, Paola Catalano1, Andrea Piccioli2, 3, Maria Silvia Spinelli4, 3 and Federica Zavaroni1
(1)
Anthropological Service, Soprintendenza Speciale per il Colosseo, il Museo Nazionale Romano e l’Area Archeologica di Roma, Rome, Italy
(2)
Oncologic Center “Palazzo Baleani” Azienda Policlinico “Umberto I”, Rome, Italy
(3)
The Italian Society of Orthopaedics and Traumatology (SIOT), Rome, Italy
(4)
Department of Orthopaedic and Traumatology, Catholic University Hospital, Rome, Italy
5.1 Introduction
Carla Caldarini5 , Paola Catalano5, Andrea Piccioli6, 7, Maria Silvia Spinelli8, 7 and Federica Zavaroni5
(5)
Anthropological Service, Soprintendenza Speciale per il Colosseo, il Museo Nazionale Romano e l’Area Archeologica di Roma, Rome, Italy
(6)
Oncologic Center “Palazzo Baleani” Azienda Policlinico “Umberto I”, Rome, Italy
(7)
The Italian Society of Orthopaedics and Traumatology (SIOT), Rome, Italy
(8)
Department of Orthopaedic and Traumatology, Catholic University Hospital, Rome, Italy
5.1.1 Historical Developments in Musculoskeletal Oncology: From Amputation to Limb Conservation
Current musculoskeletal surgery is based on studies from the beginning of 1900 and the incorporation of metal implants (into the human body) that are subjected to corrosion when in contact with bodily fluids, thus reacting as a foreign body. In 1932, the development of Vitallium, an alloy of chromium and cobalt, first used in dental implants, opened the way to the employment of chromium-cobalt alloy syntheses in orthopaedics [1, 2]. The use of Vitallium in musculoskeletal oncology dates back to 1943, when a proximal femur endoprosthesis was implanted [3] after resection due to giant-cell tumour, with signs of evident integration at autopsy and radiography 1 year later. This led to the creation of new implants using different materials, such as steel, polyethylene, and others, both in the treatment of resections and in long bone defects [4]. However, amputation represented the main treatment option in patients affected by musculoskeletal neoplasias. The actual spread of prosthetic implants (still personalized) came thanks to the progress in radiology, pathology, chemotherapy, and radiotherapy, which allowed a better staging and assessment of the tumour’s size, and a higher survival rate in patients with musculoskeletal tumours. In particular, adjuvant chemotherapy was used in the 1970s as additional therapy in surgery to reduce local relapses and treat any residual cancer cells with encouraging results in terms of survival rates [5, 6]. Moreover, thanks to the progress in integrated treatments, the number of candidate patients for prosthetic treatments and conserving surgery increased, and this was a major improvement compared to amputation. This context led to a growing effort towards the improvement of prosthetic systems and the birth of standard modular endoprostheses [7], first for the proximal and distal femur, for the proximal tibia, and for the proximal humerus [8–11]. With the development of more and more sophisticated prostheses for the reconstruction of bone defects after resection, a major contribution to the systematization of the treatment approach of musculoskeletal tumours was given by Prof. Campanacci and Prof. Enneking [12] who set the ground rules for staging, reconstruction, and integrated treatment of musculoskeletal tumours. In conclusion, musculoskeletal oncologic surgery was actually born about half a century ago and has evolved since then. In particular, the new material technologies, the development of adjuvant therapies, and the systematization of the approach have led us to the present context, where we are able to save most patients’ limbs, thus increasing their quality of life, and the prognosis in case of musculoskeletal tumours [13].
