This injury was initially reported by Giovanni Monteggia in 1814 as a fracture of the ulna associated with an anterior dislocation of the radial head.6
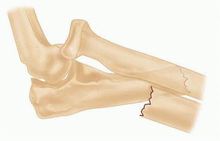
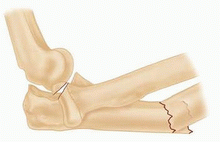
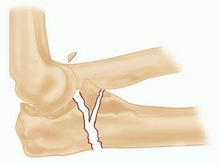
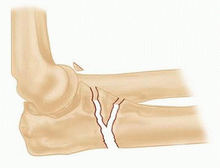
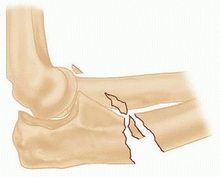
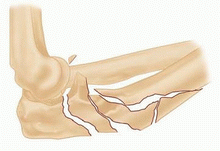
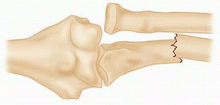
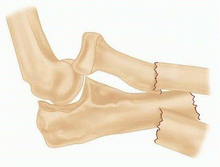
The term “Monteggia lesions” was coined by Bado to describe any fracture of the ulna associated with a dislocation of the radiocapitellar joint.1
The Bado classification of Monteggia lesions,1 with the Jupiter subclassification of type II fractures,4 is shown in Table 1.
Equivalent injuries in adults
Variable pathology that is thought to be equivalent to injuries classified by the Bado system
Equivalent injuries do not always fall within the traditional definition of a Monteggia fracture in that they do not always have a concomitant radiocapitellar dislocation.
Therefore, it can be argued that these injuries are not necessarily equivalent to Monteggia fractures.
Type I and II injuries are the only ones that have equivalent injury patterns.
The exact mechanism of injury for Monteggia fractures is controversial.
Proposed mechanisms of injury for type I injuries include the following:
Direct blow to the posterior aspect of the elbow
Fall on outstretched arm with hyperpronated hand (forearm pronation levers radial head anteriorly)
Fall on outstretched arm
Violent contraction of biceps pulling radial head anteriorly
Proposed mechanism for type II injuries: hypothesized to occur when a supination force tensions the ligaments that are stronger than bone
Proposed mechanism for type III injuries: direct blow to the inside of the elbow with or without rotation
The initial examination should systematically evaluate:
Skin integrity
Neurovascular status of the extremity
Bony injury
Ulna fracture
Injury pattern
Noncomminuted
Comminution
Associated injury to key structural elements of the ulna (coronoid, olecranon)
Radial head injury
Isolated dislocation without fracture
Radial head or neck fracture
Plain radiographs (FIG 1): Orthogonal radiographs of the elbow, forearm, and wrist are required.
Ulna fracture is easily identified.
Radial head fracture or dislocation can be subtle, especially if radial head dislocation reduces.
Computed tomography (CT) scans can be helpful to determine the extent of the bony injury and the location of fracture fragments. They are particularly helpful in fractures involving the coronoid, olecranon, and radial head.
3D CT reconstructions provide information on the spatial relationship of fracture fragments in comminuted fractures.
Isolated ulna fracture
Nightstick fracture
Olecranon fracture
Fracture-dislocation of the elbow (“terrible triad” injury)
Transolecranon fracture-dislocation
Monteggia fracture-dislocations in the adult population are generally treated surgically.
Improved fixation methods and surgical technique have remarkably improved the results of surgery, making it a more reliable treatment option.
The timing of surgery depends on the condition of the soft tissues and the availability of necessary equipment and personnel.
The surgeon should define all injuries that need to be addressed.
Equipment requirements:
Small fragment plates and screws or anatomic plating system
Minifragment system
Threaded Kirchner wires
Radial head replacement
Bone graft (allograft or autograft)
Lateral decubitus position with the arm over a padded arm support (FIG 2)
Supine positioning is an alternative approach (although it is not preferred because of difficulty in maintaining the arm across the chest). If this approach is used, a saline bag under the ipsilateral shoulder will help keep the arm across the chest.
Table 1 Bado Classification of Monteggia Lesions, With Jupiter Subclassification of Type II Fractures | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
Related posts:
 Volar Plating of Distal Radius Fractures
Operative Treatment of Radius and Ulna Diaphyseal Nonunions
Open Reduction and Internal Fixation of Nonarticular Scapular Fractures
Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability
Fixation of Periprosthetic Fractures About/Below Total Hip Arthroplasty
Lateral Tibial Plateau Fractures
Volar Plating of Distal Radius Fractures
Operative Treatment of Radius and Ulna Diaphyseal Nonunions
Open Reduction and Internal Fixation of Nonarticular Scapular Fractures
Open Reduction and Internal Fixation of Fracture-Dislocations of the Elbow with Complex Instability
Fixation of Periprosthetic Fractures About/Below Total Hip Arthroplasty
Lateral Tibial Plateau Fractures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


