The toenail is a specialized keratinized appendage with a primary function of protection for the distal phalanx. It is capable of only a limited number of pathologic responses, many of which are reviewed in this chapter.
Unlike skin and hair, the nail does not shed or desquamate and is not cyclic. Nails are hard because of a relative lack of water content as compared with the stratum corneum (1). Water flux across the nail is ten times that across skin; however, the nail plate is unable to hold water because of its low (less than 5% by weight) lipid content (2). Moreover, the relatively high sulfur content in nails, predominantly in the form of cystine, appears to contribute to their hardness. Nails are 9.4% cystine by weight compared with 1% in callus (3).
Because the nail is hard and does not desquamate, many of the conditions involving the nails become more difficult to treat either with medication or by surgical means. A thorough knowledge of the properties of the nail and its surrounding anatomic structures increases the effectiveness of all treatment programs and enables the physician to provide better cosmetic results (4).
ANATOMY
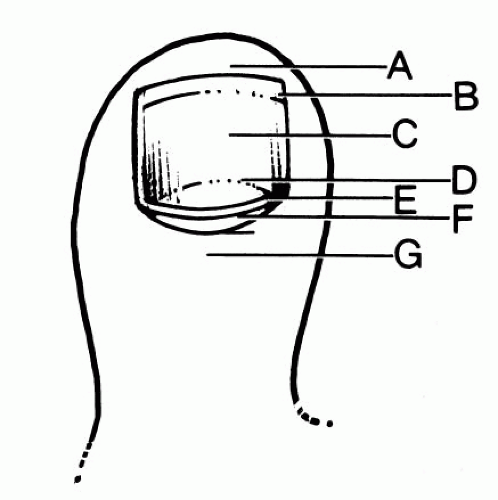
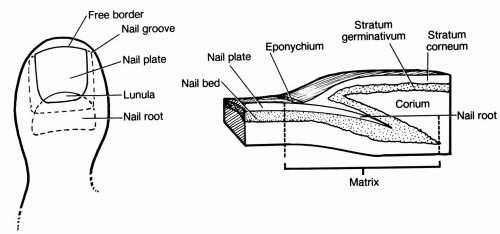
The nail consists of a nail plate and the supporting tissues surrounding it (Fig. 1). Nail growth appears to be continuous, with little change in the overall rate. Toenails extend distally approximately 0.03 to 0.05 mm a day. The thickness of the toenail is between 0.05 and 1.0 mm. The toenail is set on the dorsal surface of the distal end of the toes in grooves that are referred to as the lateral and proximal nail grooves (Fig. 2). The grooves are covered by corresponding folds, the lateral and proximal nail folds. The nail plate itself appears translucent in areas where it is not attached to the underlying nail bed. The areas that are attached to the underlying adherent and vascular nail bed appear pink as the result of the transmission of color from this area.
Many digits display a white semicircular lunula at the proximal end of the nail plate, which is the topographic marker of the nail matrix. The lunula represents the junction point between the nail matrix and the nail bed. The nail matrix, which synthesizes the nail plate substance, extends proximally under the nail fold about 5 to 10 mm in depth. The region underlying the free edge of the nail plate distal to the nail bed and proximal to the epidermis of the tip of the digit is the hyponychium. Overlapping the matrix of the nail is the proximal nail fold, the stratum corneum of which is prolonged distally as a thin, cuticular fold, the eponychium. Below the nail lies the germinative zone that, together with the subjacent corium, forms the nail bed (5).
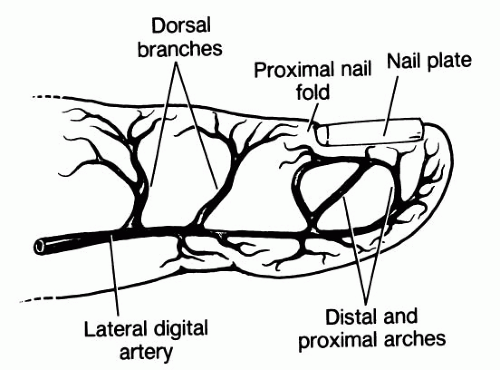
Circulation to the nail is supplied by two arterial arches derived from the two digital arteries. The digital arteries course laterally on the digits and give off multiple small dorsal branches into the pulp space of the distal phalanx. These dorsal branches, in turn, divide to form the distal and proximal arches (Fig. 3). An additional branch leaves the digital artery at the midportion of the middle phalanx and does not enter the pulp space but courses over the distal interphalangeal joint space. This serves the proximal matrix and provides the corollary circulation (6).