History of Medicine: Tumours Care
Valentina Gazzaniga and Silvia Marinozzi
In Ancient medical texts, the term tumour is not always used as our term neoplasm, generally referring only to swellings, skin lesions, inflammatory status. palaeontology and palaeopathology studies have highlighted how cancer seems to be characteristic of terrestrial vertebrates, even though some neoplastic forms have also been found on fossils of water animals and reptiles, and have demonstrated the philogenetic relationships between focal hyperostosis in fish and osteoma in man. Neoplastic lesions have been found on animal fossils from the palaeolithic and mesozoic periods, but the finds dating back to the jurassic and the cretaceus periods, that is the time of the development of terrestrian animals and reptiles, certainly show a higher rate of neoplasms than the water species. The difficulty in reaching a diagnostic certainty on biological and human ancient material is clearly shown in an article by Luigi Capasso (Antiquity of Cancer. International Journal of Cancer. 113(1):1–12). The diagnoses of tumours on palaeolithical human skeletal finds are still unreliable, and the small number of finds does not allow a realistic hypothesis of the incidence of these diseases in prehistoric and ancient populations. In Hippocrates’s works, the terms karkinos and karkinoma recall, metaphorically and literally, a “wear and tear” of the areas attributable to animals’ bites and scratches, and they are used by the hippocratic doctor to explain the appearance of ulcers and internal and far-between new formations, as a consequence of a pathological process recalling a live entity moving within the body, and eating and corroding its organs and limbs. The semantic and conceptual continuity of some forms of neoplasms is found in the use of the Latin terms cancer and carcinoma to identify some pathological conditions. Celsus describes carcinoma as an abnormal hard new growth, forming mainly in the high areas of the body, in particular on the face (skin, nostrils, ears, and lips) and on women’s breasts; first it develops as a swelling, and later involves the blood vessels thus producing red, rugged ulcers. It is difficult to remove after the very first growth phase, and almost always incurable, because the disease relapses even when removed. Similarly, Celsus attributes the ability to relapse also to “goitre”, a disease characterized by hard and resilient nodules growing underneath a corrupt and purulent part of the body, particularly in the armpit, groin, and breast areas, that can be interpreted as a scirrhous swelling of the glands (De medicina V, XXVIII, 7). In Galen (129–210), the choice of terms is based on what the lesions and pathological new growths look like, and on the assonance of signs and symptoms with a specific animal: “…we often see a tumour in the breasts that totally looks like a crab”, because it has legs on both sides, as the veins that branch out from the tumour mass (Ad Glauconem de Methodo Medendi. II, K. XI, 140–141). Sometimes, due to black bile build-up, some blackish, non-purulent swellings grow and cause some malignant ulcers corroding the flesh (De atra bile, K. V, 122). The diseases called after an animal’s name due to the morphologic similarity of the physical alterations to a given animal species often have a similar aetiologic interpretation: in Galen, cancer and elephantiasis both derive from a black bile build-up, which causes preternatural growths (De alimento K XV, 331). The same is found in the choice of therapies, which involves, based on the principle of similia similibus curantur, the pharmaceutical use of crab (Plinius N.H.XXXII, 46, 134). Celsus provides information of lesions likely associated to bone tumours when he refers to forms where the bone grows big, then becomes black, and decays, developing ulcers or fistulas that can progress and erode it; the intervention involves the removal of the rotten flesh so as to uncover the bone and cauterize it, and in case of larger lesions the bone has to be scraped to allow some blood to come out. If there are caries, the bone has to be scraped until the harder part of it is reached, while in the presence of black matter the tissue is removed until the bone is completely white. For this operation, Celsus also uses the drill, which the hippocratic tradition had indicated for the removal of bone segments and splinters which could be harmful in fractures of the skull. The modiolus is composed of two wooden sticks, a thread, and a series of removable metallic tips; one stick is bow-shaped, with handles at its extremities, and pierced in the middle so as to allow the second stick to slide through it; this one ends in a metal cylinder with a saw-toothed lower edge to screw the trephines on; the grips of the bow are pierced to allow the thread to turn around the upper part of the toothed crowns of the drill (and to pull it alternately in one or the other direction to turn the trephines and pierce the area to be removed). This tool is used in case of small lesions, because it acts with one only perforation able to insert the catheters and dry the bone, so as to remove the corrupt areas, then scrape and remove the rotten ones. In the presence of larger and deeper lesions, a drill is used, with a tip that widens and lifts a bigger amount of bone; some holes are pierced around the corrupt area, thus allowing the removal of the whole diseased region with a chisel. Non-oily medications are then placed on the area, such as raw wool soaked in oil and vinegar (De medicina VIII, 2, 1).
