciatic notch with the superior gluteal nerve.
PATHOGENESIS
The SI ligaments are the most resilient in the human body and therefore must be subject to substantial forces and energy transmission to result in disruption.
Anteroposterior (AP) compression of the pelvic ring causing external rotation of the innominate (which may or may not be coupled with a vertical shearing force) is the most common cause of SI joint dislocation.
Sacral fractures, however, can occur in three distinctly different situations.
Insufficiency fractures of the sacrum arise secondary to failure through excessively osteoporotic or osteopenic bone.
Stress fractures of the sacrum resulting from fatigue and cyclic failure of normal bone in high-level athletes or military recruits
Traumatic disruptions resulting from high-energy lateral or anteroposterior compression (APC) and/or vertical shear injuries such as (in order of decreasing frequency) motorcycle crashes, auto-pedestrian collisions, falls from height, motor vehicle accidents, or crush injuries.13,31
NATURAL HISTORY
Pelvic fractures occur in at least 20% of blunt trauma admissions, most frequently in young males.
They can result in small insignificant fractures of the pubic rami with no compromise of pelvic ring stability, or major injuries and disruptions that can be associated with lifethreatening bleeding and/or visceral injury.
The pelvic ring encloses the true pelvis (organs contained below the pelvic brim, extraperitoneal) and the false pelvis (organs contained above the pelvic brim, both peritoneal and retroperitoneal).
The most commonly associated injuries to structures contained within the true pelvis are the internal iliac arterial and venous systems and branches, the bladder (20%) and urethra (14%), the lumbosacral plexus, and the rectum and vaginal vault (open pelvic fractures).
Injuries to structures within the false pelvis as a direct result of the pelvic fracture are uncommon, but severe iliac wing fractures with abdominal wall disruption can result in intestinal injury and even entrapment.
Morbidity and mortality from pelvic fractures can be quite high and is most commonly secondary to pelvic hemorrhage.
The mortality rate associated with pelvic fracture with an associated bladder rupture approaches 35% in some series.
The mortality rate of open pelvic fractures involving the perineum used to be as high as 50%, but this has decreased to approximately 2% to 10% with the liberal use of diverting colostomies and more advanced stabilization techniques.
Neurologic injury to the lumbosacral plexus can lead to significant sensorimotor dysfunction involving the extremities, bowel, bladder, and sexual organs.
Because of these associated neurovascular and visceral injuries, pelvic fractures often result in prolonged recovery periods, significant chronic pain, permanent disability, and loss of psychological and socioeconomic structure.5,7,9,19,20,21
PATIENT HISTORY AND PHYSICAL FINDINGS
Any patient presenting with a history of trauma or satisfying criteria for a Trauma Alert in the emergency department should be suspected of having a pelvic fracture until otherwise ruled out by radiologic and physical examination.
The physical examination should follow the primary and secondary survey of the advanced trauma life support protocol.1
Examination of a patient suspected of having a pelvic fracture should be divided into the examination of the abdomen, pelvic ring, perineum, rectum, vagina, and lower extremities.
The abdominal examination should elucidate the following:
Tenderness, fullness, or rigidity
Abdominal wall disruptions, defects, or open wounds
Flank ecchymosis
Presence of internal degloving or a Morel-Lavallée lesion (separation of the subcutaneous tissues from the underlying muscular fascia). This can be recognized by subcutaneous fluctuance or a fluid wave and, later, extensive ecchymosis.
The rectal and vaginal examination should consider the following:
The position of the prostate (a high-riding prostate may be a sign of urethral injury)
Palpable bony fragments perforating the rectal or vaginal mucosa
Defects or tears in the wall of the rectum or vagina indicating possible bony penetration
Rectal or vaginal bleeding indicating possible tears or bony penetration
Urethral bleeding at the meatus indicating possible urethral or bladder disruption
Scrotal or labial swelling and ecchymosis indicating pelvic hemorrhage (FIG 4)
Rectal tone, perianal sensation, voluntary sphincter control, and bulbocavernosus reflex to assess for the presence of cauda equina syndrome or lower sacral nerve root injury
FIG 4 • Scrotal ecchymosis from internal pelvic hemorrhage.
Examination of the pelvic ring and extremities should focus on the following key factors:
Palpable internal or external rotation instability of the pelvic ring with manually applied AP and lateral compressive forces on the iliac wings/crests. However, in an awake patient or with hemodynamic instability, multiple forceful attempts at manipulating the pelvis is not recommended, as this will be very uncomfortable to the patient and may exacerbate ongoing pelvic hemorrhage (Table 1).
Leg length discrepancy with asymmetric internal or external rotation
Neurologic status in patients able to comply can be assessed as follows:
L1-L2: iliopsoas (hip flexors) and upper anterior thigh sensation
L3-L4: quadriceps (knee extensors) and lower anterior thigh/medial calf sensation
L5: extensor hallucis longus, digitorum longus (toe dorsiflexion), peroneal eversion (although this can have a strong
L4 component), and lateral calf/dorsum of foot sensation
S1: gastrocsoleus complex (ankle plantar flexion) and posterior calf sensation
S2-S3: flexor hallucis and digitorum longus (toe plantar flexion) and sole of foot sensation
Table 1 Methods for Examining the Pelvis for Stability
Examination
Technique
Illustration
Grading
Significance
External rotation pelvic instability
Legs are positioned flexed, abducted, and externally rotated. Hands are placed on the iliac crests and an AP force is applied.