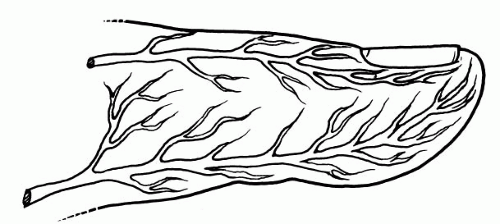
The hallux receives its innervation from four nerves: (a) a digital branch of the deep peroneal that supplies the lateral dorsal area, (b) the medial dorsal cutaneous nerve, (c) the lateral common digital nerve from the medial plantar nerve that supplies the lateral plantar area, and (d) the medial digital nerve from the medial plantar nerve that supplies the medial plantar area of the hallux (7) (Fig. 4).
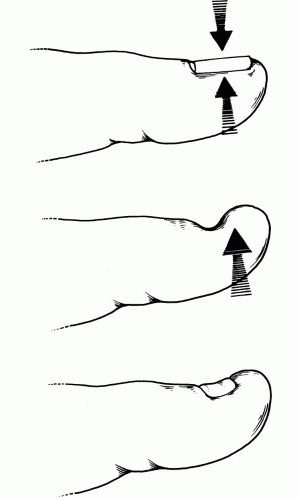
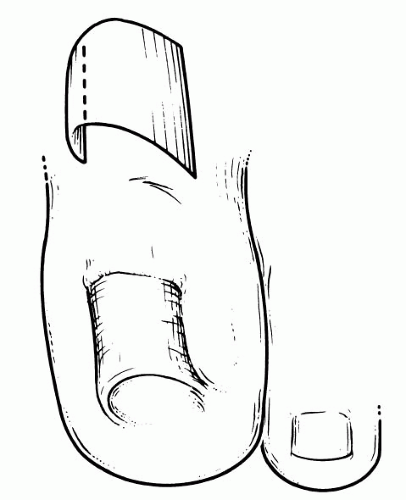
Because of the orientation of the matrix cells in a forward position and because of pressure exerted by the posterior nail fold, the nail grows forward and flat rather than upward. If a portion of the nail matrix is rearranged because of injury or surgery, or if it is grafted on the skin away from the nail fold, it will produce a nail that projects straight up from its surface (8). If the nail is completely removed, the upward pressure will force the distal nail bed to bend and elevate upward, causing a deformation of the distal nail bed. As the new nail begins to grow out, it approaches the end of the toe only to meet this soft tissue wall, which tends to bulge the soft tissues upward around the distal part of the new nail, and the result is the creation of an ingrown or clubbed nail (9) (Fig. 5).
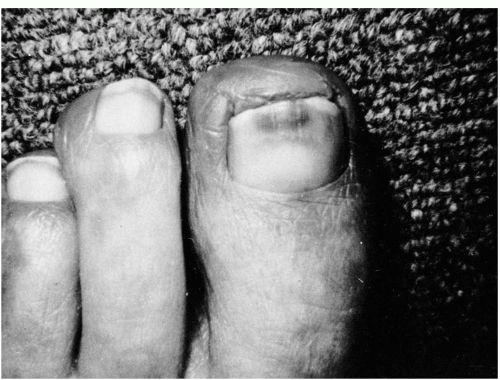
FIG. 1. Clinical appearance of the toenail. A, free nail edge; B, point of separation of the nail from the bed; C, nail plate; D, lunula; E, cuticle; F, eponychium; G, skin overlying the posterior nail fold.
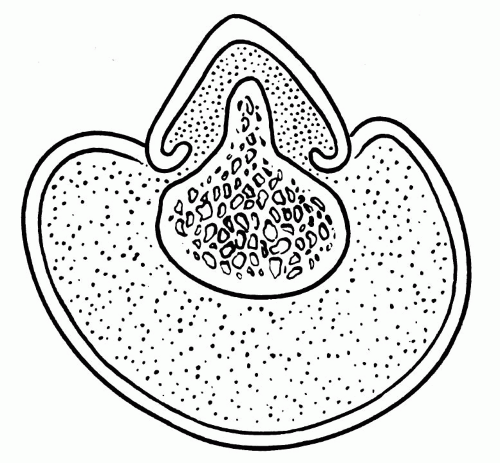
FIG. 2. Illustrative anatomy of the nail and diagram depicting the longitudinal cross section of the toenail.
