12
Neurovascular Healing and Thromboembolic Disease
2. Discuss the vascular supply to nerve tissue.
3. Understand the mechanical behavior of nerve tissue.
4. Identify the causes and classification of nerve injury.
5. Discuss intrinsic nerve healing.
6. Describe methods of surgical repair of nerve injury.
7. Identify structure and composition of vascular tissue.
8. Discuss the vascular response to injury.
9. Explain the various signs and symptoms of vascular injury.
10. Discuss the pathophysiology of thromboembolic disease.
11. Recognize risk factors of deep vein thrombosis and pulmonary emboli.
PERIPHERAL NERVE INJURY
Vascular Supply
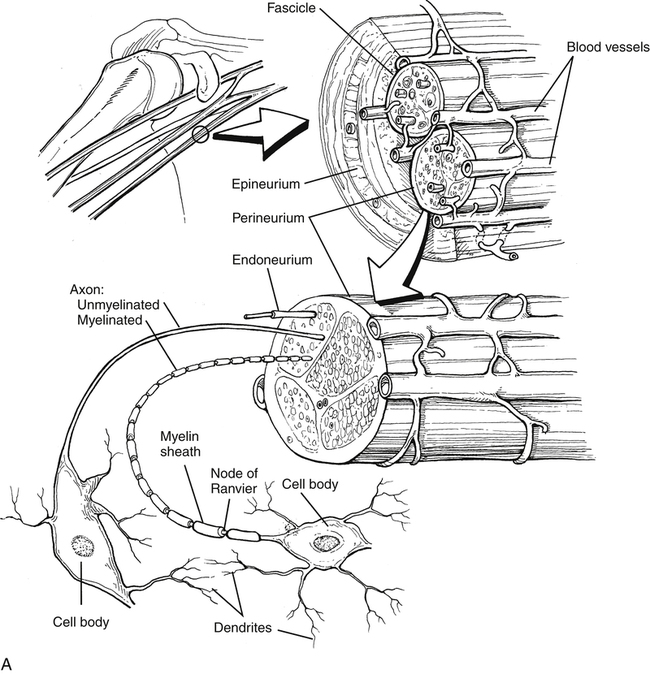
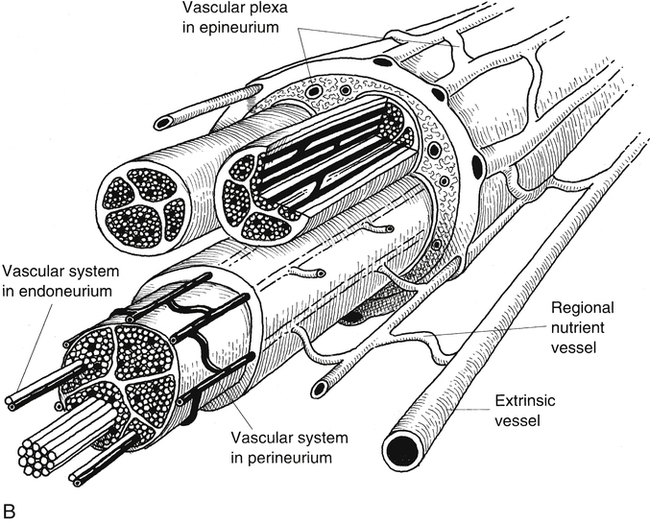
Peripheral nerve has a complex and extensive blood supply. The PNS requires an ongoing nutritive energy supply for maintenance of nerve conduction. Longitudinal extrinsic vessels connect with regional feeding vessels that form a vascular plexus within the epineurium, perineurium, and endoneurium connective tissue network within the nerve fiber (Fig. 12-1).2,9
The initial response to nerve trauma is a predictable response like that seen after vascular tissue trauma. After a brief period of vasoconstriction, vascular permeability increases because of the release of potent chemical mediators such as serotonin and histamine.11 The result is edema within the nerve fiber’s connective tissue barriers (epineurium, perineurium, endoneurium). The dramatic change in fluid pressure and tissue edema adversely affects oxygen transport, nutrition, ion content of nerve cells, and conductivity of the traumatized nerve fiber.9
Mechanical Behavior of Nerve Tissue
Nerve tissue is highly deformable, expressing relatively similar viscoelastic mechanical behavior as other soft tissue. Essentially, two load deformation terms are used to quantify a tissue’s ability to adapt structurally and mechanically to time-dependent forces. Creep is a term used to describe the tissue’s ability to change or “creep” to a new length in response to a constant, applied load. The greater the load (stress), the faster the tissue will deform or creep. Stress relaxation is similar to creep, in that it is a time-dependent phenomenon. It occurs when a material is elongated (strained) to a given dimension and then maintained at that length. In this situation, there is a reduction in the amount of stress required to maintain the fixed length. Peripheral nerve tissue responds with this viscoelastic behavior by showing ultimate load-to-failure values of 20% to 60%. Although peripheral nerve tissue may tear when the nerve is elongated to approximately 20% more than its resting length, ischemic changes, which profoundly affect nerve function, may occur when a nerve is stretched less than or equal to 15% of its resting length.1,12