N/A
Palpable widening of the pelvis or increased SI joint space or symphyseal widening is seen on simultaneous fluoroscopic images with the C-arm.
Internal rotation pelvic instability
Legs are positioned extended, adducted, and internally rotated. Hands are positioned over the greater trochanters and a lateral to medial compressive force is applied.
N/A
Palpable instability of the pelvis or a decrease in SI joint space or symphyseal diastasis is seen on simultaneous C-arm images.
Vertical instability
Legs are positioned extended. While one extremity is supported at the heel, traction is applied to the other.
N/A
A visual change in leg length discrepancy can be seen in some cases. Otherwise, simultaneous C-arm images may disclose one acetabulum or iliac crest at a different level than the other.
AP, anteroposterior; SI, sacroiliac.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain Radiographs
The standard AP (pelvis) view should be part of the initial trauma series screening. With enough experience, many of the injuries to the posterior pelvic ring can be diagnosed with this single projection (FIG 5A).
A good AP radiograph should have the pubic symphysis colinear with the sacral spinous processes.
This allows side-to-side comparison of bony landmarks to aid in diagnosis of subtle displacements of the sacrum or SI joint.
The cortical density of the pelvic brim and iliopectineal line should be traced back to its intersection with the lateral margin of the sacral ala.
This intersection should be at the same level (usually the superior margin of the S2 foramen) bilaterally.
Asymmetry in the SI joint space and the appearance of the sacral foramina should alert the surgeon to the possibility of an SI joint dislocation or sacral fracture.
Fractures of the L5 transverse process may be a clue to a vertical shear or severe open book pelvic injury that has avulsed the transverse process via the iliolumbar ligament.
FIG 5 • A. AP pelvis radiograph. Ideal film should have symphysis aligned with sacral spinous processes. B. Inlet pelvic radiograph. Note sacral promontory and alar regions. C. Outlet pelvic radiograph. Note sacral foramina and SI joints. Ideal image should have top of symphysis-rami at the S2-S3 level. D. Axial CT scan of transforaminal (Denis zone 2) sacral fracture. E. Axial CT scan of SI joint dislocation. Note diastasis of anterior and posterior joint.
Symphyseal diastasis or displaced rami fractures should alert the examiner to additional injuries in the posterior ring even though they may not be readily apparent on the initial radiographic evaluation.
The inlet projection is taken with the x-ray beam directed caudally approximately 45 degrees to the radiographic film.
A true inlet view of the pelvis, however, may require variations on this degree of angulation because of the variations pelvic obliquity, sacral inclination, and dysmorphism. A perfect inlet view will show the anterior cortices of the sacral bodies superimposed.
This view simulates a direct view into the pelvis from above along its longitudinal axis (see FIG 5B).
The inlet view is helpful in imaging the following:
External or internal rotation of the hemipelvis
Opening of the SI joint or an impaction fracture of the sacrum
“AP” displacement or translation of the hemipelvis (see the following texts)
The outlet projection of the pelvis is obtained by directing the x-ray beam approximately 45 degrees cephalad to the radiographic film.
A true outlet view of the sacrum, however, may require variations in this degree of angulation because of the variations in pelvic obliquity, sacral inclination, and dysmorphism. A perfect outlet view will show the sacral foramina as full circles.
This view simulates looking at the sacrum and SI joints directly en face (FIG 5C).
The outlet view is helpful in imaging the following:
Cephalad or “vertical” shift of the hemipelvis
Sacral fractures relative to the foramina
Flexion-extension deformity of the hemipelvis
It is important to remember that these radiographs are taken at about 45 degrees to the long axis of the patient’s body.
Therefore, a given amount of translation or displacement seen on the inlet or outlet view is in fact the sum of displacement vectors in both the coronal and axial planes. For example, “posterior” shift seen on the inlet projection is in fact a combination of both posterior and cephalad translation relative to the long axis of the body.
Computed Tomography
Computed tomographic (CT) scanning is imperative in any suspected pelvic ring injury.
As the pelvis is a ring structure, any disruption in one location (no matter how seemingly insignificant) must (by virtue of ring structure mechanics) be accompanied by disruption in another location (pathologic fractures excluded).
Three-millimeter axial sections (or 3 mm of vertical travel per 360-degree rotation of the gantry in a spiral CT) are recommended to disclose the majority of significant injuries (FIG 5D,E).
FIG 6 • A. AP radiograph of patient with a U-shaped sacral fracture. Note inlet view of proximal sacrum but outlet appearance of caudal sacrum. B. Axial and sagittal CT scan reconstructions of the same patient with a U-shaped sacral fracture.