FIG. 3. Blood supply to the hallux. (Redrawn from Scher RK. Nail surgery. In: Epstein E, Epstein E Jr, eds. Techniques in skin surgery. Philadelphia: Lea & Febiger, 1979:164-170, with permission.)
FIG. 4. Nerve supply to the hallux.
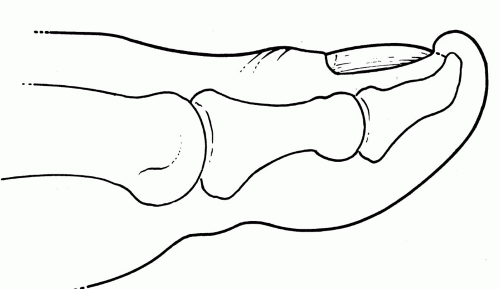
FIG. 5. Avulsion of the nail allows the distal nail bed to deform upward, causing hypertrophy of nail lip that may result in an embedded or clubbed nail as the new nail grows outward.
PATHOLOGIC CONSIDERATIONS
Changes in the toenails may be caused by disease, trauma, infection, biomechanical abnormalities, hereditary or genetic factors, and the effects of aging (10). The toenails offer little or no benefit, with the possible exception of protection to the dorsal toes; however, they represent a large number of complaints in patients with foot problems (11). Krausz in 1950 reported a nail survey of 4,600 podiatric patients with a total of 2,788 nail disorders that comprised 60% of the complaints (12). In a follow-up article in 1970 (13), he reported on 10,900 podiatric patients with a total of 6,754 nail problems (61%). The 4 most commonly reported problems were as follows: onychocryptosis, 1,765; onychauxis and onychogryposis, 1,493; onychophosis, 1,334; and onychomycosis, 551.
The nail itself is capable of only a few types of reaction patterns and is therefore predictable in its changes. Similar changes are shared by many different types of conditions and diseases. Skin and nail changes begin to occur as people age. The toenails thicken and show a slowing in growth, and they become more susceptible to disease (14). Other factors such as associated osseous disorders may also cause changes in nail growth and may create problems affecting toenails (15). Nail changes may occur during pregnancy (as early as the sixth week) and consist of transverse grooving, increased brittleness, softening, and distal onycholysis (16).
Pathologic Anatomy
Diseases and disorders of the nails may be classified into divisions according to (a) maladies peculiar to the nails themselves, (b) onychodystrophies, (c) ungual manifestations of dermatitis, (d) ungual manifestations of systemic disease, and (e) congenital conditions of the nails (17). The diseases themselves can be grouped into different classifications according to the most common types, which include (a) infection, (b) psoriasis, (c) contact dermatitis, (d) eczematous dermatitis, (e) hypovitaminosis, (f) tumor, (g) trauma, and (h) general disease (18).
Anonychia, the absence of nails, affects one or more nails and is usually congenital. It may be seen in nail-patella syndrome (hereditary onychoosteodysplasia) (19). Beau’s lines are transverse lines or grooves in the nail plate that may be associated with trauma or a disease process.
Brittleness of nails is common and may be caused by local or general factors, including nutritional disturbances, thyroid disorders, skin conditions, and aging. Constant immersion in water and exposure to certain chemicals may also cause brittleness of the toenails.
Clubbing of the nails may be seen in congenital heart disease and chronic pulmonary diseases and may also be associated with subacute bacterial endocarditis. Discoloration of nails may be caused by external or internal causes and may give clues to underlying systemic disease.
