CHAPTER 16 Open bony augmentation of glenoid bone loss—the latarjet and variants—surgical technique
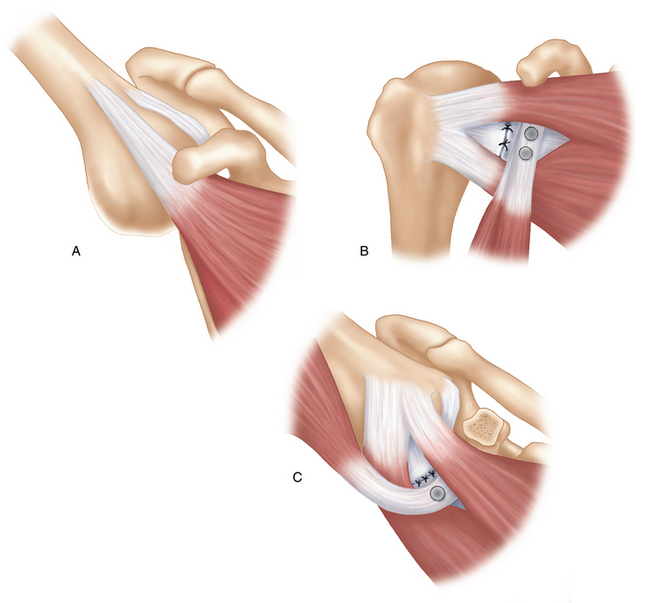
 The Latarjet procedure is effective in treating anterior instability by providing a “triple blocking” mechanism. The “triple blocking” mechanism is comprised of (1) a bone effect—increased anteroposterior (AP) diameter of glenoid articular surface, (2) a muscular effect—action of the conjoint tendon on the inferior subscapularis, and (3) a ligamentous effect—repair of the capsule to the coracoacromial ligament stump.
The Latarjet procedure is effective in treating anterior instability by providing a “triple blocking” mechanism. The “triple blocking” mechanism is comprised of (1) a bone effect—increased anteroposterior (AP) diameter of glenoid articular surface, (2) a muscular effect—action of the conjoint tendon on the inferior subscapularis, and (3) a ligamentous effect—repair of the capsule to the coracoacromial ligament stump.



Introduction
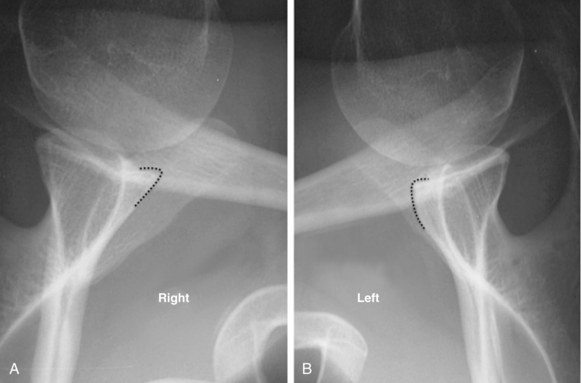
Glenoid bone loss is commonly observed in anterior instability and varies greatly in both its extent and significance.1,2 In 2000, Burkhart et al reported a recurrence rate following arthroscopic Bankart repair for anterior instability of 4% in patients without significant bone deficiency, whereas the rate of recurrence was 67% in the presence of a bone lesion.3 They defined significant glenoid bone loss as an “inverted pear glenoid” in which there is a greater than 25% loss of the inferior glenoid diameter. In the setting of anterior instability with significant bone loss, a Latarjet procedure is recommended.
In 1954, Latarjet described a coracoid bone block technique to prevent anterior dislocation, suggesting that the horizontal limb of the coracoid process be fixed to the anteroinferior margin of the glenoid with a screw.4 Augmentation of the anteroinferior glenoid with this procedure has obvious advantages in cases of glenoid bone loss. However, this “bone blocking effect” only contributes in part to the stabilizing mechanism of the Latarjet procedure. Although the precise mechanism is still unknown, the success of the intervention is explained by a triple effect first proposed by Patte et al5: (1) the effect of the conjoint tendon when the arm is abducted and externally rotated, where it acts as a sling on the inferior subscapularis and anteroinferior capsule; (2) the “bony effect,” increasing or restoring the glenoid AP diameter; and (3) the effect of repairing the capsule to the stump of the coracoacromial ligament (Fig. 16-1).
The technique described in this chapter includes a number of modifications from the original, most notably the use of two screws instead of one to provide stable fixation of the coracoid and utilization of a subscapularis splitting approach. Performing the Latarjet procedure through a horizontal split in the subscapularis preserves the continuity of the muscle fibers and allows for immediate postoperative range of motion exercises in external rotation. Numerous additional variations have been proposed relating to the subscapularis management, the position and alignment of the coracoid process, including intra- or extraarticular placement, methods of coracoid fixation, the management of the capsulolabral structures, and performing the procedure arthroscopically. Regardless of which specific variations are used, a precise surgical technique is essential to avoid potential complications. With appropriate patient selection, the Latarjet procedure can be expected to prevent recurrent anterior instability without the loss of external rotation in more than 98% of cases.6
Indications/contraindications
Preoperative history, examination, and radiographic findings
Preoperative history
Examination findings
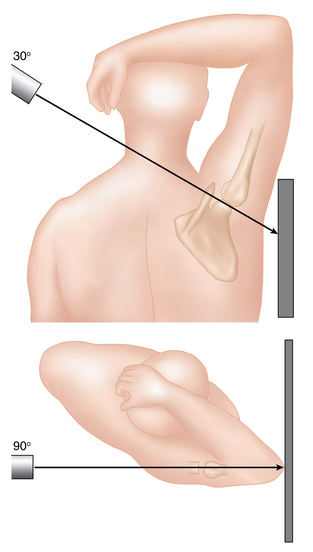
Radiographic findings
Description of techniques
Surgical exposure
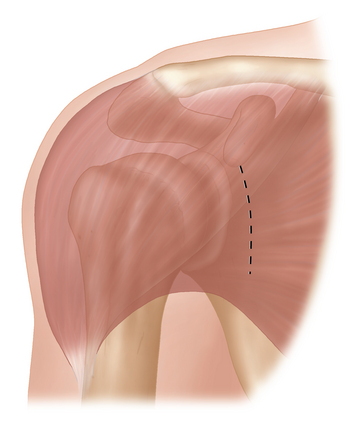
A deltopectoral approach is used. The skin incision is vertical from the tip of the coracoid, extending 4 to 5 cm towards the axillary fold (Fig. 16-4). In cases in which improved cosmesis is desirable (i.e., young females) an incision as small as 3 cm can be used. The cephalic vein is taken laterally, and its large medial branch is ligated. A self-retaining retractor is used to maintain exposure between the deltoid and pectoralis major. The arm is placed in abduction and external rotation and a Hohmann retractor is placed over the top of the coracoid process.
Procedure
Step 1—coracoid osteotomy and preparation
Related posts:
 Recurrent instability due to capsular deficiency
Open treatment of anterior instability—surgical technique
Arthroscopic treatment of multidirectional instability—surgical technique
Recognition and management of combined instability and rotator cuff tears
Arthroscopic treatment of posterior instability—surgical technique
Imaging findings in posterior instability
Recurrent instability due to capsular deficiency
Open treatment of anterior instability—surgical technique
Arthroscopic treatment of multidirectional instability—surgical technique
Recognition and management of combined instability and rotator cuff tears
Arthroscopic treatment of posterior instability—surgical technique
Imaging findings in posterior instability
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


