Miscellaneous Unusual Tumors of Bone
This chapter is concerned with some uncommonly rare tumors of bone. Some of these are included in the classification of bone tumors (see Chapter 1) and some are not. This includes neural and fatty tumors discussed in Chapters 25 and 26, respectively, of the previous edition of this book.
SCHWANNOMA
Neurogenic tumors of bone are rare. In a review of the English-language literature in 1992, Turk and coauthors found 79 examples of intraosseous schwannoma (neurilemmoma). Neurofibromas should be distinguished from schwannomas because the latter have practically no potential for malignant transformation. The differentiation is usually straightforward: schwannomas are well-circumscribed masses arising from a nerve, whereas neurofibromas are usually fusiform and course along the nerve.
In approximately half of the large group of cases studied at Mayo Clinic by Hunt and Pugh in 1961, neurofibromatosis was associated with various skeletal changes. These changes included erosive effects in bone caused by contiguous neurogenic tumors, dysplasia of vertebral bodies with scoliosis, defects of the posterior orbital wall, congenital bowing, and pseudarthrosis. Intraoasseous neurofibromas are distinctly rare. Some of the osseous defects noted in patients with von Recklinghausen disease have been coincidental, unrelated processes.
Malignant peripheral nerve sheath tumors have rarely been described arising in bone, and evidence in reported cases is not altogether convincing. The inherent characteristics of a malignant growth make it difficult to verify the exact tissue of origin in a questionable case. Growth in relation to a nerve is important in establishing the neurogenic origin of a sarcoma. In any event, the problem is academic because the treatment for such a sarcoma would be the same as for fibrosarcoma of bone. In the Mayo Clinic files, four patients with von Recklinghausen disease had spindle cell sarcoma of the bone. Although the lesions in these cases may represent malignant peripheral nerve sheath tumors, there is no proof of their neurogenic nature, and they have been included with fibrosarcomas.
INCIDENCE
Schwannoma is a rare primary bone tumor. In the Mayo Clinic series, the 23 cases accounted for less than 1% of the primary benign tumors of bone (Fig. 25.1).
SEX
Thirteen of the twenty-three patients were females.
AGE
A wide age range was represented, but 11 of the 23 patients were in the second and third decades of life.
LOCALIZATION
The mandible and the sacrum were the most commonly involved bones, accounting for six and nine tumors, respectively. Schwannomas are not uncommon in the region of the sacrum. Quite often, it is impossible to know whether the lesion arose from the sacrum or from one of the nerves and eroded the bone secondarily. A case was included only if the radiographic features suggested that the tumor was a primary neoplasm of bone. Three lesions were in the skull, two in the mid femur, and one each in the rib, distal tibia, and scapula. The literature suggests a pronounced predilection for involvement of the mandible.
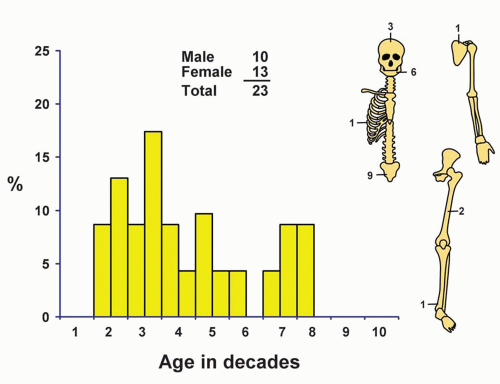 Figure 25.1. Distribution of schwannomas according to age and sex of the patient and site of the lesion. |
SYMPTOMS
Many schwannomas of bone are asymptomatic, a few produce prominent pain, and some result in local tumefaction.
PHYSICAL FINDINGS
There are no specific physical findings unless a patient has neurofibromatosis.
RADIOGRAPHIC FEATURES
Well-defined cystlike rarefactions, sometimes with a slightly sclerotic border, are produced by schwannomas. When in a long tubular bone, these rarefactions are typically in the shaft and often near its end. The defect sometimes has a bubbly appearance because of the irregular corrugations in the wall of the cavity that houses the lesion (Figs. 25.2, 25.3, 25.4 and 25.5).
GROSS PATHOLOGIC FEATURES
Material removed from a schwannoma of bone, like that of its soft-tissue counterpart, is a relatively firm mass of fibroblastic tissue. It may be somewhat gelatinous or myxoid, and a yellow or brownish discoloration is occasionally present. The relationship to a nerve or its canal,
if such can be established, is an important diagnostic clue. The lesion may be partially cystic (Fig. 25.5).
if such can be established, is an important diagnostic clue. The lesion may be partially cystic (Fig. 25.5).
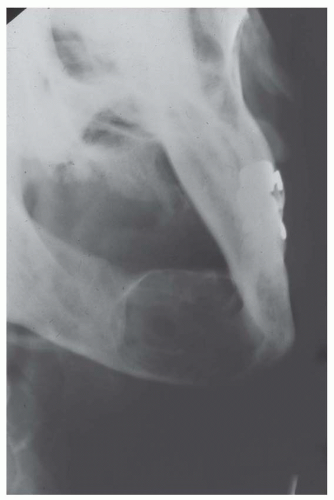 Figure 25.2. Schwannoma involving the mandible produces a well-defined expansile lucency. The lesion is surrounded by a sclerotic rim, suggesting a benign process. |
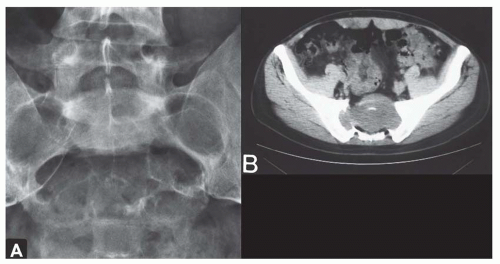 Figure 25.3. Schwannoma. Lesion of the sacrum in a 40-year-old man who had experienced back pain for 2 years. A: Plain radiograph shows a large lytic mass. Sharp margination, sclerotic rim, and foraminal expansion favor a benign neurogenic process. B: Computed tomogram shows clearly that the lesion arose from within the bone. |
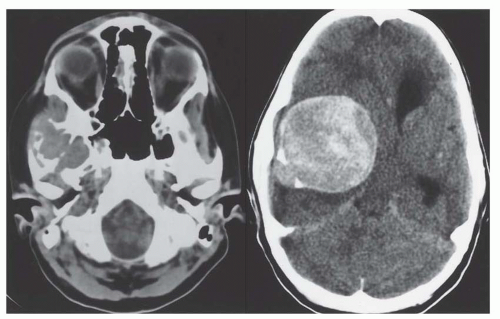 Figure 25.4. Computed tomograms at two levels show a large schwannoma involving the temporal bone in a 12-year-old girl. |
HISTOPATHOLOGIC FEATURES
Schwannomas are well-circumscribed lesions, and the edges are sharply demarcated from surrounding bone. There is no invasion of surrounding medullary bone. The lesion is essentially a spindle cell process, which may be quite vascular. Typically, the vessels have a thick hyaline wall. The spindle cells have a very characteristic wavy nucleus, and nuclear palisading may be prominent (Figs. 25.6 and 25.7). Areas of foam cells and hemosiderin pigment are commonly seen. As with schwannomas of soft-tissue localization, the nuclei may be irregular in size, dark staining, and bizarre, probably because of degeneration. Although these nuclei are suggestive of a malignant tumor, the virtual absence of mitotic figures and the benign radiographic appearance indicate the benign quality of the neoplasm.
 Figure 25.5. Schwannoma forming an expansile benign-appearing lesion in the distal fibula in a 50-year-old man. |
TREATMENT
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