Causes and Classification of Nerve Injuries
Trauma to peripheral nerve comes from mechanical, thermal, chemical, and vascular injury. Mechanical sources cause contusion, concussion, stretch, compression, laceration, and transection.8,9 Classification of nerve injury provides concise and anatomic descriptions. However, the clinical reliability of this system is debatable.1,6,9 Many injuries cannot be classified into a single grade. The three most common categories of nerve injury are neurapraxia, axonotmesis, and neurotmesis.6,8,9
Neurapraxia is the reduction in nerve conduction at the site of injury, usually due to compression. The lesion is local, the axon’s continuity is maintained, and all pathologic changes associated with neurapraxia generally are reversible if the cause is removed.6,8,9 Functional recovery occurs within weeks or months.9
In axonotmesis, the epineurium remains intact, while damage to the perineurium and endoneurium occurs to varying degrees. Because the epineurium is undamaged, functional recovery without surgery may occur. However, as greater amounts of perineurium and endoneurium become involved, surgery is required to achieve the most functional recovery.9
Neurotmesis is diagnosed when the entire nerve trunk is transected or ruptured. The total loss of nerve continuity requires surgical adaptation and coaptation. Prognosis depends on the nature of the injury, as well as local and general factors, such as patient age and timing of the repair.1,6
In a very broad sense, a pure motor nerve is a greater risk for injury than a pure sensory nerve. A gross prediction is that peripheral nerves usually fail to conduct impulses related to motion (first), proprioception, touch, temperature and pain (last). Recovery of these abilities occurs in the reverse order.1,8
Compression and Traction Neuropathy
Nerve compression injuries are acute or chronic in origin. In both cases, the physiologic consequence of compression or traction on peripheral nerve tissue is mechanical disruption of the nerve fiber and ischemia (Fig. 12-2).9 Anatomically, certain peripheral nerves are at risk for compression neuropathy because of the surrounding arrangement of soft tissue and bone, which limits the nerve’s three-dimensional motion. Specifically at risk in the lower extremity are the common peroneal nerve behind the fibular head and the lateral femoral cutaneous nerve within the inguinal ligament (meralgia paresthetica).1 In the upper extremity, nerves most susceptible to mechanical disruption are the radial nerve within the spiral groove of the humerus, and the median nerve within the soft tissue confines of the carpal tunnel arch. Spinal nerve roots are more susceptible to compression injury than peripheral nerves because spinal nerve roots have no epineurium.9