Another important point to bear in mind is the appearance of the sacrum on the AP projection.
If one sees a paradoxical inlet view of the upper sacrum and outlet view of the distal sacrum, a lateral x-ray and
CT scan with sagittal reconstructions must be performed to rule out an occult sacral fracture-dislocation (U-shaped sacral fracture otherwise known as spinal-pelvic dissociation) (FIG 6A,B).
Bilateral sacral alar fractures noted on an axial CT image of the sacrum should alert the surgeon to a U-shaped sacral fracture dislocation or spinal-pelvic dissociation.
Retrograde Urethrography and Cystography
Retrograde urethrography and cystography are mandatory in pelvic fractures with ring disruption to rule out urethral/bladder injury.
The Foley catheter is partially inserted into the urethra, and the balloon is inflated with 2 to 3 mL of sterile saline to occlude the urethra. Ten to 15 mL of water-soluble contrast is then injected into the urethra and the outlet view of the pelvis is repeated.
If no extravasation is seen, the catheter is advanced into the bladder with injection of a further 300 mL of water-soluble contrast to rule out a bladder rupture. If no contrast extravasation is noted, the bladder is drained with the catheter, and any residual dye is noted.
If passage of the catheter is not possible or there is a tear of the urethra or bladder neck, suprapubic catheterization should be performed well above the umbilicus if possible (to avoid contamination of potential future anterior pelvic operations).
Pelvic Angiography
Angiography is indicated in those patients exhibiting persistent hemodynamic instability despite10
Adequate volume resuscitation
Other sources of hemorrhage being ruled out (abdomen, thorax, and long bone fractures)
Attempts to “close” the pelvic ring (see the following texts) have failed to stop pelvic hemorrhage
Most cases of pelvic hemorrhage (85%) arise from venous bleeding and are not amenable to angiographic embolization.
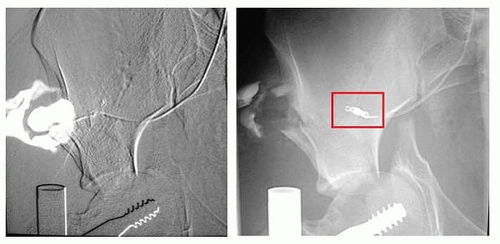
Arterial bleeding is usually from branches of the internal iliac system (median sacral, superior gluteal, pudendal, or obturator arteries) (FIG 7).
Arterial hemorrhage is more common in patients older than 65 years.
If diagnostic peritoneal lavage is being performed to rule out abdominal hemorrhage, then it must be performed above the umbilicus and arcuate line to avoid false-positive results from pelvic hemorrhage.
NONOPERATIVE MANAGEMENT
As a general rule, traumatic complete SI dislocations should not be managed nonoperatively.
Progressive cephalad displacement of the hemipelvis will result in pelvic malunion. Leg length inequality, chronic mechanical low back and buttock pain, pelvic obliquity with sitting imbalance, and dyspareunia are common complaints when the hemipelvis and ischial tuberosities are malpositioned.
For patients in extremis, sepsis, or critical medical comorbidity, nonoperative therapy may be required until the patient can tolerate pelvic reconstruction procedures. This helps to reduce the pelvic deformity, stabilize the pelvic hemorrhage and clot, and improve patient comfort in the acute resuscitative period.2 In such cases, the pattern of deformity dictates the maneuvers to be used to minimize deformity.
Patients with vertical instability should be placed into balanced longitudinal skeletal traction in an attempt to reduce and/or prevent further cephalad displacement. Traction is also an effective adjunct for hemostasis during resuscitation. Distal femoral skeletal traction is preferable.
Patients with external rotation deformity of the pelvic ring (ie, an open book pelvis) should be treated with circumferential wrapping with either a sheet or commercially available pelvic binder (ie, the T-POD pelvic binder, PYNG Medical Corporation, Richmond, BC, Canada) placed over the greater trochanters. Frequent skin checks are mandatory to prevent full-thickness pressure ulceration and as such, they are rarely, if ever, indicated for definitive treatment (FIG 8).
FIG 7 • Angiogram showing extravasation and embolization of superior gluteal artery. (Courtesy of Prof. Johannes Reuger, with permission.)
Anterior pelvic external fixators can be applied either in the trauma bay or the intensive care unit (ICU) for patients in extremis.
Anterior pelvic external fixators are good for controlling external and internal rotation of the anterior pelvic ring.
Thus, the surgeon may elect to use them definitively in situations where the SI joint is only disrupted through the anterior SI ligaments (a type 2 injury with no vertical or sagittal plane instability) or with certain lateral compression injuries where the sacral fracture is stable by virtue of its impaction.
By themselves, however, anterior external fixators are not effective in controlling the posterior pelvic ring, and if applied incorrectly, can make some pelvic deformities worse.16,29
Only gold members can continue reading. Log In or Register to continue








 Volar Plating of Distal Radius Fractures
Volar Plating of Distal Radius Fractures