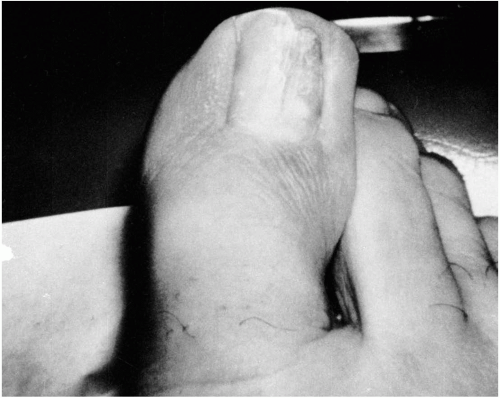
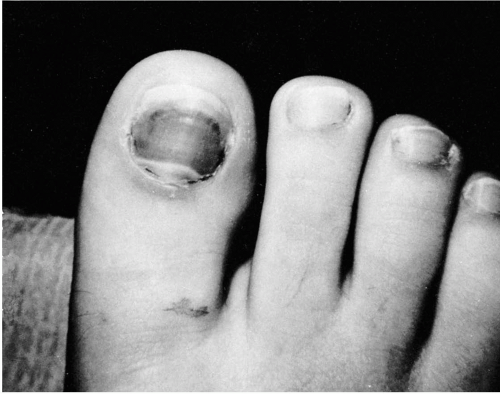
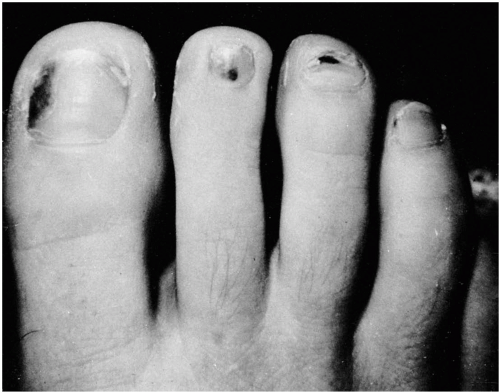
Dystrophic fissured nails are usually secondary to trauma but may also be a response to infection (Fig. 6). Hemorrhage may be visualized by subungual hematoma, which is almost always the result of trauma (Figs. 7 and 8). Splinter hemorrhages of the toenails may also be seen in subacute bacterial endocarditis and in certain types of dermatoses. Splinter hemorrhages have been reported in adult vitamin C deficiency syndrome (20).
Hypertrophy of the toenails may result from trauma or from developmental anomalies such as pachyonychia congenita (21). Other causes of nail hypertrophy are psoriasis, fungal infections, and Darier’s disease (22).
Koilonychia, spoon-shaped nails, are most commonly seen as a symptom of iron deficiency anemia. This may be a temporary disorder in young children and is also seen as a congenital anomaly.
Onychauxis is caused by hyperkeratosis of the nail bed itself. This may be secondary to local or systemic disease and may be the result of trauma. Fungal and bacterial infections also cause onychauxis.
FIG. 6. Dystrophic fissured toenail secondary to infection.
Onychoclavus, a type of onychophosis of the edge of the fifth toenail, appears as a complication of wearing shoes with narrow or pointed toes or from pressure of deformed nail margins (23). This may also occur as a result of bony spurring beneath the margin of the nail or from varus rotation of the toe that causes the patient to walk on the side of the digit.
Onychocryptosis, ingrowing of toenails, is seen more frequently than any other nail condition. Considerable time is spent dealing with the medical and surgical treatment of this particular problem.
Onycholysis, a separation of the nail from the nail bed, is one of the most common nail symptoms and is found as a result of trauma, psoriasis, fungal infections, and certain drug reactions (6).
FIG. 7. Subungual hematoma of the hallux caused by trauma.
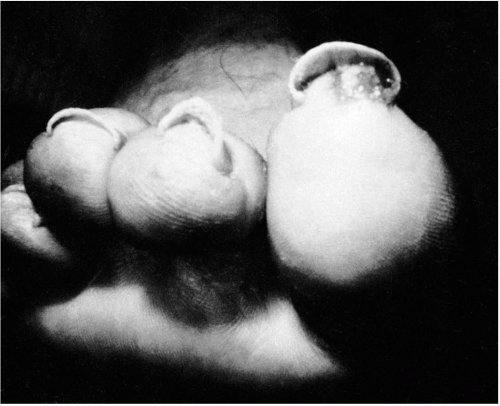
FIG. 8. Subungual hematomas typically seen in runners.
Pitting of the toenails is common in several types of dermatoses and is also seen in alopecia areata and fungal infections. Minor degrees of pitting are seen in healthy nails, and when no other skin complaints are found, it is considered to be a normal variant. Psoriasis is the condition in which pitting is seen most frequently (24); however, pitting can be found in patients with other conditions, including lichen nitidus (25).
Pterygium formation is a condition in which the cuticle appears to grow forward on the nail plate and the nail is split into two portions that gradually become smaller as the pterygium widens. This condition occurs as a result of impaired peripheral circulation and is seen in lichen planus (Fig. 9). Shedding of the nail may result from loosening of the base, as in onychomadesis, or separation from the nail bed (onycholysis) as a result of injury or disease.
