CHAPTER 36 Complications of Wrist Arthroscopy
The use of arthroscopy has enabled direct visualization and diagnosis of intra-articular wrist pathology.1–3 It is widely used in the treatment of wrist injuries, such as triangular fibrocartilage complex tears, scapholunate and lunatotriquetral tears, and synovitis, and the excision of dorsal ganglia and débridement of arthritic lesions.4–10 Wrist arthroscopy has proved to be an excellent way to examine intra-articular pathology11–14 and to treat these pathologic conditions.15–27
PREVENTING COMPLICATIONS
Arthroscopy has justifiably been touted as a safe and effective method for examining the intra-articular components of the radiocarpal and midcarpal joints,28 and it is considered a relatively low-risk procedure.29–33 As with any surgical procedure, complications may be encountered, including tendon injury from inappropriately placed portals, skin slough from traction devices, nerve injury, complex regional pain syndrome,34–36 and rare conditions such as one case involving fistula formation after wrist arthroscopy.37 Associated with each portal are certain anatomic structures with which the surgeon must be familiar to prevent portal-specific complications from occurring.38 This chapter seeks to familiarize the wrist surgeon with these structures and techniques for preventing injury to them. Portal anatomy and the risks associated with each portal based on surrounding anatomic structures are addressed, along with the general risks associated with wrist arthroscopy. The Pearls and Pitfalls section describes common errors made when learning wrist arthroscopy and the techniques employed to avoid those errors.
RISKS AND COMPLICATIONS BY PORTAL SITE
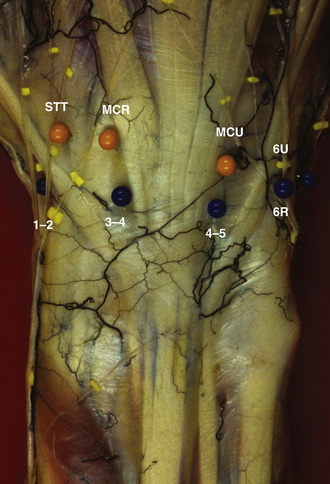
Wrist arthroscopy portals are based on the extensor compartments of the wrist. Figure 36-1 provides an overview of the dorsal arthroscopy portals with associated structures.
1-2 Portal
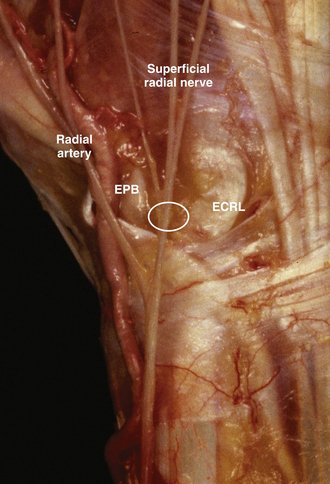
The superficial radial nerve is also at risk because its dorsal branch lies over the 1-2 portal. The most effective way to avoid laceration or traction of this nerve as the medial branch of the superficial radial nerve arborizes ulnarly is to make the portal skin incision with a no. 11 blade knife inserted only through the skin layer and then by traction on the skin itself, rather than using the blade, to enlarge the portal. Blunt dissection down to the capsule is recommended to ensure preservation of this dorsal branch as it crosses the portal site (Fig. 36-2).
3-4 Portal
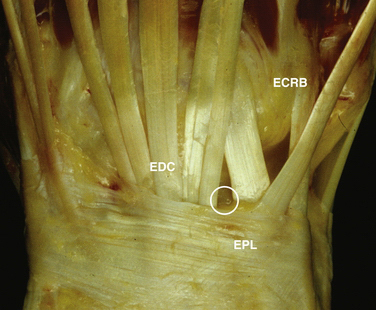
The 3-4 portal is most commonly the first portal established and is most easily established by inserting an 18-gauge needle into the wrist joint just distal to Lister’s tubercle and insufflating the joint with as much solution as the joint can hold comfortably. At that point, the needle and syringe may be removed from the joint while maintaining the capsular distention. The information from needle insertion and palpation of the capsular distention guides placement of the 3-4 portal directly over the radiocarpal joint between the ECRB/EPL and the EDC. The skin is pulled over the tip of the blade to establish the portal, lessening the risk of inadvertently lacerating one of the tendons. After the skin incision is made, the blunt trocar and cannula are inserted, moving the tip in a medial and lateral direction to have tactile feedback and ensuring guidance into the joint without injury to the articular cartilage (Fig. 36-3).
4-5 Portal
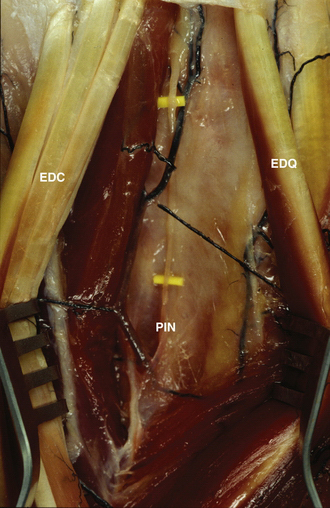
The structures most at risk during placement of the 4-5 portal (i.e., extensor digitorum communis–extensor digiti quinti [EDC-EDQ] portal) are the terminal branch of the posterior interosseous nerve and the dorsal sensory branch of the ulnar nerve. The posterior interosseous nerve passes deep to the fourth dorsal compartment on the ulnar side dorsal to the wrist to provide sensation to the wrist joint. The risk of damage to this nerve during placement of the 4-5 portal is lessened by placement of the portal in a slightly ulnar position with relation to the EDC tendon. The portal should be placed just radial to the EDQ tendon. From a practical point of view, the loss of the function of this nerve causes no functional deficit, and some think that it diminishes pain in the wrist joint.
The transverse branch of the ulnar dorsal sensory nerve is also at risk during placement of this portal. The transverse branch of this nerve passes distal to the portal, and risk of injury may be lessened by placing the portal as proximal as possible in the wrist joint. We recommend longitudinal portal placement followed by blunt insertion into the joint to ensure preservation of the nerve (Fig. 36-4).