Fig. 1.1
Irreversible flexion contracture of the knee, secondary to multiple hemarthroses. Note the posterior subluxation of the tibia associated with the problem
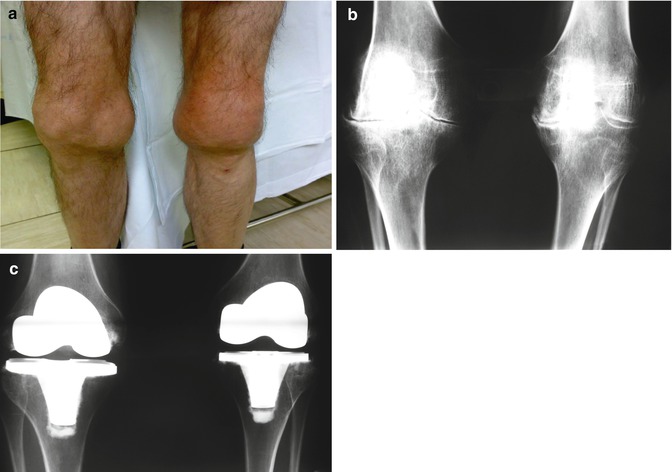
Fig. 1.2
Clinical appearance of severe hemophilic arthropathy in both knees (a) and the radiographic images confirming the joint disease (b). A bilateral total knee replacement was performed in two stages, with a satisfactory result (c)
The non-joint-related musculoskeletal problems in hemophilia, which account for over 10 % of orthopedic lesions in the patient with hemophilia, are essentially soft-tissue hematomas, muscle hematomas, and pseudotumors [4].
With adequate prophylaxis, at least from the age of 2–18 (ideally lifelong), it is possible to convert severe hemophilia into a moderate condition, considerably reducing (although not totally preventing) the associated musculoskeletal problems [5–7].
The main benefit of orthopedic surgery in hemophilia is that it markedly improves the patient’s quality of life [8]. This is achieved by appropriately managing the joint problems (hemophilic arthropathy) and the muscle hematomas and their complications (hemophilic pseudotumors, nerve paralysis caused by compression, and compartment syndrome) [7].
The level of evidence of hemophilia literature is very low. In fact, no study on the musculoskeletal complications of hemophilia has been included in the Cochrane Library so far. The aim of this chapter is to discuss the management of the musculoskeletal manifestations of hemophilia.
1.2 Management of Muscle Hematomas and Their Complications
1.2.1 Compartment Syndrome and Compression Neuropathy
Muscle hematomas can occur in any part of the body (Fig. 1.3) although the most common sites are the iliopsoas muscle and the flexor compartment of the forearm [4, 9]. If not adequately dealt with, they can lead to compartment syndrome and a possible need for urgent surgical decompression of the compartment [10]. Iliopsoas hematomas are often associated with paralysis of the crural nerve. It is important to remember that a right iliopsoas hematoma can be confused with appendicitis. The diagnosis of iliopsoas hematoma should be confirmed by ultrasound and/or computed tomography (CT). Crural nerve paralysis often requires rehabilitation for as long as 18 months before it fully resolves. Electromyography (EMG) is useful for the diagnosis and for assessing progress. Periodic ultrasounds are essential to confirm that the hematomas have been completely reabsorbed, and with the appropriate hematological treatment, this does usually occur. New bleeding, however, is common, and the treatment must therefore be continued for several weeks or even months until complete reabsorption is certain. Surgical decompression of the compartment is not appropriate for an iliopsoas bleed even if there is crural nerve involvement.

Fig. 1.3
Large hematoma in the right thigh of a hemophilia patient, anterior view (a) and posterior view (arrow) (b).
In the forearm, surgical opening of the entire flexor compartment may be necessary, since once compartment syndrome is established, it has a considerable effect on the function of the whole arm [4]. In some patients (particularly the immunosuppressed), a soft tissue hematoma can become spontaneously infected and turn into an abscess. Diagnosed early, this can generally be resolved with treatment based on intravenous antibiotics and surgical drainage.
1.2.2 Hemophilic Pseudotumors
Although rare, pseudotumors are a serious complication of hemophilia. They are progressive cyst-like inflammations that affect the muscles, caused by recurrent bleeding and associated with radiographic evidence of bone involvement [11–13]. Most pseudotumors are seen in adult patients and occur near the proximal ends of the long bones. However, they can occur distally in the wrist and ankle in young patients before skeletal maturity. If left untreated, proximal pseudotumors may destroy the soft tissues, erode the bone, and cause serious vascular and/or nerve damage.