FIG. 9. Pterygium of the hallux toenail in lichen planus.
FIG. 10. Vascular disease may cause painful toes that may be misdiagnosed as paronychia or subungual hematoma.
Splitting and striation appear longitudinally and may be the result of trauma and aging. These conditions are also seen in patients with rheumatoid arthritis and may be secondary to nutritional deficiencies (17). Thinning of the nail plate is seen secondary to decreased peripheral circulation, lichen planus, iron deficiency anemia, and epidermolysis bullosa.
Systemic Diseases
Nail changes accompanying systemic disease are relatively common complaints among patients. These changes are frequently good indicators of internal disease. Nail changes have been reported in patients who have iron deficiency anemia, Plummer-Vinson syndrome, idiopathic hemochromatosis, Raynaud’s disease, rheumatoid arthritis, and hepatolenticular degeneration (Wilson’s disease) (26). Painful toes may also be misdiagnosed as onychocryptosis or paronychia when the condition is actually secondary to the ischemic pain of vascular disease (27) (Fig. 10).
FIG. 11. Cross section of subungual exostosis showing how this osseous condition may cause deformation of the nail bed and incurvation of the nail plate. This condition is sometimes referred to as pincer nail.
FIG. 12. Pincer nail formation caused by subungual exostosis of the distal phalanx.
Trauma
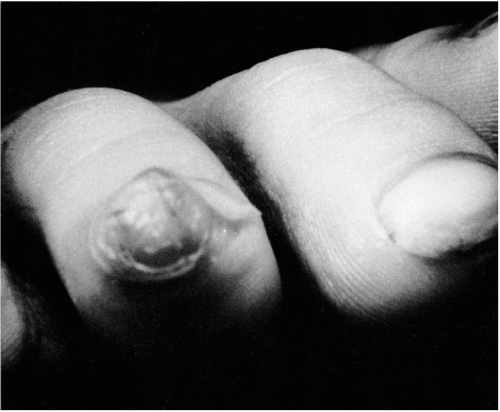
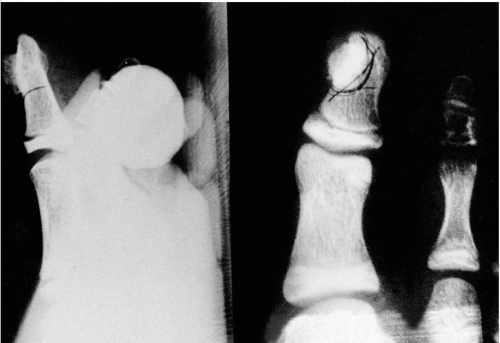
Obvious damage to the nail plate and nail bed causes pathologic changes of the nail. Damage to the nail matrix also causes defects ranging from grooves, pits, and ridges to frank abnormalities of the newly growing nail. Trauma may also result in the complete loss of the nail by avulsion, and if the nail root is damaged, a thicker, discolored nail may be the result. Injury to the underlying distal phalanx may also cause osseous change that results in deformity of the outgrowing nail. One of those lesions is the subungual exostosis that is believed to be secondary to trauma to the dorsal toe area (Fig. 11). The underlying subungual exostosis may result directly in onychocryptosis (28). In more pronounced cases the resultant condition is a pincer nail (Fig. 12). Some investigators believe that the osseous configuration of the distal phalanx is responsible for ingrown toenails, whether it be a dorsal spur of the tip of the phalanx or the upward sweep of the phalanx (29). Other reports indicate that the distal pulp of the digit, as well as the nail, may be changed because of the exostosis formation (30) (Fig. 13). Most subungual lesions occur over the distal phalanx of the hallux (31,32). In many of these cases, in which the exostosis is a result of trauma to the distal phalanx, the moderately growing lesion becomes painful as it enlarges, and surgical intervention is warranted (33) (Fig. 14).
FIG. 13. Lateral view showing how distal exostosis may change the configuration of the distal pulp of the digit.
FIG. 14. Traumatic exostosis of the distal phalanx that may become painful as it enlarges.