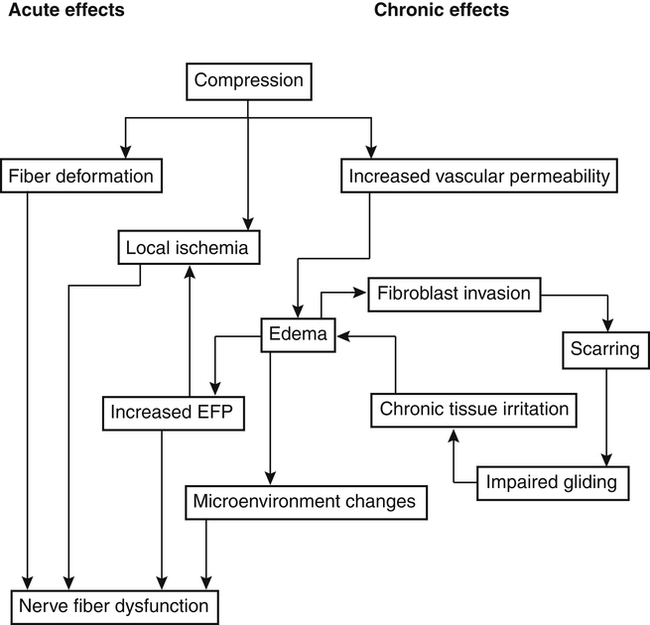
The biological responses of the PNS to acute and chronic compression include obstruction of intraneural blood vessels, tissue anoxia, local ischemia, nerve fiber deformation, increased vascular permeability, intraneural edema, and fibroblastic proliferation with resultant decreased nerve gliding.9
Traction or stretch neuropathy is classified as acute or chronic with the magnitude of injury classified as neurapraxia, axonotmesis, and neurotmesis as described. A practical and common description of acute traction neurapraxia is the “burner” or “stinger” experienced by athletes, in which the shoulder is depressed with concomitant contralateral head and neck flexion that creates a brachial plexus stretch.2
Occasionally with lengthy surgical procedures, prolonged wide surgical field exposure leads to inadvertent stretch of surrounding peripheral nerve tissue. Surgical procedures may also require prolonged tourniquet application, with cuff pressures occluding neural blood supply.8,9
Physical therapy (e.g., range of motion [ROM] exercise) after prolonged joint immobilization may cause traction neurapraxia due to premature and intensive stretch. During the protection phase of postoperative care or during prolonged immobilization, slow, controlled stretch, devoid of high velocity or force protects nerve from unwanted injury.8,12
Some patients may experiences signs and symptoms of peripheral nerve compression or entrapment at more than one level of the same nerve. The term double crush syndrome is used to describe these signs and symptoms. The most common example is carpal tunnel median nerve compression neuropathy and cervical nerve root injury. Another example is nerve entrapment neuropathy at the elbow along with cervicothoracic root lesion. To explain this syndrome, it is hypothesized that a compression lesion at one level of the nerve makes the same nerve more susceptible to injury at another site.1,9 It is suggested that compression reduces nerve conduction, blood supply, and the amount of plasma membrane proteins. These reductions adversely influence other segments, making them more sensitive to mechanical or compressive forces.9
Methods of Peripheral Nerve Repair
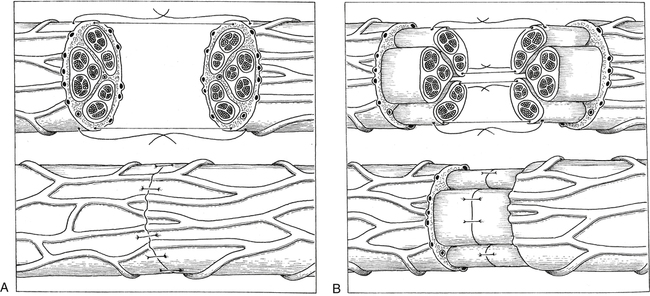
The term neurorrhaphy is synonymous with direct coaptation or surgical apposition of corresponding nerve stumps or fascicles.8,9 This specific intervention is reserved for neurotmesis with complete disruption of nerve continuity. The basic objectives for surgical repair (neurorrhaphy) are to maximize the number of axons that regenerate across the lesion and to reinnervate distal sites accurately, for example, that proximal motor axons reach distal motor axons (Fig. 12-3).1,8,9





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