Despite having a mortality rate of 20 %, the treatment of choice for proximal pseudotumors is surgical removal [11]. This mortality is primarily due to surgery. Regression, although not true cure, has been reported with long-term treatment with the deficient clotting factor and immobilization. This treatment should only be used in inoperable cases, such as patients with inhibitors who are poorly controlled. Percutaneous evacuation of the pseudotumor followed by filling with fibrin glue and/or cancellous bone can at times provide satisfactory results. Preoperative embolization of large pelvic pseudotumors may help to reduce intraoperative bleeding when removing surgically.
Distal pseudotumors can be controlled with hematological treatment and immobilization. It is important to be aware of the possibility of pseudotumors when one or more masses are detected in the limbs or pelvic region of a person with hemophilia. However, chondrosarcoma and liposarcoma have been confused with hemophilic pseudotumors in these patients [14]. Ultrasound, CT, and MRI (magnetic resonance imaging) will help to confirm the diagnosis in each case.
1.3 Management of Hemophilic Arthropathy
Hemophilic arthropathy is polyarticular (knees, ankles, elbows, hips, shoulders) and affects the patients from early childhood. Hemarthroses are accompanied by severe pain and an initially reversible antalgic flexion contracture. The blood within the joint alters chondrocyte (cartilage cells) proteoglycan synthesis, causing their death (apoptosis).
1.3.1 Hemarthrosis
Proper treatment of hemarthrosis should include early diagnosis, adequate hematological treatment, evacuation of the blood in the joint (arthrocentesis), physiotherapy, and prevention of new episodes of bleeding [7]. Clinical diagnosis should be confirmed by ultrasound. X-rays should also be performed to rule out (or confirm) radiological signs of joint disease.
A great deal of debate continues to surround the subject of joint aspiration (evacuation of the hemarthrosis or arthrocentesis) in hemophilia. Until very recently, it was considered to be extremely dangerous due to the high risk of new bleeding and infection (septic arthritis). My view is that major hemarthroses must be aggressively treated to prevent progression to synovitis and recurrent joint bleeds. However, there is no evidence of grade I in the literature confirming the role of arthrocentesis in the setting of hemarthrosis. The use of joint aspiration is more a matter of experience based in empirical data [4]. Therefore, we use arthrocentesis in acute and tense hemarthroses. The joint puncture must be done under tight hematological control and strict aseptic conditions [4].
Following arthrocentesis, it is recommended that the joint be immobilized for 3–5 days with a compression bandage. Ice should not be used for acute hemarthroses, as that seems controversial now [15]. The patient should then undergo a course of controlled physiotherapy, as rehabilitation is essential in order to prevent, as far as possible, chronic synovitis. The duration of the physiotherapy will depend on the time required for full recovery of joint mobility and muscle strength. Recurrent bleeding episodes must be avoided during the recovery period. Patients should be seen every 3 months in order to assess their progress closely.
1.3.2 Synovitis
Another problem is synovitis (synovial hypertrophy), caused by the cytokines and angiogenic factors from the intra-articular hemorrhage that stimulate the synovial cells to replicate, which eventually leads to a vicious circle of hemarthrosis-synovitis-hemarthrosis [3]. The circle must be broken by synovectomy. This may be medical or surgical. Medically, the best type is radiosynovectomy, the alternative being chemical synovectomy. Surgical synovectomy can be performed arthroscopically or by open surgery [16–20].
Short courses of intra-articular prednisone should be taken into account as an option prior to synovectomy [21].
Review of literature prior to 2002 showed no reports of malignancy related to 32P [22, 23]. However, in 2002 and 2009 two cases of acute lymphocytic leukemia (ALL) were reported after radiosynovectomy in two hemophilic children [23]. Given the short latency between exposure and diagnosis of ALL in both patients, the casual relationship between 32P exposure and ALL could not be firmly established. It is important to note, however, that there was also insufficient data to rule out causality.
Recently, a report of Infante-Rivard et al. demonstrated that there was no dose-response relationship with the amount of radioisotope administered or the number of radiosynovectomy treatments [19]. The study provided some indication for the safety of the procedure, but homogenous diagnostic groups of younger patients (such as hemophilic patients) receiving radiosynovectomy will need more evaluation.
The principal aim in hemophilia is, as far as possible, to prevent hemarthrosis before the synovitis can occur. Once developed, the aim is to treat it as early and aggressively as possible. The diagnosis should be confirmed by ultrasound or MRI (magnetic resonance imaging). Ultrasound is particularly useful for the knee, while MRI is more accurate for the elbow and the ankle. Nowadays power Doppler ultrasonography (US) is a very important tool for assessing knee bleeds [24, 25]. When conservative treatment, i.e., deficient clotting factor replacement therapy plus physiotherapy, fails to break the hemarthrosis-synovitis-hemarthrosis vicious circle, intervention is required to destroy the synovial membrane.