Also considered to be of traumatic origin are osteochondroma and enchondroma. Much confusion exists in the literature between osteochondroma and subungual exostosis. Most authors agree that osteochondroma can be differentiated from exostosis because osteochondroma has a cartilage-capped external surface. Because growth begins at or before puberty and the condition frequently is found in patients between 10 and 25 years of age, osteochondroma sometimes is listed as congenital (34) (Fig. 15). Exostosis differs from osteochondroma in that it has a female-to-male ratio of 2:1, whereas osteochondroma has a male predilection. The cartilaginous cap in the exostosis is made up of fibrocartilage rather than the hyaline cartilage of osteochondromas, and finally exostoses occur away from the epiphyseal line (35) (Table 1).
FIG. 15. Subungual hallux osteochondroma in a 13-year-old boy.
Paronychia or nail plate deformity and discoloration may occur with a solitary osteochondroma. However, this condition is rare in the distal phalanges as compared with exostoses and osteoma (36).
Infections
The two main types of infections involving toenails are fungal and bacterial. Onychomycosis, infection of the toenail by fungi, is divided into four clinical types: (a) distal subungual onychomycosis, (b) proximal subungual onychomycosis, (c) superficial white onychomycosis, and (d) candidal onychomycosis (37) (Table 2).
A distal subungual onychomycosis is the most common variety of fungal infection of the nail. The initial infection is in the area of the stratum corneum of the nail bed. The discoloration begins at the edge of the nail and spreads proximally. Onycholysis begins with thickening and irregularities of the nail plate as it separates from the nail bed. The subungual debris begins to accumulate and secondary bacterial infection may ensue. Trichophyton rubrum is the most common cause of this condition.
Proximal subungual onychomycosis begins in the stratum corneum of the proximal nail fold. It usually begins as a small, white area located proximally on the nail plate and subsequently enlarges laterally and spreads distally. Again, T. rubrum is the most common cause. This is also the rarest clinical form of nail fungus (26).
TABLE 1.Differential characteristics of exostosis, osteochondroma, and enchondroma
Tumor
Age (yr)
Sex ratio
History of trauma
Rate growth
X-ray
Exostosis
20-40
Female/male 2:1
Occasionally
Moderate
Trabeculated osseous growth with expanded distal portion covered with radiolucent fibrocartilage
Osteochondroma
10-25
Male/female 2:1
Often
Slow
Well-defined sessile bone growth with hyaline cartilage cap
Enchondroma
20-40
Male = female
Often
Rapid
Loculated bone cyst showing radiolucent defect, bone expansion, and flecks of calcification
From Norton LA. Nail disorders. J Am Acad Dermatol 1980;2:457, with permission.
Superficial white onychomycosis begins by directly invading the nail plate itself rather than extending onto the nail plate from the adjacent stratum corneum. This form of fungal infection does not occur in the fingernails but is a relatively common infection of the toenails. It creates a soft, white island on the surface of the nail that may spread to form large patches and encompass the entire surface of the nail. T. mentagrophytes is the most common cause of white superficial onychomycosis (37).
Candidal onychomycosis usually occurs in patients with mucocutaneous candidiasis. The infection, caused by Candida albicans, begins at the distal portion of the nail, spreads proximally the entire length of the nail, and can cause serious disfiguration. C. parapsilosis is rarely found in the fingernails; however, this organism is isolated frequently from toenails (26).
Bacterial infections usually involve the tissue surrounding the toenail rather than infecting the toenail itself. Paronychia is one of the more common nail complaints seen by the clinician treating the foot and ankle (Figs. 16, 17, 18, 19 and 20). Various organisms such as Staphylococcus, Streptococcus, Escherichia coli, and Pseudomonas have all been isolated from paronychial infections. Pseudomonas, one of the few bacteria capable of infecting the nail plate, produces pyocyanin, a blue-green discoloration of the nail (26). Some authors believe that onychocryptosis is actually secondary to infection rather than a problem of the nail itself (38). Others believe that paronychias and onychias are actually classified incorrectly and are really subungual granuloma pyogenicum (39).
TABLE 2.Organisms in onychomycosis
Toenails
1.
Distal subungual onychomycosis:
Dermatophytes: Trichophylon rubrum, T. mentagrophytes, Epidermophyton floccosum
Yeasts and molds: Candida parapsilosis, Scopulariopsis brevicaulis, Aspergillus, Cephalosporium, Fusarium
2.
Proximal subungual onychomycosis:
Trichophyton rubrum, T. megninii, T. schoenleini, T. tonsurans
Modified from Norton LA. Nail disorders. J Am Acad Dermatol 1980;2:451-467, with permission.
FIG. 16. Stage I (mild) paronychia.
