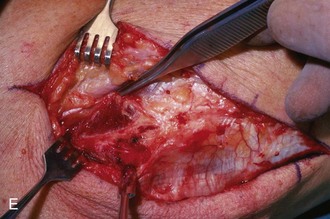
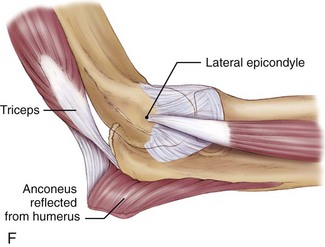
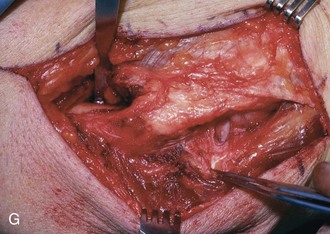
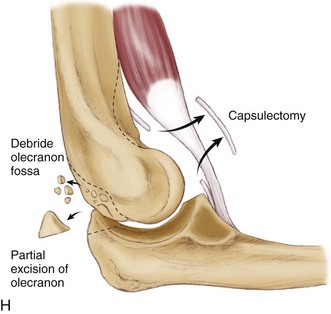
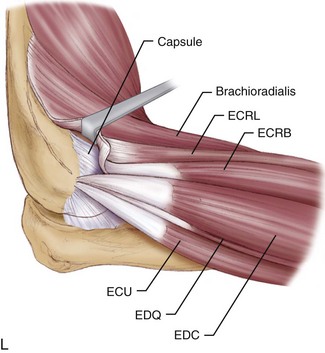
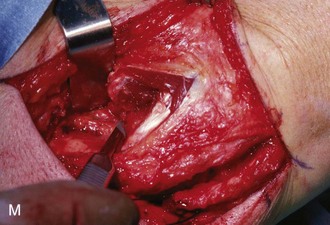
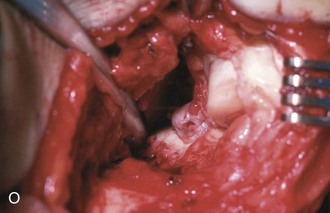
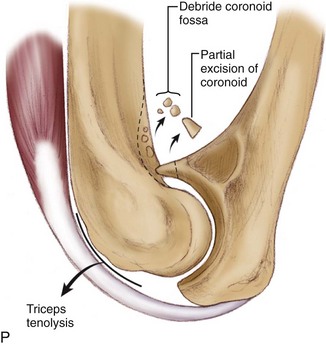
Chapter 48 Elbow motion can be restricted by contracture of the skin, capsule, and muscles; heterotopic ossification, osteophytes, or implants; articular incongruity or damage; and malunion or nonunion.1 Ulnar neuropathy is commonly associated with elbow contracture and can be precipitated or exacerbated by surgeries that increase mobility.2 The best candidate for an arthroscopic elbow contracture release is a patient with capsular contracture with or without osteophytes. Most patients with pure capsular contractures after trauma can achieve functional motion with time and exercises (including static progressive or dynamic elbow splinting).3,4 Primary elbow arthritis is uncommon. Ulnar nerve decompression is worth considering in patients with less than 100 degrees of flexion even when there are no signs or symptoms of ulnar neuropathy.2 Once the ulnar nerve has been released, performance of a capsular excision from the medial side is straightforward.5 Arthroscopic elbow contracture release is more difficult and more dangerous than open contracture release, particularly because elbow arthroscopy is an uncommon procedure at which most of us are not well practiced.6–10 For all of these reasons, operative treatment of elbow stiffness is best reserved for patients with heterotopic bone, errant implants, or ulnar neuropathy—situations in which an open procedure is preferable. It is helpful to be aware of the details of prior trauma, burn, or central nervous system injury, prior surgeries in particular. In patients with prior central nervous system injury, one must determine the ability of the patient to participate in a postoperative rehabilitation protocol.11 A painful contracture suggests arthritis or ulnar neuropathy. Numbness and dexterity problems suggest ulnar neuropathy. The quality of the skin is important, particularly in postburn contractures.12 The status of the skin with respect to prior injury and operative treatment will influence the operative tactics. When planning operative treatment of a posttraumatic contracture, we prefer to wait until the skin and scar are mobile and soft and no longer edematous or adherent. A complete motor and sensory examination of the ulnar nerve is performed, along with evaluation for a Tinel sign and an elbow flexion test. Standard anteroposterior and lateral radiographs of the elbow are usually sufficient to identify and to characterize arthritis, heterotopic ossification, and nonunions, but computed tomography is occasionally of use. In more complex cases the computed tomographic scan can help with preoperative planning.11 Three-dimensional reconstructions are particularly easy to interpret. Computed tomographic scans may be particularly useful for characterizing malunion of the articular surface of the distal humerus.13 Morrey and colleagues14 found that 15 daily activities could be accomplished