A medical synovectomy is simply the injection of a substance into the joint to “stabilize” the synovial membrane. The main reason for performing any type of synovectomy is the presence of an excessive amount of synovial membrane in a particular joint (hemophilic synovitis). We consider medical synovectomy the procedure of choice in cases of hemophilic synovitis with recurrent hemarthrosis, and that surgical synovectomy should only be used in cases where medical synovectomy has repeatedly failed. In view of its efficacy and minimal risk, medical synovectomy may also be used in patients with inhibitors [13, 14, 26].
The differential diagnosis between synovitis and hemarthrosis can, and should, be made by US and/or MRI. Plain X-rays are useful for assessing the degree of joint disease when deciding on synovectomy. It is logical to expect that the worse the synovitis, the more difficult it will be to resolve it by synovectomy. Indeed, in severe cases, multiple consecutive medical synovectomies can be necessary, and even then, surgical synovectomy may still be required.
The main indication for medical synovectomy is the presence of chronic hemophilic hypertrophic synovitis causing recurrent hemarthroses that do not respond to hematological treatment. The most commonly used these days are chemical synovectomy (rifampicin, oxytetracycline) and isotopic synovectomy or radiosynovectomy (with yttrium-90, phosphorus-32, or rhenium-186). In general, medical synovectomy has a 70 % efficacy rate, and it can be used at any point in the patient’s life; the main aim is to reduce the number and severity of hemarthroses and the damage the blood in the joint causes to the cartilage over the medium and long term.
Radiosynovectomy can be repeated if the first injection fails, up to three times at 6-month intervals if radioactive isotopes are used, or weekly, as many as 10–15 times if using rifampicin or oxytetracycline. Radiosynovectomy has been used worldwide for over 40 years, and no evidence has been found of any harm caused by the radioactive isotopes [27, 28]. In my opinion, assuming the isotopes are available, radiosynovectomy (with yttrium for knees and rhenium for elbows and ankles) is the procedure of choice in children aged over 12. We prefer rhenium for elbows and ankles because its therapeutic penetration power (1 mm) correlates well with the size of the synovium of medium-sized joints. However, in the knee we prefer yttrium because its therapeutic penetration power is 2.8 mm and it correlates well with the size of the knee synovium. Failing radiosynovectomy, rifampicin, and oxytetracycline are the alternatives (multiple, fairly painful, weekly injections are required for effective chemical synovectomy) [16–20].
Surgical synovectomy can be performed by open surgery or by arthroscopy. Most authors recommend arthroscopy [20, 29]. Once skeletal maturity has been reached, open surgery synovectomy may be indicated for the elbow, combined with resection of the radial head to improve pronation and supination of the elbow. In our center, we now always opt for radiosynovectomy with yttrium-90 (knees) or rhenium-186 (elbows and ankles) as the first option, and then if, after 2–3 radiosynovectomies at 6-month intervals, we have not managed to control the synovitis, we turn to surgical synovectomy (preferably arthroscopic) [26]. Prior radiosynovectomy does not lessen the chance for optimal response with surgical synovectomy (radiation does not cause fibrosis that makes complete resection difficult).
In terms of radiosynovectomy, our experience has confirmed a 70 % reduction in the mean rate of bleeds. Regarding pain and ROM, the rate of improvement is 70 % (statistically significant) and 3 % (not significant), respectively [18]. We use yttrium-90 (185 MBq, TPP-therapeutic penetration power of 2.8 mm) in the knees and rhenium-186 (TPP 1 mm) in the elbows (56–74 MBq) and ankles (74 Mbq). We have given over 400 injections to date (1–3 per patient, at 6-month intervals). The risk of complications is 1.5 % (four inflammatory responses, one mild radiation burn to the skin, one septic arthritis of the knee). Radiosynovectomy is our first option for the treatment of synovitis (450 euros per injection), with arthroscopic synovectomy as second-line treatment (4,500 euros). We opt for arthroscopic synovectomy after the failure of three attempts at radiosynovectomy at 6-month intervals. So far, only 3.5 % of patients have required this technique [18].
1.3.3 Advanced Joint Disease
The literature seems to support the use of the intra-articular injections of hyaluronic acid (so-called viscosupplementation) in the treatment of knee osteoarthritis, because it diminishes pain and improves disability, generally within 1 week and for up to 3–12 months (but especially at the 5–13-week postinjection period). There are only five reports in the literature on the efficacy of knee viscosupplementation in hemophilia, all of them with a low level of evidence [30]. The five studies dealing with viscosupplementation in hemophilia recommend it for hemophilic arthropathy of the knee as a way of delaying the need of operative treatment when noninvasive medical therapy (relative rest, oral anti-inflammatory drugs, oral analgesics, and physical therapy) has failed. My view is that the short-lived improvement afforded by viscosupplementation does not seem to warrant its use in hemophilic patients given the risks and the cost involved. Further trials are required to ascertain whether viscosupplementation should be indicated in painful radiological hemophilic arthropathy of the knee [30].