FIG. 17. Stage II (moderate) paronychia.
FIG. 18. Stage III (severe) paronychia.
FIG. 19. Acute streptococcal paronychia with characteristic erythema surrounding an infected nail border.
FIG. 20.Pseudomonas paronychia with underlying blue-green nail plate discoloration.
TABLE 3.Benign and malignant tumors involving the nails
Benign tumors
Warts (periungual and subungual)
Fibroma (e.g., tuberous sclerosis)
Acquired digital fibrokeratoma
Neurofibroma
Myxoid cyst
Pyogenic granuloma (periungual and subungual)
Glomus tumor
Pigmented nevus
Keratoacanthoma
Bone cyst
Subungual exostosis
Osteochondroma
Enchondroma
Solitary bone cyst (e.g., aneurysmal bone cyst)
Malignant tumors
Squamous cell carcinoma (most common)
Malignant melanoma
Basal cell carcinoma
Metastatic carcinoma (e.g., club nails)
Bowen’s disease
Modified from Gunnoe RE. Diseases of the nails. Postgrad Med 1983;74:357-362, with permission.
Benign and Malignant Tumors
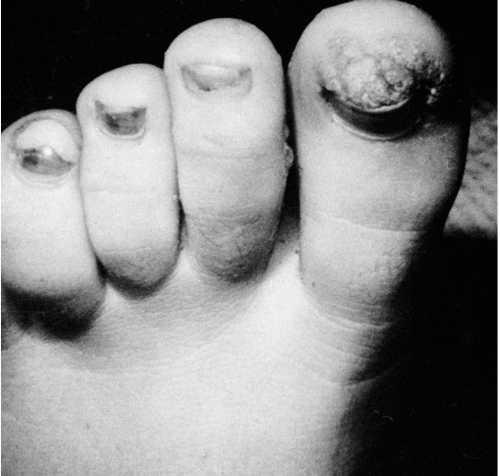
Many different benign and malignant tumors affect the tissue surrounding the nails and involve the nails themselves (Table 3). The most common type of benign tumor involving the nail is the verruca (either periungual or subungual in location) (Fig. 21). Acquired digital fibrokeratoma is a benign hyperplasia caused by trauma to the digits that clinically appears as firm, hyperkeratotic nodules impinging on the nail plate and causing a groovelike deformity similar to that seen with a mucoid cyst. It is also similar to the periungual fibroma seen in tuberous sclerosis (40). Periungual fibromas may be solitary and may also occur subungually (41). Pyogenic granuloma may be periungual or subungual (39) and may cause malformation of the nails in a fashion similar to a painful subungual glomus tumor, a small benign neoplasm of the skin and subcutaneous tissues, which may involve the nail bed (42). Benign bone cysts and tumors may also cause changes to the overlying nail bed and subsequently changes in the nail. In a similar effect, a distal phalanx aneurysmal bone cyst can cause secondary changes in the nail bed and the external appearance of the toenail (43). All these conditions may produce pain, and the patient may complain of discomfort in the subungual region, with or without a visible mass, before actual changes in the nail occur. Paronychia or nail plate deformity and discoloration may follow the subjective complaint of pain.
FIG. 21. Subungual and periungual verrucae of the hallux.
FIG. 22. Long-standing ulceration that was eventually diagnosed by biopsy as squamous cell carcinoma.
Malignant tumors that cause nail change are usually seen in the subungual region. Other clinical findings may include pain, swelling, and inflammation, and most patients have a history of chronic paronychia or trauma to the distal phalanx (44). Long-standing recalcitrant subungual ulcerations should be suspected to be possible squamous cell carcinoma (45) (Fig. 22). The prognosis is generally good, although squamous cell carcinoma of the skin occasionally metastasizes to the inguinal lymph nodes. This is much less of a problem with subungual squamous cell carcinoma. Punch biopsy diagnosis makes examination of such slow-healing ulcerations an atraumatic procedure and may preclude extensive growth of the lesion and permit early recognition and adequate removal (46).