5.2 Benign Bone Tumours
5.2.1 Osteochondroma of the Proximal Humerus
5.2.1.1 Morphological and Palaeopathological Description of the Subject
The skeleton, pertaining to a mature male subject, is whole and in a good state of preservation. The cranial indices denote a roundish shape (brachycranic), with averagely diverging frontal crests; the orbits are large (hypsiconchic), while the nasal index has intermediate values (mesorrhine). The right portion of the frontal bone shows a sub-circular depression, presumably due to a trauma (Fig. 5.1). Two Wormian sutural ossicles can be observed bilaterally along the lambdoid suture. The oral pathologies consist of moderate calculus build-ups on all the teeth and resorption of the alveolar margins, both on the maxillary and mandibular bones. Moreover, some cavities can be observed only on the left emi-maxillary: a destructive one on the second molar, a mild one at the mesial neck of the first premolar, and a superficial one mesially on the third molar. The right superior second incisor and right inferior canine present rotated if compared with proper alignment. The section indices of the limbs suggest a robust subject with well-developed muscular insertions. The shoulders seem particularly under stress, with the presence of enthesopathies at the insertion of the costo-clavicular and conoid ligaments of the right clavicle and at the insertion of the pectoralis major muscle of the right humerus. The femurs are platymeric, and the attachment tubercle of the adductors, on the medial condyle of the right femur is hypertrophic and defined by bone spicules. The third trochanter can also be detected on the right femur, and is considered as a variant of the post-cranial skeleton [14] by some authors, while others consider it as an occupational marker, because it is a part of the insertion of the gluteus major muscle [15]. The lateral epicondyle of the right tibia shows the outcomes of a likely depression fracture, with remodelling of the antero-medial margin and new bone apposition (Fig. 5.2). A concave depression of the supero-lateral margin of the right patella may have resulted from a prolonged contraction of the quadriceps (vastus notch). A severe and localized periostitis can be observed on the proximal third of the right fibula diaphysis. Only the joint of the left elbow shows some arthritic signs: the trochlea articular margins are raised and irregular and the coronoid fossa is enlarged, with well-defined margins; a small area of subchondral necrosis can be detected on the lateral epicondyle (osteochondritis dissecans) [16]. In addition, the surfaces of the olecranon and of the coronoid process are expanded, with new spicular bone formations. The vertebral column is affected by mild degenerative, erosive, and productive phenomena, and four thoracic vertebrae, on the eight that can be observed, show Schmörl’s hernias. Bilaterally the ischiatic tuberosity, at the origin point of the semitendinous muscle, is extended and eroded, the potential manifestation of a chronic inflammation.


Fig. 5.1
Depression on the frontal bone
Fig. 5.2
Fracture of the lateral epicondyle of the right tibia
5.2.1.2 Description of the Lesion
Osteochondroma (also called exostosis or osteocartilaginous exostosis) is the most common benign lesion affecting the bone and accounts for 10–15 % of all bone lesions, both in women and in men [17]. The location is typically metaphyseal or metadiaphyseal. In this case, the metadiaphyseal location, the large implant base, and the continuity of the medullary from the host bone into the exostosis with no periosteal reaction is highly suggestive of sessile osteochondroma of the proximal left humerus (Fig. 5.3). The macroscopic examination shows the top of the extostosis as a spongious marrow, resulting from the loss of the cartilaginous cap. The absence of intramedullary and periosteal reactions (Fig. 5.4) of the contiguous bone rules out malignancies. In this type of lesion, the area more prone to a malignant transformation is the cartilage cap (chondrosarcoma) with a percentage <1 % in single cases and from 3 to 5 % in cases of multiple exostoses [17]. Symptoms depend on the site of the lesion and on the adjacent structures, because the clinical picture depends on the compression “ab extrinseco” of the exostosis.