with an arc of ulnohumeral motion of 30 to 130 degrees of flexion and an arc of forearm rotation of 50 degrees of pronation to 50 degrees of supination. However, these numbers should not be used to decide when to operate for elbow stiffness. Patients can adapt to and function well with much less motion,15 perhaps more so when the stiffness is in the nondominant elbow. Therefore the indication for operative contracture release is a combination of diminished elbow motion and disability directly related to stiffness. Simple capsular contracture (no heterotopic bone, no malunion or nonunion, no implants blocking motion, no ulnar neuropathy) usually responds to reassurance and encouragement of exercises, time, and static progressive or dynamic elbow splinting.3 Therefore one should never rush into operative treatment of capsular contracture; patience and frequent visits for reassurance and encouragement are worthwhile. Obvious hindrances to motion, including heterotopic bone, malunion, nonunion, prominent implants, and ulnar neuropathy, merit operative treatment. Heterotopic ossification can be resected within 3 or 4 months of injury (when it is radiographically mature and the skin is mobile with little or no edema) regardless of activity on bone scans.11,12,16,17 Stiffness associated with advanced arthrosis or unsalvageable nonunion or malunion should be treated by interpositional or prosthetic elbow arthroplasty.18,19 Elbow capsulectomy can be performed simultaneously with debridement of a deep infection. It also forms an integral part of the treatment of malunion,13 nonunion,19 and instability.20 Unstable skin can be treated with either prior or concomitant procedures to improve soft tissue coverage.12 Patients with capsular contracture who desire extension can be treated with lateral capsulectomy (Fig. 48-1).21,22 Patients with concomitant ulnar neuropathy or limitation of elbow flexion are best treated with medial capsulectomy (Fig. 48-2).5,23 Patients with heterotopic bone, prominent implants, or complex contracture that cannot be adequately released from medial or lateral alone may benefit from a combined release.5,12 Preoperative (within 24 hours) radiation therapy (a single 7-Gy dose) is administered to patients with heterotopic bone to be excised.
Open Elbow Contracture Release
Preoperative Considerations
Physical Examination
Imaging
Indications and Contraindications
Surgical Planning
Related posts:
 Knot-Tying and Suture-Passing Techniques
Arthroscopic Remplissage for Management of Engaging and Deep Hill-Sachs Lesions
Open Repair of Multidirectional Instability
Arthroscopic Meniscus Repair: Inside-Out Technique
Tendon Augmentation Devices in Rotator Cuff Repair
Arthroscopic Lateral Retinacular Release and Lateral Retinacular Lengthening
Knot-Tying and Suture-Passing Techniques
Arthroscopic Remplissage for Management of Engaging and Deep Hill-Sachs Lesions
Open Repair of Multidirectional Instability
Arthroscopic Meniscus Repair: Inside-Out Technique
Tendon Augmentation Devices in Rotator Cuff Repair
Arthroscopic Lateral Retinacular Release and Lateral Retinacular Lengthening
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Open Elbow Contracture Release