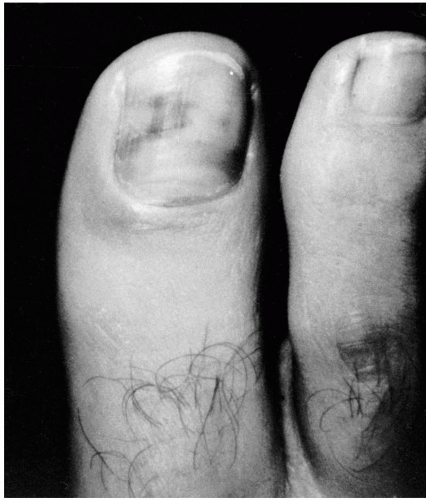
Malignant melanoma below the nail plate is not as damaging to the nail as are other types of malignant lesions. This particular malignant process is frequently misdiagnosed as a subungual hemorrhage; however, unlike flat lesions of malignant melanoma that develop slowly over years, the hemorrhagic subungual lesions develop quickly, and, in contradistinction to malignant melanomas, hemorrhagic lesions are usually uniformly deep black (47). In a series of 72 patients with subungual melanoma, nearly one-half gave a history of trauma, 65% of the lesions were either on the thumb or the great toe, and 36% had lymph node metastases at the time of surgery (48). In another series of 25 patients with subungual melanoma, the prognosis was poor. Only 36% of the patients were alive after 9 months, so the 5-year mortality rate was high (49).
Basal cell carcinoma is the least common cutaneous malignant disease involving the nail bed. Most cases of subungual basal cell carcinoma have been reported on the hand. As in the case of other malignant lesions, biologic behavior and resistance to treatment may be a clue to the ultimate diagnosis (50).
Bowen’s disease of the nail bed has been reported (51,52). These lesions are slow growing, with an insidious onset, and are different in appearance from Bowen’s disease on the skin (53). The lesion usually starts in the lateral nail fold and subsequently involves the nail bed, with secondary destructive changes of the nail plate. Mikhail in 1984 reported 21 cases of sublingual epidermoid carcinoma (which includes Bowen’s disease and invasive squamous cell carcinoma), which involved only a single case of squamous cell carcinoma of the hallux (54) (Fig. 23). He also reviewed the literature and found that of 113 cases there were 13 subungual lesions involving the toes.
Finally, any tumor under or about the nail should be suspected to be malignant whenever the patient has persistent infection, pain or swelling, or a visible mass that does not respond to standard therapeutic approaches. Radiographic and biopsy examination should be done as early as possible and repeatedly, if necessary, to provide an accurate diagnosis.
Biomechanical Abnormalities
One of the most frequent causes of ingrown toenails in children and adolescents is biomechanical imbalance. Onychocryptosis of the lateral nail margin of the hallux results from compression of the lateral nail fold between the hallux and the second digit. This forces the nail fold to overgrow the nail plate, causes the nail margin to become imbedded within the tissue, and results in pain and secondary infection. A similar problem occurs on the medial nail fold when the foot excessively pronates and weight is transferred through the great toe from lateral to medial (55). Abnormal dorsiflexion of the digits results in trauma to the hallux toenail and irritation to the dorsum of the lesser toes. As the hallux dorsiflexes, the distal phalanx is extended. The tip of the hallux contacts the shoe cap and traumatizes the hallux toenail, which thickens because of intermittent pressure.
FIG. 23. Bowen’s disease of the hallux nail plate.
FIG. 24. Ingrowing medial toenail with an incurvated nail plate secondary to laterally directed pressure on the medial hallux.
McGlamry (Doctors Hospital seminar notes, 1969) also reported a predictable pattern of onychocryptosis and onychoincurvatus resulting from the laterally directed pressures on the nails produced by wearing snug or tight-fitting hosiery (Fig. 24). This condition is especially noticeable with the use of snug elastic stockings and pantyhose. The normal care of the nail margins becomes difficult with this incurvation, and consequently keratinous debris accumulates beneath the nail and begins to decay, a situation that provides an ideal medium for the growth of microorganisms.
Hypertrophy of nail plates with massive thickening and yellow-brown discoloration
Dyskeratosis congenita
X-linked or autosomal dominant
Thinning of the nail plate, fusion with proximal nail fold, ridging, atrophy
Darier’s disease (Darier-White disease)
Autosomal dominant
Distal subungual wedge-shaped keratoses, longitudinal red and white striations, variable thickening and thinning, splinter hemorrhages, papules on proximal nail folds
DOOR syndrome (deafness onychoosteo-dystrophy, mental retardation)
Autosomal recessive
Absent or atrophic nails
Modified from Norton LA. Nail disorders. J Am Acad Dermatol 1980;2:451-467, with permission.
Only gold members can continue reading. Log In or Register to continue