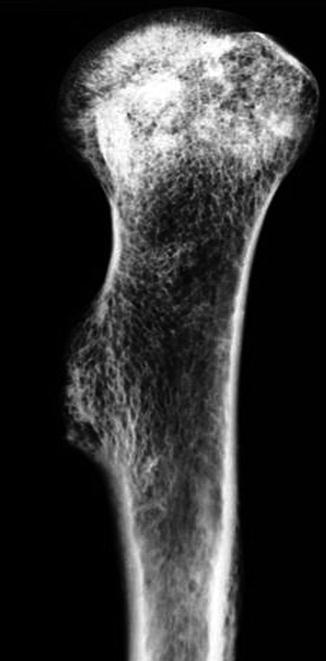
Fig. 5.3
Left humerus osteochondroma
Fig. 5.4
X-rays antero-posterior view of the proximal humerus. Exostotic lesion with no osteostructural alterations
5.2.2 Osteochondroma of the Proximal Tibia
5.2.2.1 Morphological and Palaeopathological Description of the Subject
The skeleton belongs to a young subject; even though the state of preservation is good, the right humerus is missing completely, and only a few fragments of the skull’s right parietal and occipital bone are left. The examination of the mandibular dento-alveolar complex shows the presence of a decay at the mesial position of the dentine, of the left second molar and one on the occlusal surface of the left third molar; the right third molar is typically peg-shaped (Fig. 5.5): it is a small-size tooth, without the normal crown morphology (diameter b-l: 3.9 mm) [18].

Fig. 5.5
Peg-shaped right third molar
The skeleton is in the growth phase and shows some metaphyseal lines still partially active when the subject died. The right radius, ulna (the humerus is missing) and lower limb are about 8 mm longer than their contra-laterals. The ligament and tendon insertions are generally weak: only two enthesopathic alterations can be detected at the insertions of the brachii muscle of the left ulna and iliopsoas of the right femur. The fifth lumbar vertebra shows an early sacralization with osteophytic reaction and remodelling of the articular facets. The anteversion of the right femoral neck (Fig. 5.6) is noteworthy, that is the angular difference between the axis of the neck of the femur and the transcondylar axis of the knee. The anteversion of the femoral neck, which is an important feature for hip stability and normal ambulation, is a multifactorial outcome of heredity, fetal development, intrauterine position, and mechanical forces [19]. The anteversion of the femoral neck draws an angle of about 55°. The right clavicle exhibits a well-healed fracture in the diaphyseal portion, with overlapping of the two bone stumps and robustness of the lateral extremity. Only a few vertebral fragments of the cervical column and of the superior tract of the dorsal one are left. On the contrary, the tract between T9 and L5 is well preserved; five thoracic vertebrae show osteophytic interapophyseal degenerations and two Schmörl’s hernias. Because of the subject’s young age, the alterations on the axial skeleton may be due to biomechanical stress.

Fig. 5.6
The anteversion of the right femoral neck
5.2.2.2 Description of the Lesion
A pedunculated osteochondroma can be observed on the medial profile of the left tibia’s proximal part (Fig. 5.7). When exostoses are so small, a differential diagnosis with the insertional calcifications of the tendons is needed. However, the present case shows a “centrifugal” attitude of the knee joint that is characteristic of osteochondroma. Even in this case, X-ray examination (Fig. 5.8) shows the lack of periosteal and endosteal reaction of the host bone and the continuity of the exostosis’ cortical and medullary with that of the tibia. In some cases, such small lesions in areas with a reduced representation of the adjacent soft tissue make the exostoses a potential site for its own fractures, and this would explain the remodelling of the end edge of this subject’s exostosis. The clinical picture shows a condition that ranges from silent to localized pain, mainly in case of fracture of the exostosis, with local swelling and jerk sensation during exercise due to conflict with the adjacent soft tissues.

Fig. 5.7




Osteochondroma of the left tibia
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
