Fig. 10.1
Schatzker classification (Hölzl, Verheyden (2008) Diagnostik und Klassifikation Der Ellenbogenverletzungen, Isolierte Olecranonfrakturen. Der Unfallchirurg 111:727–734)
Another classification system according to the AO (Arbeitsgemeinschaft für Osteosynthesefragen) takes the proximal radius and proximal ulna fractures as one group of lesions into account. These fractures are classified as belonging to region “21”, “2” standing for the second long bone region (lower arm), “1” standing for the proximal part of it. Type A fractures are extraarticular, type B are intraarticular fractures concerning the articular surface of either the radius or the ulna, and type C are intra-articular fractures involving both bones.
A third classification system is the Mayo classification according to Morrey (Fig. 10.2). Olecranon fractures are divided into three types, with subtypes taking the degree of comminution into account. Mayo type I fractures are undisplaced fractures and may be subdivided into type A, noncomminuted fractures, and type B, comminuted fractures. Type II fractures are stable displaced fractures, and may be noncomminuted (type IIA) or comminuted (Type IIB). Type III are fracture dislocations.
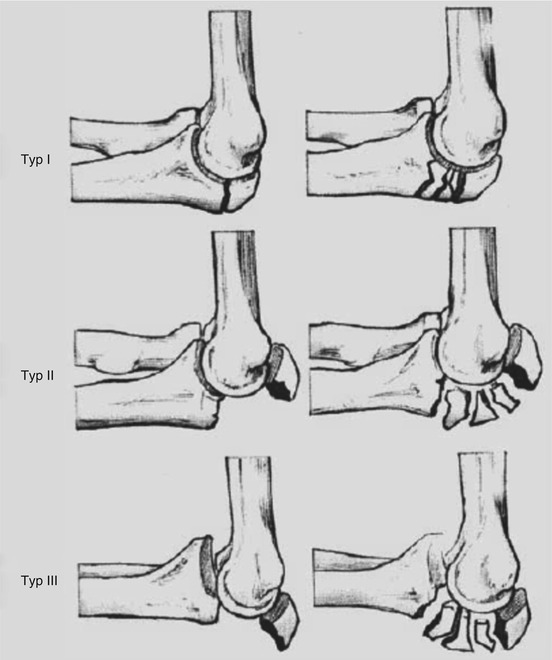
Fig. 10.2
Mayo classification
10.5 Treatment
10.5.1 Conservative Treatment
Nondisplaced olecranon fractures may potentially be managed by maintaining the elbow in a semi-flexed position (to 90° of flexion) with a cast for 7–10 days. Follow-up radiographs at 1, 2, and 4 weeks after trauma are recommended to assess for displacement. After 1 week of immobilization, protected range of motion should be performed. Restrictions on active resisted elbow extension and weight bearing should be maintained for 6–8 weeks.
10.5.2 Operative Treatment
Displaced fractures require surgical intervention. Several different methods of internal fixation have been described. The fracture pattern plays a role in determining the fixation that is selected. Tension band wiring, intramedullary screw fixation, plate osteosynthesis, and fragment excision have been described. The aim of internal fixation is anatomic and permanent reduction of the articular surface, in order to mobilize the elbow as soon as possible and to prevent post-traumatic arthrosis.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


