CHAPTER 15 New Techniques in Elbow Arthroscopy
Elbow arthroscopy was pioneered during the early 1980s, but it came to increased prominence after Andrews and Carson’s 1985 paper,1 which described the anatomy of the elbow joint as seen through the arthroscope and demonstrated the feasibility of arthroscopic diagnosis and treatment of disorders of the elbow. Further works by Morrey,2 Lynch and colleagues,3 Poehling and coworkers,4 and O’Driscoll and Morrey5 secured the procedure as an accepted orthopedic practice. Initial concerns about the potential for neurologic injury remain the primary concern of elbow arthroscopists today, and thorough knowledge of the neurovascular anatomy of the elbow is essential for performing elbow arthroscopy safely.
THE STIFF ELBOW
 Intra-articular pathology, such as intra-articular fibrosis, causing elbow stiffness may be amenable to arthroscopic treatment, but the prognosis may be limited.
Intra-articular pathology, such as intra-articular fibrosis, causing elbow stiffness may be amenable to arthroscopic treatment, but the prognosis may be limited.

We prefer to position the patient in a lateral position with the arm flexed at the elbow 90 degrees over a fixed bolster (Fig. 15-1). A 30-degree, 4.0-mm arthroscope without side-venting cannulas is most often used, but a 2.7-mm arthroscope can make visualization of the lateral gutter easier, and a 70-degree scope may add perspective in tight joints.

Capsule distention is performed easily and safely through the lateral soft spot. The normal joint can accommodate about 30 mL of fluid at 70 degrees of flexion, but in patients with joint contracture, this amount is significantly decreased and averages only 6 mL at 85 degrees. The capsule is also about 15% less compliant in these cases, and it is often thickened.6 Although capsule distention can increase the safety of portal placement by increasing the distance from the articulation to related neurovascular structures, the distance from the capsule to these structures remains unchanged and does not protect the neurovasculature during capsulectomy or capsular release.
We think the safest method of making portals is to incise sharply through the epidermis and dermis and bluntly dissect through the depths of the subcutaneous fat layers. This minimizes damage to cutaneous nerves that are found in the very depth of the subcutaneous fat (Fig. 15-2).7

Three types of anterior capsular releases have been reported:
 A capsulotomy is performed superiorly from medial to lateral. It is performed proximally to minimize the chance of radial nerve injury, and it is usually performed with cautery or a hook knife.
A capsulotomy is performed superiorly from medial to lateral. It is performed proximally to minimize the chance of radial nerve injury, and it is usually performed with cautery or a hook knife. In a linear capsulectomy, a strip of the proximal capsule is excised with a basket forceps or a resector.8
In a linear capsulectomy, a strip of the proximal capsule is excised with a basket forceps or a resector.8 In a radical capsulectomy, the entire anterior capsule is excised. To perform this safely, the radial nerve requires exploration.9
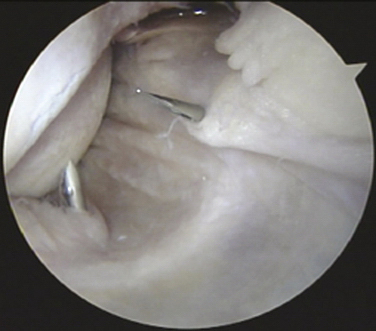
In a radical capsulectomy, the entire anterior capsule is excised. To perform this safely, the radial nerve requires exploration.9We prefer to perform a capsulectomy rather than a simple release to reduce the risk of recurrence. If the surgeon wishes to identify the radial nerve before excising the adjacent capsule, we recommend the use of two medial portals and a lateral retractor to protect nervous tissue (Fig. 15-3). Our preferred technique is to excise the medial one half of the capsule first. A mini-Hohmann retractor is then introduced through the medial portal. An arthroscope is placed in the medial superior portal with the retractor in the medial inferior portal. The capsule can then be teased off the brachialis muscle using blunt dissection. The blunt-ended retractor can be rotated to identify this natural interval. The radial nerve can be safely retracted anteriorly by advancing the retractor toward the lateral side. After this interval is developed, a second retractor is passed through the anterolateral portal and passed between the capsule and the first retractor, which can be removed. At this point, the capsulectomy can be safely completed. The capsulectomy should not proceed unless the nerve can be clearly visualized and protected with the Hohmann retractor.
PEARLS& PITFALLS
Postoperative Management and Rehabilitation
The range of motion achieved intraoperatively should be accurately recorded. The aim is to achieve this range as early as possible postoperatively. Good postoperative analgesia is essential, and the use of nerve blocks can be useful. Range-of-motion exercises should be active whenever possible. Continuous passive motion (CPM) or night splinting is advocated by some surgeons, but it is not used in our practice. Although CPM has been shown to mildly improve active flexion in open capsulectomy, mean active extension is unaffected, and it is often poorly tolerated.10






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


