Fig. 3.1
(a–d) Puncture needle biopsy in cervical spine in a patient with metastatic carcinoma. In cases like this, fine needle or core needle biopsy is undoubtedly a better alternative than surgical biopsy
Fig. 3.2
(a) Fine needle biopsy in a lytic lesion of the sacrum. (b and c) Paraffin-embedded small blood clots clearly show a chordoma
Fig. 3.3
(a) Infrequent location of a solitary myeloma. The smear (b) and paraffin-embedded blood clots (c) establish the diagnosis of myeloma
Fig. 3.4
(a) Lytic lesion of the upper end of a humerus. (b) CT-guided puncture needle biopsy. (c) Low magnification of fragment including osteosclerotic margin and the tumoral lesion. (d) At high magnification, a diagnosis of chondroblastoma was made
Fig. 3.5
(a) Core needle biopsy of an osteosarcoma of femur. (b) Microphotograph of the cylinder. (c) The smear shows pleomorphic cellularity
Fig. 3.6
(a) Giant cell tumor in the lower epiphysis of femur. (b) CT-guided core needle biopsy. (c) Microphotograph at low magnification showing bone cylinder and blood clots. (d) The bone cylinder contains no lesion. (e) In a small blood clot, it is possible to identify a fragment of the lesion corresponding to giant cell tumor
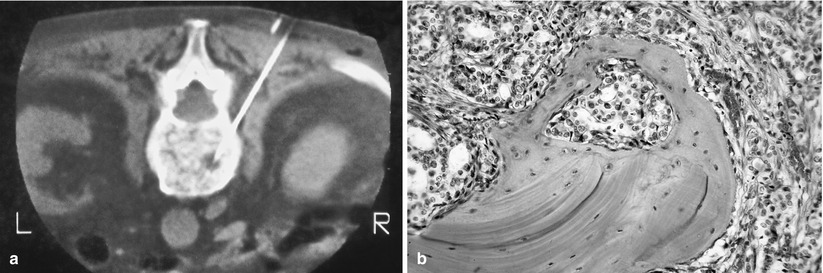
Fig. 3.7




(a and b) Puncture needle biopsy in a vertebral body affected by adenocarcinoma metastasis. In small lesions, the use of CT-guided biopsy is useful to obtain representative specimen
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