When the extent of joint involvement progresses as a result of the joint bleeds being impossible to control, patients will not only develop certain joint deformities and contractures but also subchondral cysts and osteophytes. Valgus deformity of the knee and the ankle is common, while the most typical in the elbow is hypertrophy of the radial head. Hemophilia patients may therefore present with valgus flexion deformities in one or both knees, equinus (Fig. 1.4) in one or both ankles, and in one or both elbows in flexion. Osteotomy is often necessary on the knee and ankle to correct the poor joint alignment [31].

Fig. 1.4
Severe equinus deformity of the ankle in a patient with hemophilia
Flexion contractures are common in hemophilia and difficult to resolve once they become fixed. The joints most affected are the elbows, knees, and ankles. The contracture is initially antalgic and is related to a hemarthrosis, which means that within the first few weeks, the contracture can be resolved with the appropriate treatment (hematological treatment plus rehabilitation) [32]. The deformity will subsequently become fixed, with the resulting negative effects on function, and may even require surgery. In the knee, lengthening of the tendons in the popliteal fossa (hamstrings release) combined with a posterior capsulotomy or supracondylar extension osteotomy may correct the flexion deformity. In the ankle, Z-lengthening of the Achilles tendon may also be necessary [4].
In the hip, patients may develop a disease similar to Perthes disease in relation to the recurrent joint bleeds. Perthes is a condition in children characterized by a temporary loss of blood supply to the hip. Without an adequate blood supply, the rounded head of the femur dies. The area becomes intensely inflamed and irritated. Perthes is really a complex process of stages. Treatment of Perthes may require periods of immobilization or limitations on usual activities. The long-term prognosis is good in most cases. After 18 months to 2 years of treatment, most children return to normal activities without major limitations. Perthes disease usually is seen in children between 4 years and 10 years of age. It is five times more common in boys than in girls. Initial treatment is with an abduction orthosis, thereby making surgery rarely necessary (varus osteotomy of neck of the femur). Juxta-articular cysts are also common and, when large and symptomatic, may require curettage and filling with bone graft, with or without fibrin glue. The formation of large anterior osteophytes is common in the ankle, and when symptomatic, surgical excision may be necessary.
Many hemophilia patients under the age of 40, and as young as 10, already have severe joint damage (advanced joint disease). At this point, the possible treatments are radial head resection, total hip replacement, arthroscopic debridement of the knee, total knee replacement (TKR), and ankle arthrodesis [4]. When there is multiple joint involvement, operating on only one joint may not improve the patient’s overall functioning, and our objective should therefore be to achieve one functional limb. It is recommended in hemophilia that multiple joint interventions be done in one single operation, since the complication rate is lower than would be expected and the rehabilitation time after multiple-joint surgery is relatively short [33].
In the elbow, radial head resection tends to reduce the number of joint bleeds and improve the degree of pronation and supination. Elbow deformity can cause ulnar nerve damage, which may require surgical neurolysis (release) [34, 35].
In the hip, the best solution is total hip replacement (THR). A spontaneously ankylosed hip can even be converted into a prosthesis, with the aim of improving the severe low back and knee pain suffered by patients with an ankylosed hip [36, 37].
In the knees, if the patient is very young and has a long life expectancy, it may be worthwhile debriding arthroscopically in order to relieve the pain for a few years [38]. If the arthroscopic knee debridement fails, TKR may be an option [39–47]. THR and TKR appear to last longer in people with hemophilia than in people of a similar age with osteoarthritis [45]. It is evident that in the age of joint replacement, hip and knee replacement should be offered to the hemophilia patient with massive joint damage associated with severe pain and marked functional disability. Nonetheless, the surgeon and the patient must weigh up the risks and benefits (especially if the patient is severely immunosuppressed).
Related posts:
 Hematological Concepts and Hematological Perioperative Treatment
Hematological Concepts and Hematological Perioperative Treatment
 Shoulder Surgery in Hemophilia
Shoulder Surgery in Hemophilia
 Orthopedic Surgery in Hemophilia: Is Thromboprophylaxis Necessary?
Orthopedic Surgery in Hemophilia: Is Thromboprophylaxis Necessary?
 Pharmacoeconomics of Orthopedic Surgery in Hemophilia
Pharmacoeconomics of Orthopedic Surgery in Hemophilia
 Advanced Hemophilic Arthropathy of the Ankle: Total Ankle Replacement or Ankle Fusion?
Advanced Hemophilic Arthropathy of the Ankle: Total Ankle Replacement or Ankle Fusion?
 Imaging of the Hemophilic Joints
Imaging of the Hemophilic Joints
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


